- Schistosomiasis (bilharziasis)

Содержание
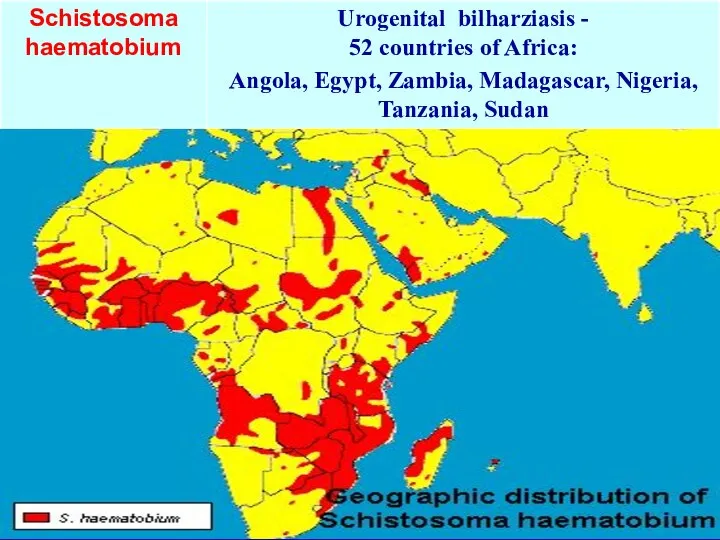
- 2. Schistosomiasis - infectious diseases caused by a group of tropical parasites with a primary lesion of
- 3. Schistosomes are prevalent in rural and outlying city areas of 74 countries in Africa, Asia and
- 4. It is difficult to know how many individuals die of schistomiasis each year because death certificates
- 5. 1851 - Bilharz opened pathogen of urinary schistosomiasis. 1898 - Manson described the causative agent of
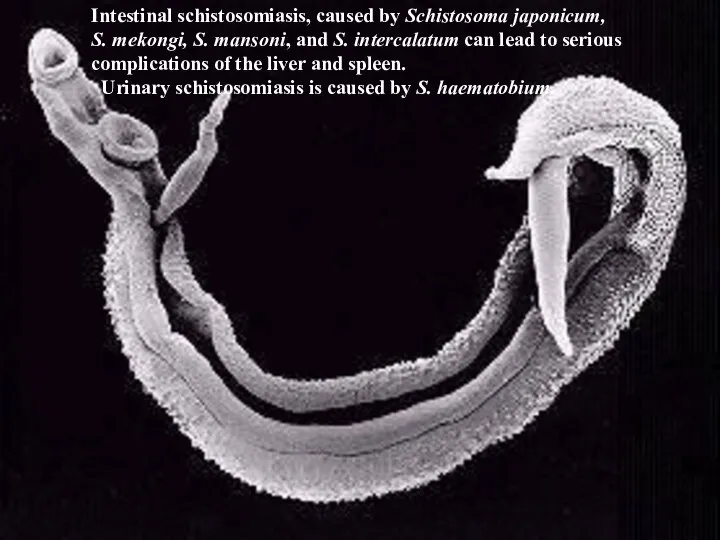
- 9. Intestinal schistosomiasis, caused by Schistosoma japonicum, S. mekongi, S. mansoni, and S. intercalatum can lead to
- 10. Source of the infection: S. mansoni, and S. intercalatum - human, rats, monkey S. mekongi –
- 11. Eggs are excreted in human urine and feces in areas with poor sanitation, contaminate freshwater sources.
- 12. Mature male and female worms pair and migrate to the intestine or the bladder where egg
- 15. ADULT PARASITES DO NOT GO OUT FROM THE BODY OF A HUMAN OR ANIMAL From penetration
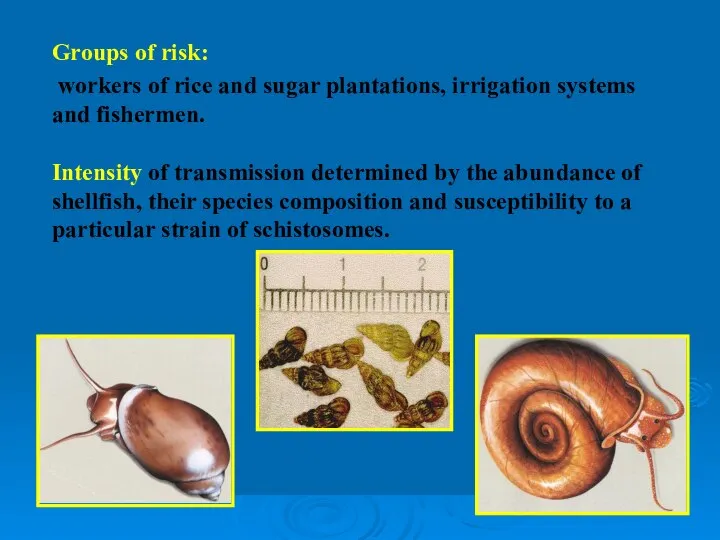
- 16. Groups of risk: workers of rice and sugar plantations, irrigation systems and fishermen. Intensity of transmission
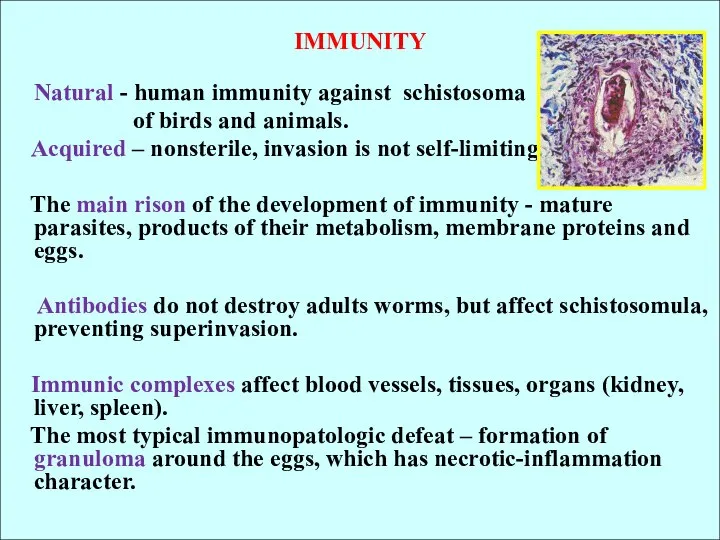
- 17. IMMUNITY Natural - human immunity against schistosoma of birds and animals. Acquired – nonsterile, invasion is
- 18. PATHOGENESIS 1. Sensitization of the organism by toxic products of schistosomula and cercariae. 2. Migration of
- 19. CLINICAL CLASSIFICATION (WHO) 1. Stage of infection (invasion) - penetration phase - migration phase 2. Stage
