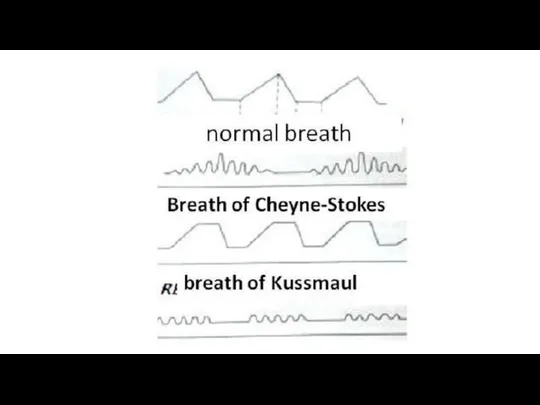
- Symptoms of respiratory system diseases. Lection 2-3

Содержание
- 2. Physical examination General inspection Cyanosis (diffuse, warm) – respiratory failure Hyperemia of the face and upper
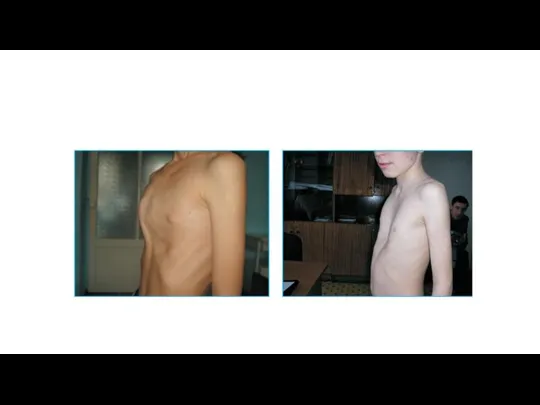
- 3. 2. Examination of the chest 1)The shape of the chest normal (asthenic, normo- and hypersthenic) pathological
- 5. 4) The position of the clavicles, supra- and subclavian fossae, the state of the intercostal spaces:
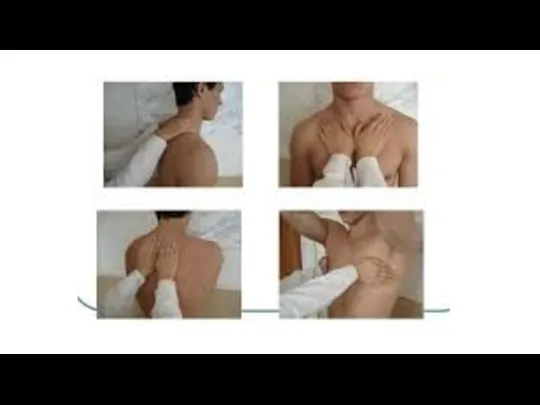
- 7. 3. Palpation of the chest Objectives Assess pain Determine the resistance of the chest Study the
- 8. Voice vibration palpation sensation of chest vibration when pronouncing individual words containing the sound R-R (tractor)
- 10. Basic pathology of the lung
- 11. Pulmonary emphisema / Эмфизема легких - increased airiness of the lungs
- 12. Норма Эмфизема
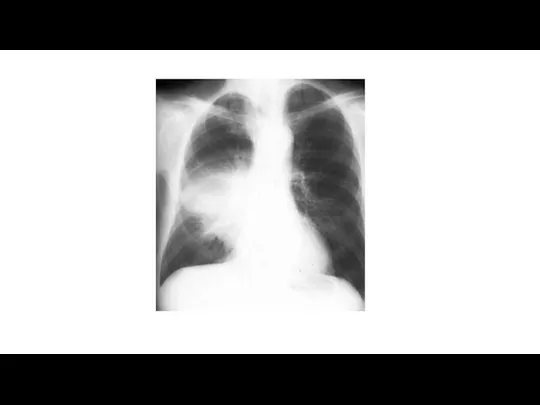
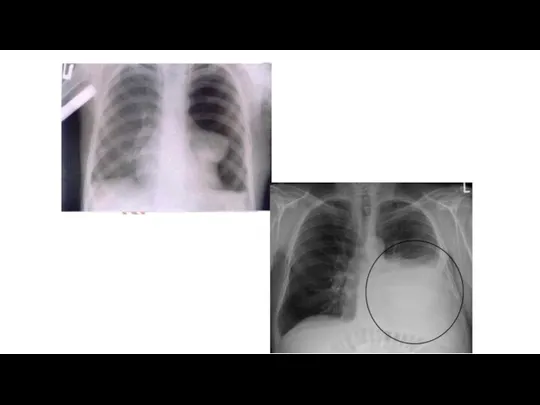
- 13. Pneumonia -acute infection of respiratory part
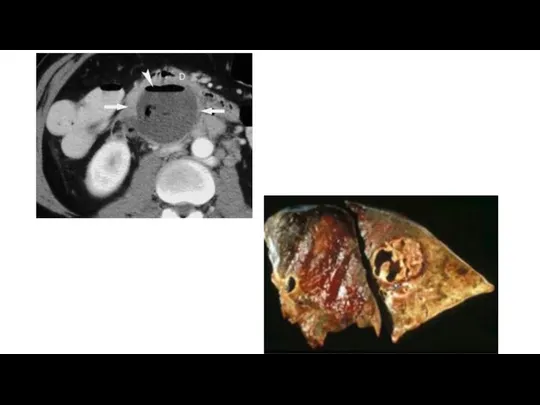
- 15. Абсцесс легкого Abscess
- 18. Atelectasis - loss of airiness of the lung tissue Fluid Compression atelectasis Air
- 20. Obstructive atelectasis
