- Anatomy of bones in childhood

Содержание
- 2. The Anatomical and physiological particularities of bone and muscular systems & its clinical importance. The Teeth
- 3. The First kernel of the large bone ossification appears in a 7-8 weeks aged embryo within
- 4. After birth the size of skeleton increases very intensively according the mass and length growth of
- 5. The fetus and newborn have a sponge like bone masses (A). After age of 3-4 years
- 6. The regeneration and healing processes in child bones occur in contrast with adult much sooner. Because
- 7. Periosteal tissues (a bone cover) provide supplemental trofic function. By comparison with adult persons in children
- 8. Toddler's fracture. Anterior-posterior radiograph of tibia. Spiral fracture is presented.
- 9. 3 parameters associated with bone tissue development and biochemicaly same teeth matrix should participate in biological
- 10. The Short Notion about kernels of the ossification. In wrist commonly used for bone age determination
- 11. Wrist X-Ray in a 1 yr old infant 2 visible bones n=1+m, где n – number
- 12. The bone, growth, teeth and passport age coincidence is indicative for the normal biological development in
- 13. The skeleton examination and the most important semiotics of bone diseases in children.
- 14. Estimating the bone system the next clinical approaches are useful: Complaints Additional questioning (case history) Objective
- 15. The most common complaint is the pain. Most often the extremities pain in children depends on
- 16. Complaints "Pains of the growing" are typical bed time accidental and self limited symptoms in a
- 17. Complaints The Flat foot Pains disturb some children commonly in shank and appear more often at
- 18. Complaints The most serious pain symptom which could be claimed by the child is a night
