- Tertiary, visceral syphilis, neurosyphilis

Содержание
- 2. General progress of tertiary syphilis. Classification of tertiary syphilis 1. It develops only in a very
- 3. General progress of tertiary syphilis. Classification of tertiary syphilis 8. Localization in essential organs can lead
- 4. Tubercular syphilid 1. grouped 2. serpiginous (creeping) 3. platform (field) 4.dwarf (small)
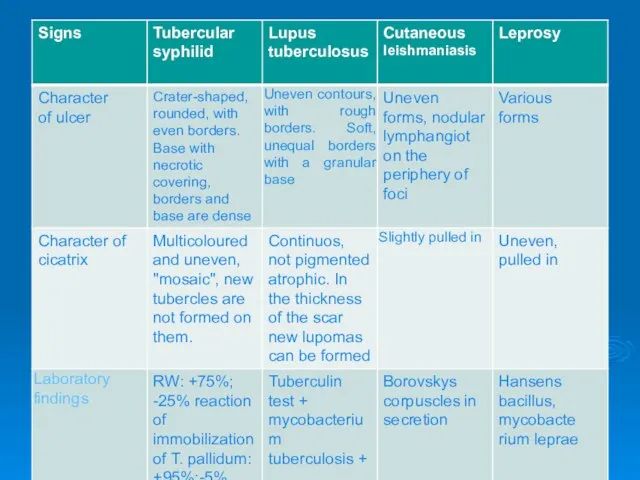
- 5. Diagnosis of tubercular and tubercular-ulcer syphilid is based on the following characteristic features a) dense infiltrate
- 8. Gummatous syphilid gumma is a sharply separated dense spherical or flat node. lying deeply under the
- 9. Gummatous syphilid Size: pea-sized, slowly increases to size of a nut; painless; movable: the skin on
- 10. Gummatous syphilid On the base of the ulcer of dead tissue (gummatous shaft), the ulcer undergoes
- 11. Latent syphilis (syphilis latens) The following information may be of assistance in the diagnosis of this
- 13. Latent syphilis (syphilis latens) The following information facilitates the diagnosis of late latent syphilis: the medical
- 14. Congenital syphilis Transmission of congenital syphilis The most common theory is that the only way of
- 15. Syphilis of the placenta Pay attention to the size, weight, colour of the placenta. Explain the
- 16. Syphilis of the fetus The infection of the parenchymal organs and fetus has a character of
- 17. Syphilis of the infants The development of congenital syphilis has a unique character. Syphilis in children
- 18. Syphilis of the infants Fig. 1, 2. Syphilitic pemphigus Fig. 3. Diffused papular infiltrate Gochzingers.
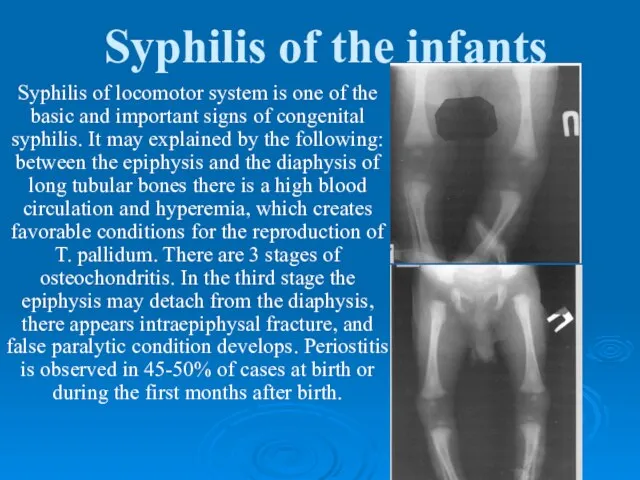
- 19. Syphilis of the infants Syphilis of locomotor system is one of the basic and important signs
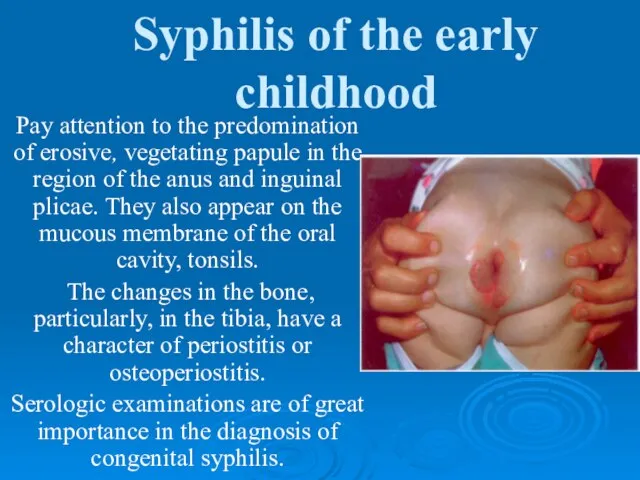
- 20. Syphilis of the early childhood At the beginning of the second half of the first year
- 21. Syphilis of the early childhood Pay attention to the predomination of erosive, vegetating papule in the
- 22. Late congenital syphilis Signs of the late congenital syphilis are divided into unconditional and accessory signs.
- 23. Late congenital syphilis Accessory signs include: dystrophy of teeth; infection of locomotor system (saber shin crus),
- 25. Late congenital syphilis The following stigmata of late congenital syphilis are the most significant: 1) Avsitidiisky's
- 27. Скачать презентацию
General progress of tertiary syphilis. Classification of tertiary syphilis
1. It develops
General progress of tertiary syphilis. Classification of tertiary syphilis
1. It develops
General progress of tertiary syphilis. Classification of tertiary syphilis
8. Localization in
General progress of tertiary syphilis. Classification of tertiary syphilis
8. Localization in
Tubercular syphilid
1. grouped
2. serpiginous (creeping)
3. platform (field)
4.dwarf (small)
Tubercular syphilid
1. grouped
2. serpiginous (creeping)
3. platform (field)
4.dwarf (small)
Diagnosis of tubercular and tubercular-ulcer syphilid is based on the following
Diagnosis of tubercular and tubercular-ulcer syphilid is based on the following