- 20. 1. Stage of infection: Penetration phase (5-6 days): in primary infection may be asymptomatic, in re-infections
- 21. 2. Stage of maturation (Japanese sch. - 4 weeks, Mansony sch.-5 weeks, urogenital sch. -8-10 weeks):
- 22. 3.Stage of impending invasion (3-7 years): Common to all types of schistosomiasis: - intensive production of
- 23. Intestinal schistosomiasis: characterized by lesions of large intestine (eggs pass through the wall), the liver and
- 24. Stage of late invasion: - Simmer’s fibrosis (fibrosis around the the portal vein) - liver is
- 25. Japanese schistosomiasis: 1. The worms produce the maximum number of eggs (up to 3,000), 2. Necrosis
- 26. LABORATORY DIAGNOSTICS: 1. Microscopic detection of eggs in the urine (after physical exertion), faeces (method of
- 27. 5. Clinical methods – X-ray examination of the bladder, lungs, esophagus, stomach, angiography, biochemical, and laparoscopy.
- 30. PREVENTION 1. Straggle with the intermediate hosts - mollusks (chemical method and biological methods - bacteria,
- 32. Скачать презентацию
Schistosomiasis - infectious diseases caused by a group of tropical
Schistosomiasis - infectious diseases caused by a group of tropical
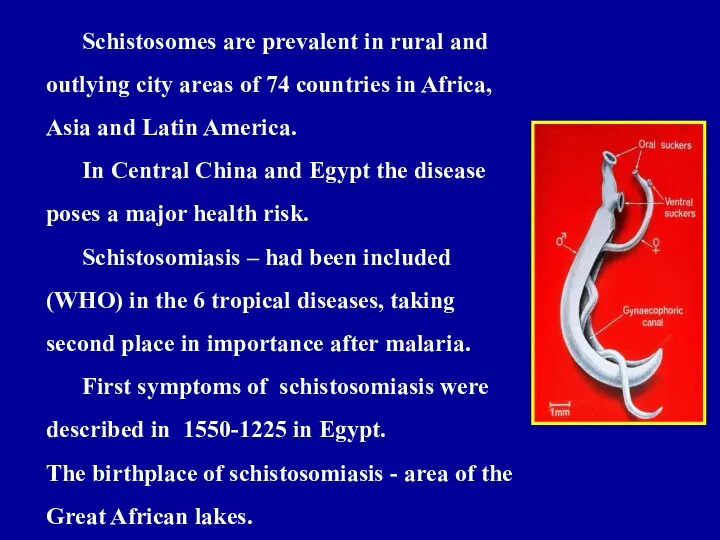
Schistosomes are prevalent in rural and outlying city areas of 74
Schistosomes are prevalent in rural and outlying city areas of 74
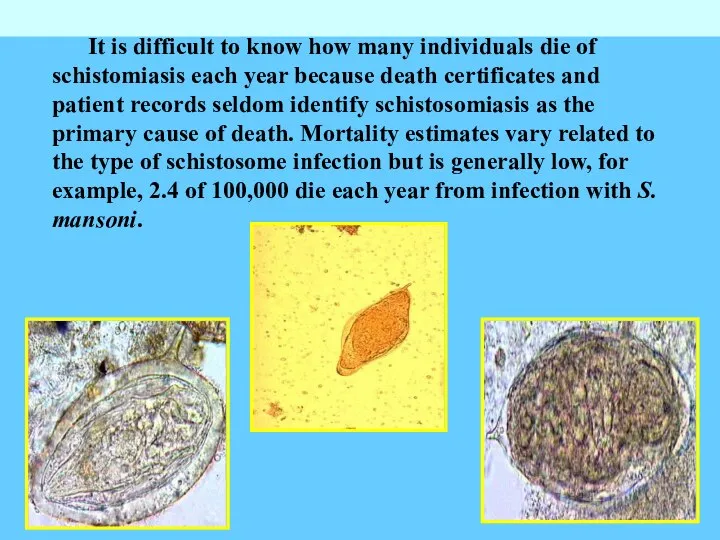
It is difficult to know how many individuals die of schistomiasis
It is difficult to know how many individuals die of schistomiasis
1851 - Bilharz opened pathogen of urinary schistosomiasis.
1898 - Manson
1851 - Bilharz opened pathogen of urinary schistosomiasis. 1898 - Manson