- 19. The big diagnostic importance has combination of pain and fixed position of limb. Septic arthritis and
- 20. The big diagnostic importance has combination of pain and fixed position of limb. Characteristic posture of
- 21. Visual inspection & palpation The Objective investigation of the skeleton is recommended to conduct from the
- 22. The skull
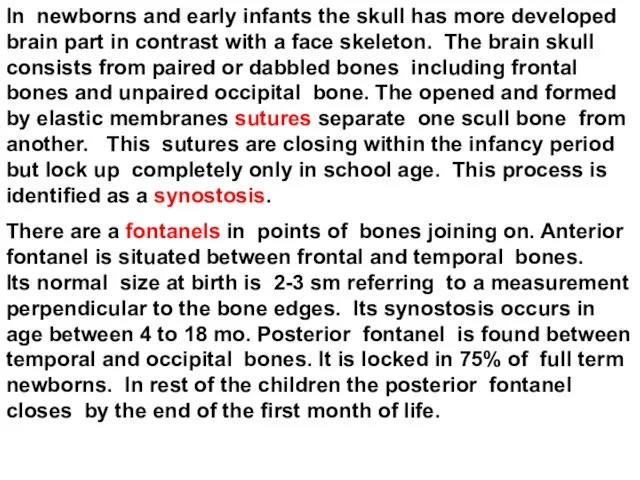
- 23. In newborns and early infants the skull has more developed brain part in contrast with a
- 24. During the difficult labor the skull bone edges are crawling one another one. This is a
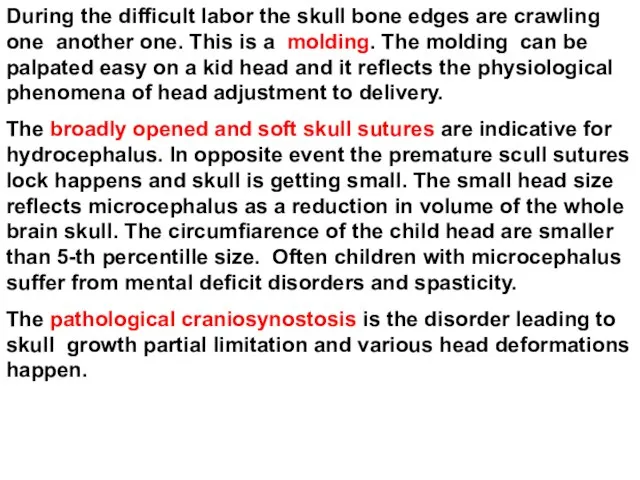
- 25. The pathological craniosynostosis This newborn girl with venus suture craniosynostosis has cloverleaf skull. In this cases
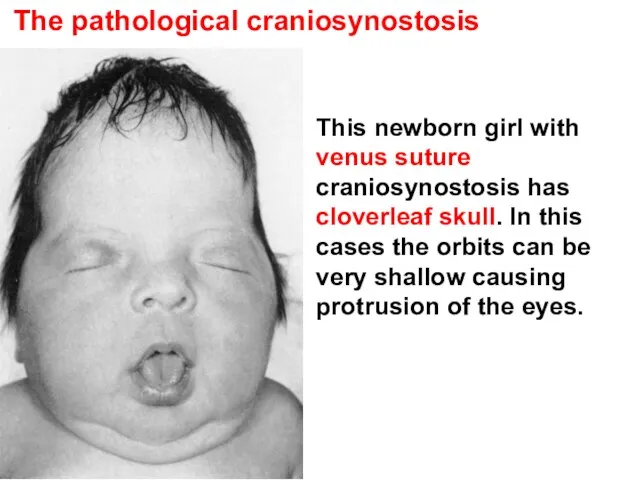
- 26. Three-week-old infant with premature sagittal craniosynostosis. Lateral view demonstrates the elongated head shape with tapering in
- 27. The kraniotabes is unusual softness of infantile skull. It can develop as a sign of vitamin-D-deficient
- 28. The Cephalhematoma is a wide-spreaded delivery trauma of bones forming skull arc in newborns. The Cephalhematoma
- 29. The Neck.
- 30. Congenital torticollis Left photo is an example of "position of discomfort" of a large baby who
- 31. The chest
- 32. In small children the thorax has rounded form and starts to be flat in anterior-posterior axis
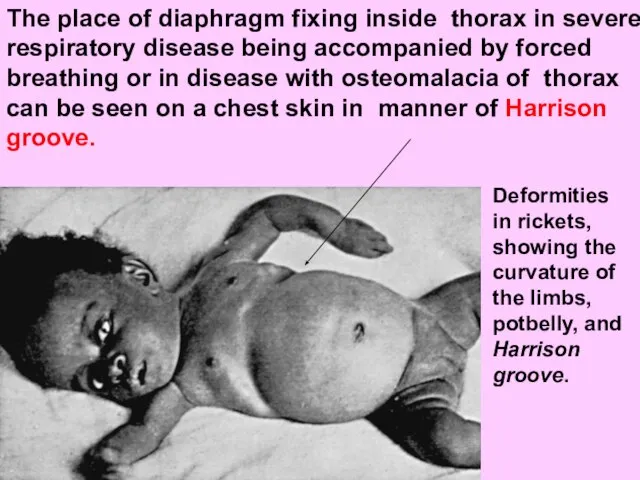
- 33. The place of diaphragm fixing inside thorax in severe respiratory disease being accompanied by forced breathing
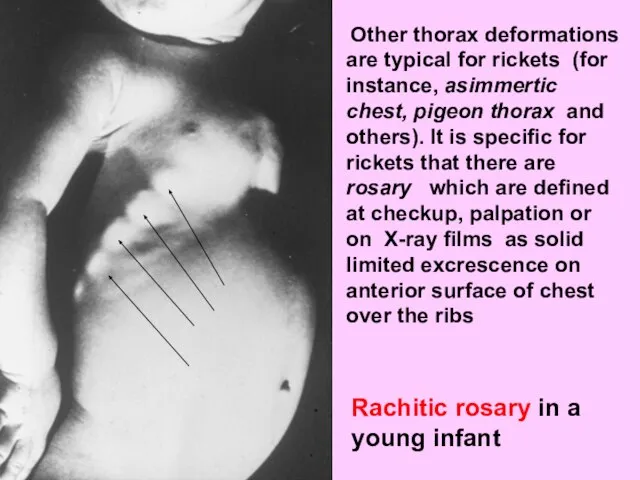
- 34. Other thorax deformations are typical for rickets (for instance, asimmertic chest, pigeon thorax and others). It
- 35. Other thorax deformations The insulated thorax deformations most often are innate and same of them can
- 36. The spine.