Gummatous syphilid
gumma is a sharply separated dense spherical or flat node.
lying
Gummatous syphilid
gumma is a sharply separated dense spherical or flat node.
lying
Gummatous syphilid
Size:
pea-sized,
slowly increases to size of a nut;
painless;
movable:
Gummatous syphilid
Size:
pea-sized,
slowly increases to size of a nut;
painless;
movable:
Gummatous syphilid
On the base of the ulcer of dead tissue (gummatous
Gummatous syphilid
On the base of the ulcer of dead tissue (gummatous
Latent syphilis (syphilis latens)
The following information may be of assistance
Latent syphilis (syphilis latens)
The following information may be of assistance

Latent syphilis (syphilis latens)
The following information facilitates the diagnosis of late
Latent syphilis (syphilis latens)
The following information facilitates the diagnosis of late
Congenital syphilis
Transmission of congenital syphilis
The most common theory is that the
Congenital syphilis
Transmission of congenital syphilis
The most common theory is that the
Syphilis of the placenta
Pay attention to the size, weight, colour of
Syphilis of the placenta
Pay attention to the size, weight, colour of
Syphilis of the fetus
The infection of the parenchymal organs and fetus
Syphilis of the fetus
The infection of the parenchymal organs and fetus
Syphilis of the infants
The development of congenital syphilis has a unique
Syphilis of the infants
The development of congenital syphilis has a unique