Intestinal schistosomiasis, caused by Schistosoma japonicum,
S. mekongi, S. mansoni, and
Intestinal schistosomiasis, caused by Schistosoma japonicum,
S. mekongi, S. mansoni, and

Source of the infection:
S. mansoni, and S. intercalatum - human, rats,
Source of the infection: S. mansoni, and S. intercalatum - human, rats,

Eggs are excreted in human urine and feces in areas with
Eggs are excreted in human urine and feces in areas with

Mature male and female worms pair and migrate to the intestine
Mature male and female worms pair and migrate to the intestine



ADULT PARASITES DO NOT GO OUT FROM THE BODY OF A
Groups of risk:
workers of rice and sugar plantations, irrigation systems
Groups of risk:
workers of rice and sugar plantations, irrigation systems
IMMUNITY
Natural - human immunity against schistosoma
of birds and animals.
Natural - human immunity against schistosoma
of birds and animals.
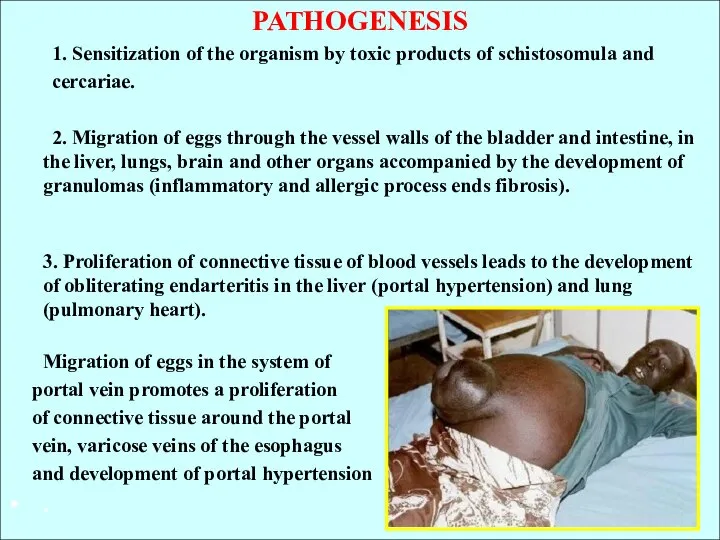
PATHOGENESIS
1. Sensitization of the organism by toxic products of schistosomula
PATHOGENESIS
1. Sensitization of the organism by toxic products of schistosomula
CLINICAL CLASSIFICATION (WHO)
1. Stage of infection (invasion)
- penetration phase
-
- penetration phase
-
1. Stage of infection:
Penetration phase (5-6 days):
in primary infection
1. Stage of infection:
Penetration phase (5-6 days):
in primary infection
2. Stage of maturation
(Japanese sch. - 4 weeks, Mansony sch.-5
2. Stage of maturation
(Japanese sch. - 4 weeks, Mansony sch.-5
3.Stage of impending invasion (3-7 years):
Common to all types of schistosomiasis:
-
Common to all types of schistosomiasis:
-
Intestinal schistosomiasis:
characterized by lesions of large intestine (eggs pass through the
Intestinal schistosomiasis:
characterized by lesions of large intestine (eggs pass through the
Stage of late invasion:
- Simmer’s fibrosis (fibrosis around the the portal
Stage of late invasion:
- Simmer’s fibrosis (fibrosis around the the portal
Japanese schistosomiasis:
1. The worms produce the maximum number of eggs (up
1. The worms produce the maximum number of eggs (up