- 37. Spinal curves In newborns the spine is direct with a small protuberance backwards in the area
- 38. The spine deviations aside are never being physiological and are nominated as scoliotic. One of the
- 39. Structural changes in idiopathic scoliosis. As curvature increases, alterations in body configuration develop in both the
- 40. The limbs and tubular bones.
- 41. In young children the tubular bones are filled with the actively-functioning red marrow. The long tubular
- 42. Limb` deformations It is known that multiple symmetric deformations of upper and lower limbs are characteristic
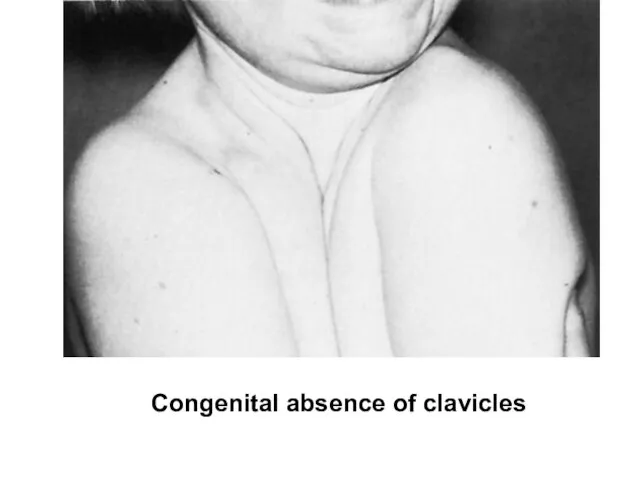
- 43. Skeleton` deformations If the deformations of skeleton are conditioned by anatomical elements lost (for instance, absence
- 44. Congenital absence of clavicles
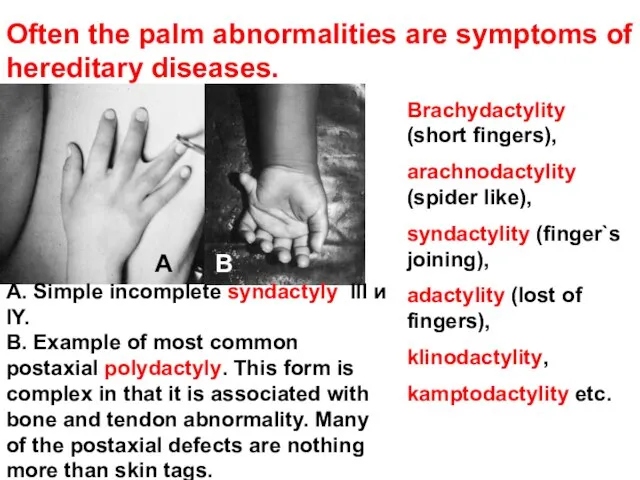
- 45. Often the palm abnormalities are symptoms of hereditary diseases. Brachydactylity (short fingers), arachnodactylity (spider like), syndactylity
- 46. The symptoms of innate displastic/dislocative hip (DDH) in infants and children.