- 21. Percussion of the lung
- 22. Comparative Percussion: Dullness or shortening of the percussion sound occurs when the lung tissue is compacted
- 23. Symbols Voice vibration Percussion tone
- 24. Lung auscultation АУСКУЛЬТАЦИЯ ЛЕГКИХ
- 25. History /История аускультации Hippocrates / Гиппократ – непосредственная аускультация ухом René-Théophile-Hyacinthe Laennec[ (1781 –1826) was a
- 28. Conditions for auscultation/ Условия проведения аускультации The patient in a sitting or standing position, breathing through
- 29. Purposes / Цели аускультации Recognize the basic breath sound / оценить основной дыхательный шум 2. Recognize
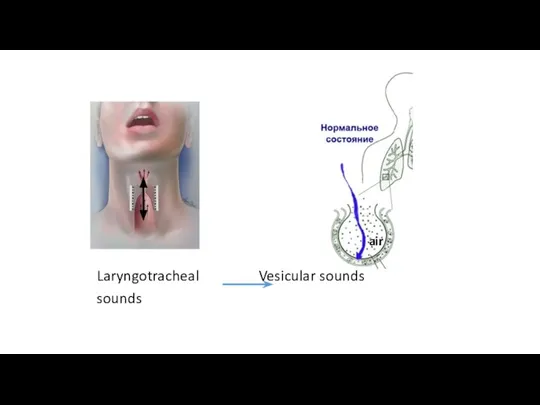
- 30. Basic breath sounds For lungs normal sound – vesicular sounds Origin: 1 step: sound is generated
- 31. Laryngotracheal Vesicular sounds sounds air
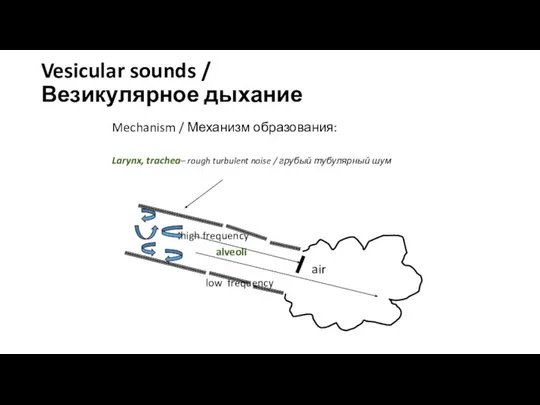
- 32. Vesicular sounds / Везикулярное дыхание Mechanism / Механизм образования: Larynx, trachea– rough turbulent noise / грубый
- 33. Vesicular sounds - normal for the lungs auscultation Laryngotracheal sounds – normal for the …. But
- 34. Auscultation depends on: 1. Upper respiratory tracts condition 2. Bronchial condition (patency) 3. Status alveoli 4.