LABORATORY DIAGNOSTICS:
1. Microscopic detection of eggs in the urine (after physical
1. Microscopic detection of eggs in the urine (after physical
5. Clinical methods – X-ray examination of the bladder, lungs, esophagus,
5. Clinical methods – X-ray examination of the bladder, lungs, esophagus,


 Блокаторы гистаминовых H2 -рецепторов
Блокаторы гистаминовых H2 -рецепторов Физиотерапевтическое лечение детей со SMA
Физиотерапевтическое лечение детей со SMA Убеждающая презентация. Власть слова, тренинг навыков публичного выступления
Убеждающая презентация. Власть слова, тренинг навыков публичного выступления Профилактика ОРВИ и гриппа
Профилактика ОРВИ и гриппа Болезни кишечника
Болезни кишечника Гепатит. Лабараторлы инструментальді диагностикасы
Гепатит. Лабараторлы инструментальді диагностикасы Этико-правовое регулирование медико-биологических экспериментов. Биоэтические проблемы прокреации
Этико-правовое регулирование медико-биологических экспериментов. Биоэтические проблемы прокреации Артықшылықты режим. Науқастардың санаттары
Артықшылықты режим. Науқастардың санаттары Лечение острого коронарного синдрома. Консервативная стратегия
Лечение острого коронарного синдрома. Консервативная стратегия Угрозы по телефону
Угрозы по телефону Патология ВНД. Неврозы
Патология ВНД. Неврозы Профилактика гриппа и ОРВИ
Профилактика гриппа и ОРВИ Физическая реабилитация при ампутации конечностей
Физическая реабилитация при ампутации конечностей Факторы, предрасполагающие к развитию тазового предлежания и пути их разрешения
Факторы, предрасполагающие к развитию тазового предлежания и пути их разрешения Психогимнастика в работе с детьми. Цели, технологии и результаты
Психогимнастика в работе с детьми. Цели, технологии и результаты Высшие психические процессы
Высшие психические процессы Третичный период сифилиса
Третичный период сифилиса Диагностика при ЧМТ
Диагностика при ЧМТ О ключевых показателях вакцинации против новой коронавирусной инфекции в Республике Карелия 08.12.2021
О ключевых показателях вакцинации против новой коронавирусной инфекции в Республике Карелия 08.12.2021 Проблемы морального и эмоционального развития в дошкольном возрасте
Проблемы морального и эмоционального развития в дошкольном возрасте Тупая травма живота
Тупая травма живота Принципы организации медицины катастроф
Принципы организации медицины катастроф Повреждения: некроз. Атрофия.апоптоз
Повреждения: некроз. Атрофия.апоптоз Личная гигиена. Гигиена кожи, одежды
Личная гигиена. Гигиена кожи, одежды Поиск клинико-практического руководства по ХОБЛ по базам электронных ресурсов
Поиск клинико-практического руководства по ХОБЛ по базам электронных ресурсов Синдром боли в животе
Синдром боли в животе Гетерохромный циклит Фукса
Гетерохромный циклит Фукса Преэклампсияның ауыр дәрежесінде жедел көмек көрсетудің алгоритмі
Преэклампсияның ауыр дәрежесінде жедел көмек көрсетудің алгоритмі