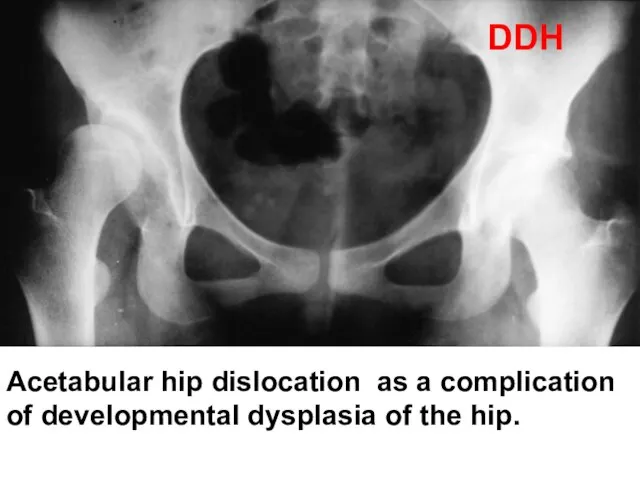
- 47. Acetabular hip dislocation as a complication of developmental dysplasia of the hip. DDH
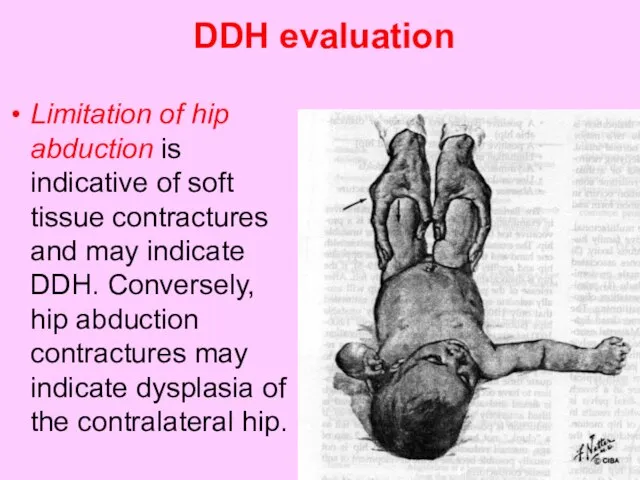
- 48. DDH evaluation Limitation of hip abduction is indicative of soft tissue contractures and may indicate DDH.
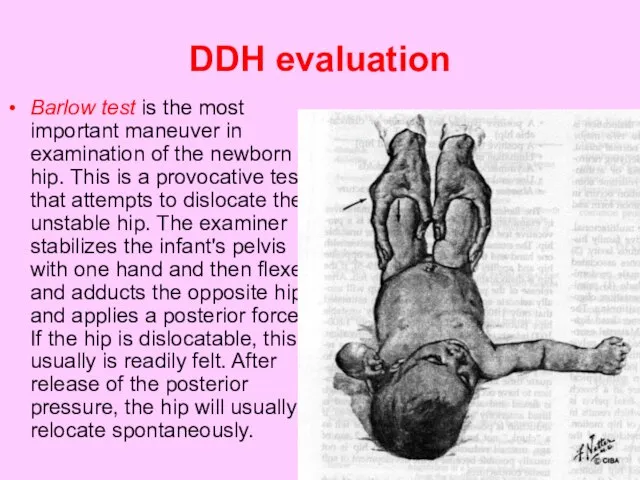
- 49. DDH evaluation Barlow test is the most important maneuver in examination of the newborn hip. This
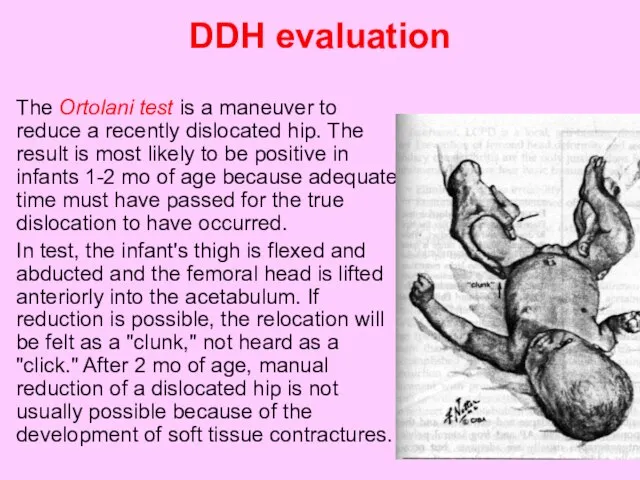
- 50. DDH evaluation The Ortolani test is a maneuver to reduce a recently dislocated hip. The result
- 51. DDH evaluation An asymmetric number of thigh skinfolds and apparent shortening of an extremity when the
- 52. DDH evaluation In older or walking children, complaints of limping, waddling (bilateral DDH), increased lumbar lordosis
- 53. The teeth and teeth formula in children. The semiotics of teeth diseases.