- 35. Evaluation of the vesicular sound Vesicular breath sounds are soft and low pitched with a rustling
- 36. Evaluation of the vesicular sounds Attenuation / Ослабление А. Diffuse / Диффузное Reasons: - hyperinflation /
- 37. Laryngotracheal sounds ! Pathological laryngotracheal sound always local Reason – consolidation of lung tissue due to
- 38. Adventitious (additional) breathing sounds / Дополнительные дыхательные шумы Crackles - Fine crackles are brief, discontinuous, popping
- 39. Adventitious breath sounds - Coarse crackles are discontinuous, brief, popping lung sounds. Compared to fine crackles
- 40. Adventitious breath sounds Wheezes are lung sounds that are continuous with a musical quality. Wheezes can
- 41. Adventitious breath sounds Monophonic wheezes (rhonchi) are loud, continuous sounds occurring in inspiration, expiration or throughout
- 42. Adventitious breathing sounds Polyphonic wheezes are loud, musical and continuous. These breath sounds occur in expiration
- 43. Pleural rubs are discontinuous or continuous, creaking sounds. The sound has been described as similar to
- 44. Bronchophony Ask the patient to say "99" several times while auscultating the chest walls. Over healthy
- 46. Скачать презентацию
Physical examination
General inspection
Cyanosis (diffuse, warm) – respiratory failure
Hyperemia of
Physical examination
General inspection
Cyanosis (diffuse, warm) – respiratory failure
Hyperemia of
2. Examination of the chest
1)The shape of the chest normal
2. Examination of the chest
1)The shape of the chest normal
4) The position of the clavicles, supra- and subclavian fossae, the
4) The position of the clavicles, supra- and subclavian fossae, the
3. Palpation of the chest
Objectives
Assess pain
Determine the resistance
3. Palpation of the chest
Objectives
Assess pain
Determine the resistance
Voice vibration
palpation sensation of chest vibration when pronouncing individual words containing
Voice vibration
palpation sensation of chest vibration when pronouncing individual words containing