Syphilis of the infants
Fig. 1, 2. Syphilitic pemphigus
Fig. 3. Diffused papular
Syphilis of the infants
Fig. 1, 2. Syphilitic pemphigus
Fig. 3. Diffused papular
Syphilis of the infants
Syphilis of locomotor system is one of the
Syphilis of the infants
Syphilis of locomotor system is one of the
Syphilis of the early childhood
At the beginning of the second half
Syphilis of the early childhood
At the beginning of the second half
Syphilis of the early childhood
Pay attention to the predomination of erosive,
Syphilis of the early childhood
Pay attention to the predomination of erosive,
Late congenital syphilis
Signs of the late congenital syphilis are divided into
Late congenital syphilis
Signs of the late congenital syphilis are divided into
Late congenital syphilis
Accessory signs include:
dystrophy of teeth;
infection of locomotor system
Late congenital syphilis
Accessory signs include:
dystrophy of teeth;
infection of locomotor system

Late congenital syphilis
The following stigmata of late congenital syphilis are the
Late congenital syphilis
The following stigmata of late congenital syphilis are the
 Применение Су-Джок терапии при работе с детьми с ОВЗ
Применение Су-Джок терапии при работе с детьми с ОВЗ Фармацевтическая компания Эвалар
Фармацевтическая компания Эвалар Пузырные и вирусные дерматозы
Пузырные и вирусные дерматозы Мораль и нравственность. Добро и зло
Мораль и нравственность. Добро и зло Психология детей с нарушениями эмоциональноволевой сферы и поведения. Лекция 1
Психология детей с нарушениями эмоциональноволевой сферы и поведения. Лекция 1 Лечение гастроэзофагеальной рефлюксной болезни у пациентов с хроническими заболеваниями органов дыхания
Лечение гастроэзофагеальной рефлюксной болезни у пациентов с хроническими заболеваниями органов дыхания Использование прибора. 经络通仪的操作流程
Использование прибора. 经络通仪的操作流程 Микроскопическое исследование осадка мочи. Часть 2
Микроскопическое исследование осадка мочи. Часть 2 Шевчук, заболевание глаз
Шевчук, заболевание глаз Металлокерамикалық көпір тәрізді протездермен емдеу
Металлокерамикалық көпір тәрізді протездермен емдеу Чувствительность и её нарушения
Чувствительность и её нарушения Легочное сердце
Легочное сердце Вирус полиомиелита
Вирус полиомиелита Здоровое питание педагога
Здоровое питание педагога Развитие зародыша и плода
Развитие зародыша и плода Новый тип коронавируса. Опасность рядом
Новый тип коронавируса. Опасность рядом Ich will mich gegen corona impfen las
Ich will mich gegen corona impfen las Угрозы здоровью населения планеты в 2019 году
Угрозы здоровью населения планеты в 2019 году Хронічна ниркова недостатність. Гостра ниркова недостатність
Хронічна ниркова недостатність. Гостра ниркова недостатність Покрытие таблеток оболочками
Покрытие таблеток оболочками Синдром артериальной гипертензии. Лекция 2009
Синдром артериальной гипертензии. Лекция 2009 Тренинг креативности
Тренинг креативности Сестринский уход за пациентами с заболеваниями глаз
Сестринский уход за пациентами с заболеваниями глаз Эпикардиальное ожирение и его роль в развитии метаболического синдрома
Эпикардиальное ожирение и его роль в развитии метаболического синдрома Правила проведения доклинического исследования лекарственного средства для ветеринарного применения, клинического исследовани
Правила проведения доклинического исследования лекарственного средства для ветеринарного применения, клинического исследовани Герпесвирусная инфекция
Герпесвирусная инфекция Современный научный подход в построении тренировочного процесса для развития основных физических качеств военнослужащих
Современный научный подход в построении тренировочного процесса для развития основных физических качеств военнослужащих Тік ішектің және артқы өтістің аурулары. Жалпы тәжірбиелік дәрігер тактикасы. Тәжірбиені меңгеру
Тік ішектің және артқы өтістің аурулары. Жалпы тәжірбиелік дәрігер тактикасы. Тәжірбиені меңгеру