- 54. The teeth are a skin appurtenance because they are derived from the embrio ectoderma. But on
- 55. The appearing of baby teeth (or primary deciduous teeth) is called as a dentition. The dentition
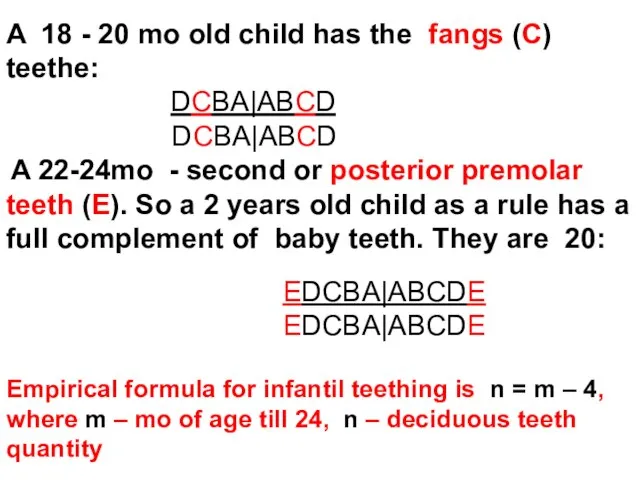
- 56. A 12 -15 mo old child as a rule has the first or anterior premolar teeth(
- 57. A 18 - 20 mo old child has the fangs (C) teethe: DCBA|ABCD DCBA|ABCD A 22-24mo
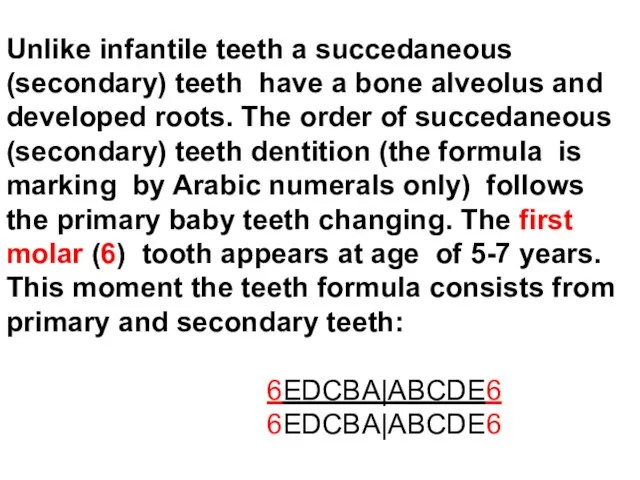
- 58. Unlike infantile teeth a succedaneous (secondary) teeth have a bone alveolus and developed roots. The order
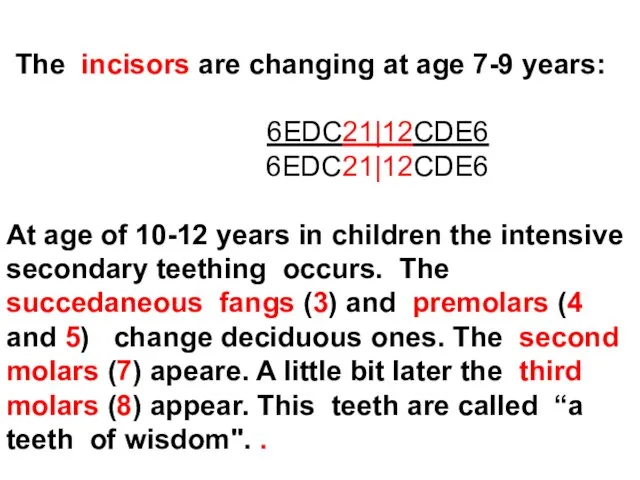
- 59. The incisors are changing at age 7-9 years: 6EDC21|12CDE6 6EDC21|12CDE6 At age of 10-12 years in
- 60. What is the “difficult" teething? Pain, itching, hypersalivation. Head cold. Fever. Diarrhea. Always a physician has
- 61. The caries and toothache in children. The caries is a destruction of hard tissues of tooth.