Basic pathology of the lung
Basic pathology of the lung
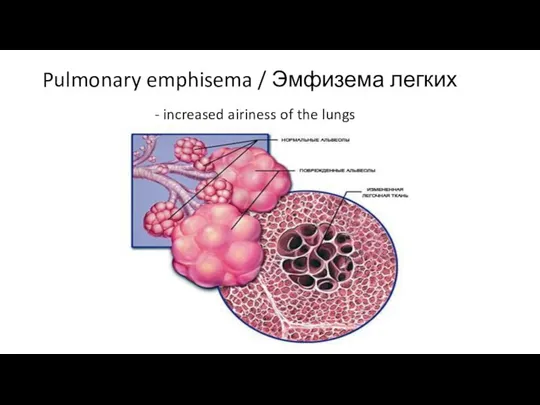
Pulmonary emphisema / Эмфизема легких
- increased airiness of the lungs
Pulmonary emphisema / Эмфизема легких
- increased airiness of the lungs
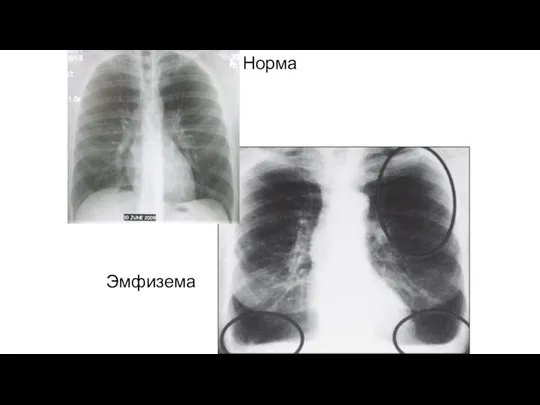
Норма
Эмфизема
Норма
Эмфизема
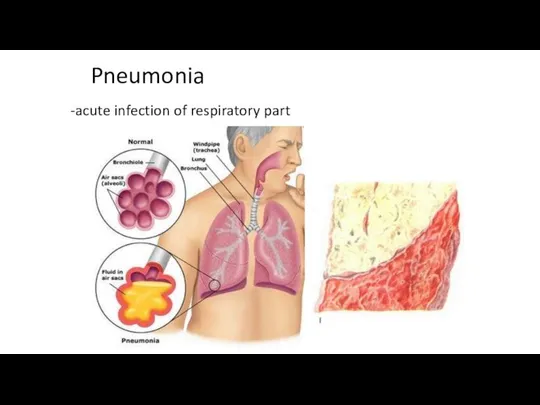
Pneumonia
-acute infection of respiratory part
Pneumonia
-acute infection of respiratory part
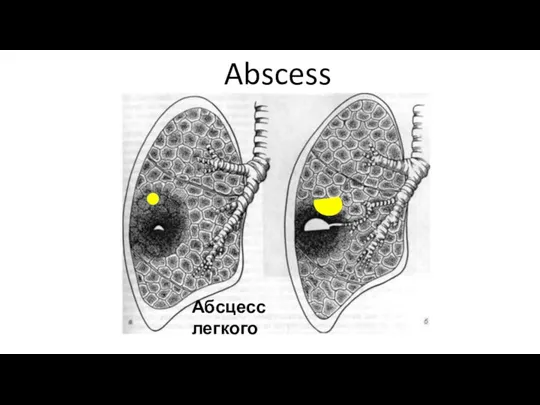
Абсцесс легкого
Abscess
Абсцесс легкого
Abscess

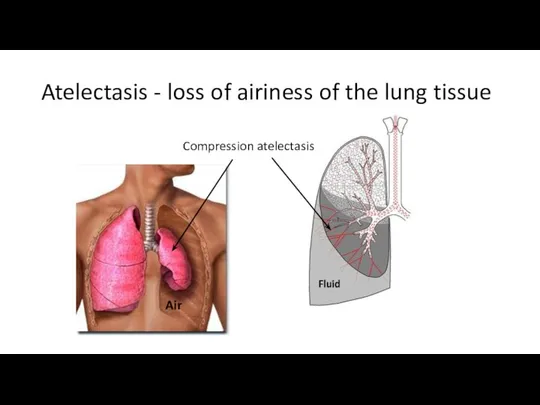
Atelectasis - loss of airiness of the lung tissue
Fluid
Compression atelectasis
Air
Atelectasis - loss of airiness of the lung tissue
Fluid
Compression atelectasis
Air
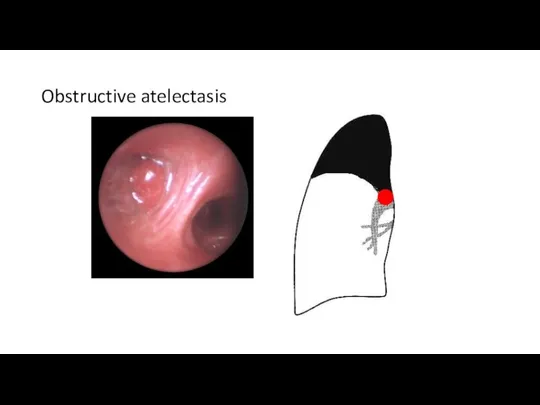
Obstructive atelectasis
Obstructive atelectasis
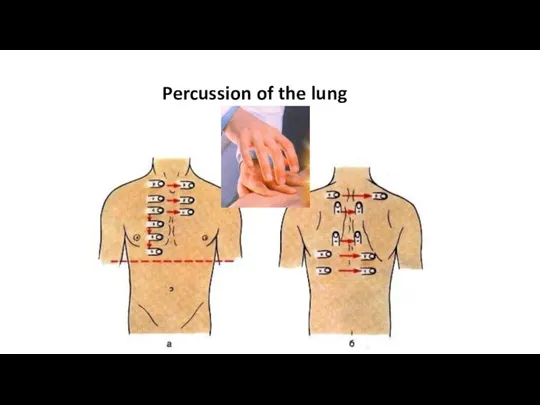
Percussion of the lung
Percussion of the lung
Comparative Percussion:
Dullness or shortening of the percussion sound occurs when
Comparative Percussion:
Dullness or shortening of the percussion sound occurs when
Symbols
Voice vibration
Percussion tone
Symbols
Voice vibration
Percussion tone
Lung auscultation
АУСКУЛЬТАЦИЯ ЛЕГКИХ
Lung auscultation
АУСКУЛЬТАЦИЯ ЛЕГКИХ
History /История аускультации
Hippocrates / Гиппократ – непосредственная аускультация ухом
René-Théophile-Hyacinthe Laennec[ (1781 –1826)
History /История аускультации
Hippocrates / Гиппократ – непосредственная аускультация ухом
René-Théophile-Hyacinthe Laennec[ (1781 –1826)
Conditions for auscultation/
Условия проведения аускультации
The patient in a sitting
Conditions for auscultation/
Условия проведения аускультации
The patient in a sitting
Purposes / Цели аускультации
Recognize the basic breath sound /
Purposes / Цели аускультации
Recognize the basic breath sound /
Basic breath sounds
For lungs normal sound – vesicular sounds
Origin: 1 step:
Basic breath sounds
For lungs normal sound – vesicular sounds
Origin: 1 step:
Laryngotracheal Vesicular sounds
sounds
air
Laryngotracheal Vesicular sounds
sounds