- 62. In small children having deciduous teeth with small amount of dentin the dental caries has some
- 63. The Particularities of dental traumas in children Intruded primary incisor that appears knocked out. Radiograph documents
- 64. Hutchinson`s teeth in congenital syphilis
- 65. The features of muscles in children
- 66. Some features of muscles The hystomorfological studies of muscular tissues in young children show the short
- 67. The skeleton muscles clinical investigation The complaints most often concern such subjective sensations of pain in
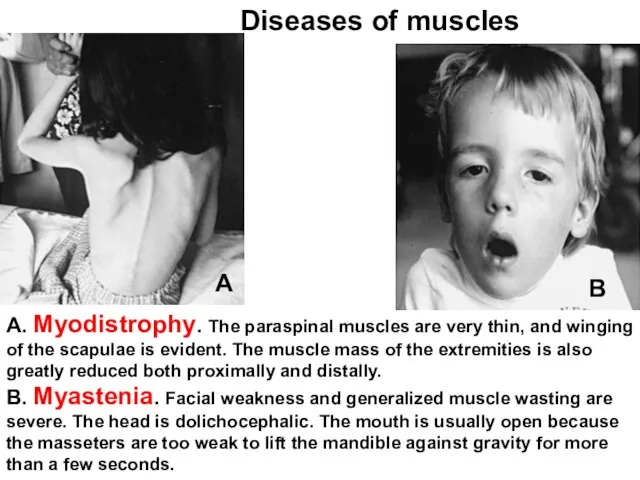
- 68. А. Myodistrophy. The paraspinal muscles are very thin, and winging of the scapulae is evident. The
- 69. Right-sided diaphragmatic (obstetrics) paralysis secondary to phrenic nerve injury, with elevation of the right hemidiaphragm and
- 71. Скачать презентацию
The Anatomical and physiological particularities of bone and muscular systems &
The Anatomical and physiological particularities of bone and muscular systems &
The First kernel of the large bone ossification appears in
The First kernel of the large bone ossification appears in
After birth the size of skeleton increases very intensively according the
After birth the size of skeleton increases very intensively according the
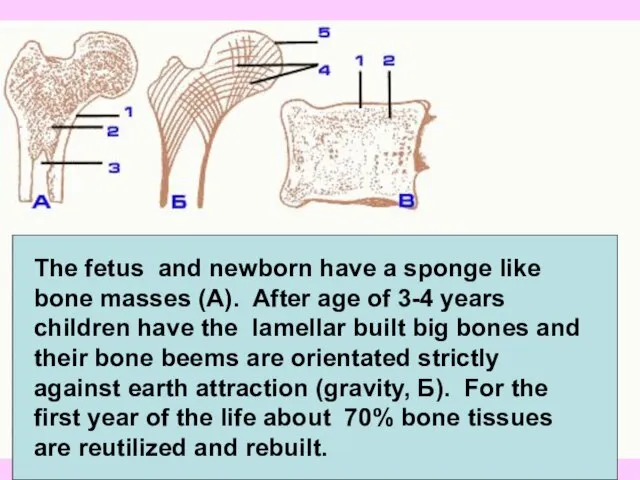
The fetus and newborn have a sponge like bone masses (A).
The fetus and newborn have a sponge like bone masses (A).