air
Vesicular sounds /
Везикулярное дыхание
Mechanism / Механизм образования:
Larynx, trachea– rough turbulent noise
Vesicular sounds /
Везикулярное дыхание
Mechanism / Механизм образования:
Larynx, trachea– rough turbulent noise
Vesicular sounds - normal for the lungs auscultation
Laryngotracheal sounds –
Vesicular sounds - normal for the lungs auscultation
Laryngotracheal sounds –
Auscultation depends on:
1. Upper respiratory tracts condition
2. Bronchial condition
Auscultation depends on:
1. Upper respiratory tracts condition
2. Bronchial condition
Evaluation of the vesicular sound
Vesicular breath sounds are soft and
Evaluation of the vesicular sound
Vesicular breath sounds are soft and
Evaluation of the vesicular sounds
Attenuation / Ослабление
А. Diffuse / Диффузное
Reasons:
Evaluation of the vesicular sounds
Attenuation / Ослабление
А. Diffuse / Диффузное
Reasons:
Laryngotracheal sounds
! Pathological laryngotracheal sound always local
Reason – consolidation
Laryngotracheal sounds
! Pathological laryngotracheal sound always local
Reason – consolidation
Adventitious (additional) breathing sounds /
Дополнительные дыхательные шумы
Crackles
- Fine crackles
Adventitious (additional) breathing sounds /
Дополнительные дыхательные шумы
Crackles
- Fine crackles
Adventitious breath sounds
- Coarse crackles
are discontinuous, brief, popping lung
Adventitious breath sounds
- Coarse crackles
are discontinuous, brief, popping lung
Adventitious breath sounds
Wheezes
are lung sounds that are continuous with a
Adventitious breath sounds
Wheezes
are lung sounds that are continuous with a
Adventitious breath sounds
Monophonic wheezes (rhonchi) are loud, continuous sounds occurring in
Adventitious breath sounds
Monophonic wheezes (rhonchi) are loud, continuous sounds occurring in
Adventitious breathing sounds
Polyphonic wheezes are loud, musical and continuous. These breath
Adventitious breathing sounds
Polyphonic wheezes are loud, musical and continuous. These breath
Pleural rubs
are discontinuous or continuous, creaking sounds.
The sound has
Pleural rubs
are discontinuous or continuous, creaking sounds.
The sound has
Bronchophony
Ask the patient to say "99" several times while auscultating the
Bronchophony
Ask the patient to say "99" several times while auscultating the
 ЛИШАЙНИКИ
ЛИШАЙНИКИ Тип Саркожгутиконосцы. Класс Саркодовые (Корненожки)
Тип Саркожгутиконосцы. Класс Саркодовые (Корненожки) Астық тұқымдастар - бағалы азықтық өсімдіктер
Астық тұқымдастар - бағалы азықтық өсімдіктер 6 Б класс МОУ СОШ №18 г. Иркутска Учитель Бабич Т.Р.
6 Б класс МОУ СОШ №18 г. Иркутска Учитель Бабич Т.Р. Чарльз Дарвин и его теория возникновения жизни
Чарльз Дарвин и его теория возникновения жизни Своя игра. 8 класс
Своя игра. 8 класс Презентация на тему "Строение сердца. Сердечный цикл." - скачать бесплатно презентации по Биологии
Презентация на тему "Строение сердца. Сердечный цикл." - скачать бесплатно презентации по Биологии Презентация на тему Генные технологии и биоэтика
Презентация на тему Генные технологии и биоэтика  Окружающий мир 2 класс. УМК Начальная школа XXI века. Поле и его обитатели
Окружающий мир 2 класс. УМК Начальная школа XXI века. Поле и его обитатели Кайнозойская эра текущая эра геологической истории Земли. Началась 66,0 миллионов лет и продолжается до сих пор. Название перево
Кайнозойская эра текущая эра геологической истории Земли. Началась 66,0 миллионов лет и продолжается до сих пор. Название перево Взаимодействие генов и их множественное действие
Взаимодействие генов и их множественное действие Условия содержания птиц
Условия содержания птиц Клеточное строение листа
Клеточное строение листа Тритикаленің химиялық құрамы мен құрылымы
Тритикаленің химиялық құрамы мен құрылымы Семейство ЛИЛЕЙНЫЕ Автор: Толстова Светлана Викентьевна, Учитель биологии МОУ СОШ №3 г. Канск, Красноярского края
Семейство ЛИЛЕЙНЫЕ Автор: Толстова Светлана Викентьевна, Учитель биологии МОУ СОШ №3 г. Канск, Красноярского края Жизнь на разных материках. (Часть 2)
Жизнь на разных материках. (Часть 2) Основные законы наследования признаков
Основные законы наследования признаков ВИРУСЫ Презентацию подготовил ученик 10 «В» класса Зверев Вениамин
ВИРУСЫ Презентацию подготовил ученик 10 «В» класса Зверев Вениамин Отруєння наркотичними речовинами
Отруєння наркотичними речовинами  Цитоплазма Митохондрии, пластиды, органоиды движения, включения.
Цитоплазма Митохондрии, пластиды, органоиды движения, включения. Этапы развития взаимодействия человека и природы
Этапы развития взаимодействия человека и природы Каракал
Каракал Картон в борьбе с сорняками
Картон в борьбе с сорняками ЗАДАЧИ И МЕТОДЫ ГЕНЕТИКИ.ПЕРВЫЙ И ВТОРОЙ ЗАКОНЫ Г.МЕНДЕЛЯ. Цель урока : сформировать знания о генетике как о науке о законо
ЗАДАЧИ И МЕТОДЫ ГЕНЕТИКИ.ПЕРВЫЙ И ВТОРОЙ ЗАКОНЫ Г.МЕНДЕЛЯ. Цель урока : сформировать знания о генетике как о науке о законо What is Speciation ?
What is Speciation ? Презентация на тему "Динамика популяций." - скачать бесплатно презентации по Биологии
Презентация на тему "Динамика популяций." - скачать бесплатно презентации по Биологии Презентация на тему "Грибы" - скачать бесплатно презентации по Биологии
Презентация на тему "Грибы" - скачать бесплатно презентации по Биологии Русский охотничий спаниель
Русский охотничий спаниель