The regeneration and healing processes in child bones occur in
The regeneration and healing processes in child bones occur in
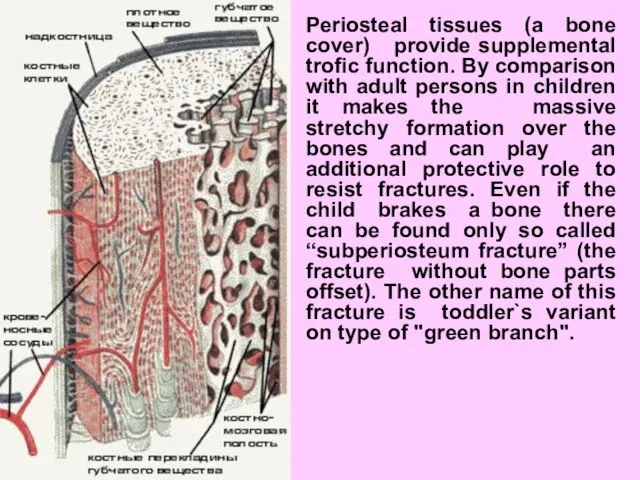
Periosteal tissues (a bone cover) provide supplemental trofic function. By comparison
Periosteal tissues (a bone cover) provide supplemental trofic function. By comparison
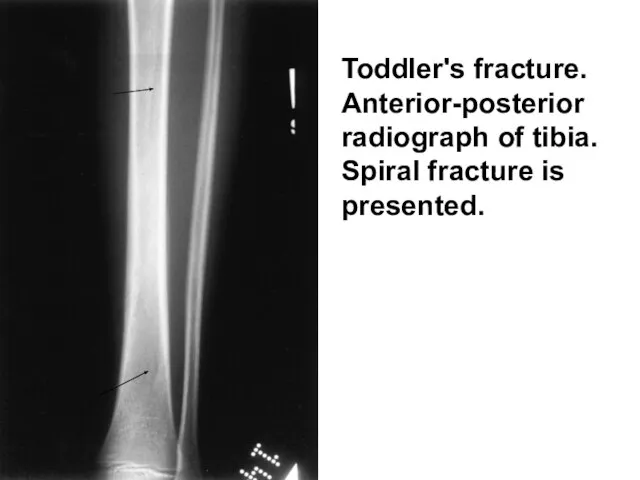
Toddler's fracture. Anterior-posterior radiograph of tibia. Spiral fracture is presented.
Toddler's fracture. Anterior-posterior radiograph of tibia. Spiral fracture is presented.
3 parameters associated with bone tissue development and biochemicaly same
3 parameters associated with bone tissue development and biochemicaly same
The Short Notion about kernels of the ossification.
In wrist commonly used
The Short Notion about kernels of the ossification.
In wrist commonly used

Wrist X-Ray in a 1 yr old infant
2 visible bones
n=1+m,
Wrist X-Ray in a 1 yr old infant
2 visible bones
n=1+m,
The bone, growth, teeth and passport age coincidence is indicative
The bone, growth, teeth and passport age coincidence is indicative
The skeleton examination and the most important semiotics of bone diseases
The skeleton examination and the most important semiotics of bone diseases
Estimating the bone system the next clinical approaches are useful:
Complaints
Additional questioning
Estimating the bone system the next clinical approaches are useful:
Complaints
Additional questioning
The most common complaint is the pain. Most often the
The most common complaint is the pain. Most often the
Complaints
"Pains of the growing" are typical bed time accidental and self
Complaints
"Pains of the growing" are typical bed time accidental and self
Complaints
The Flat foot Pains disturb some children commonly in shank and
Complaints
The Flat foot Pains disturb some children commonly in shank and
Complaints
The most serious pain symptom which could be claimed by the
Complaints
The most serious pain symptom which could be claimed by the
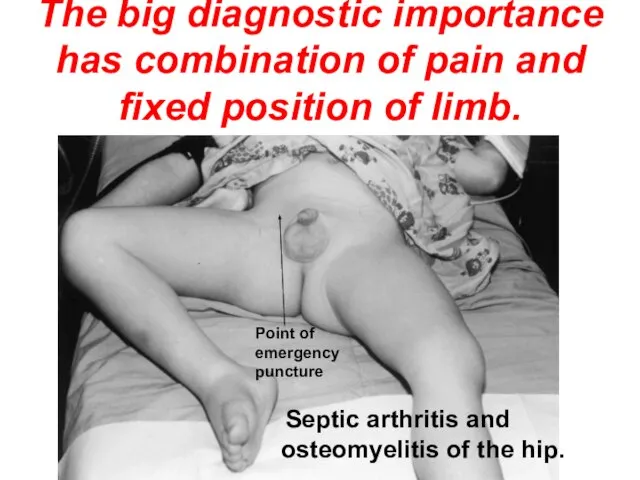
The big diagnostic importance has combination of pain and fixed position
The big diagnostic importance has combination of pain and fixed position
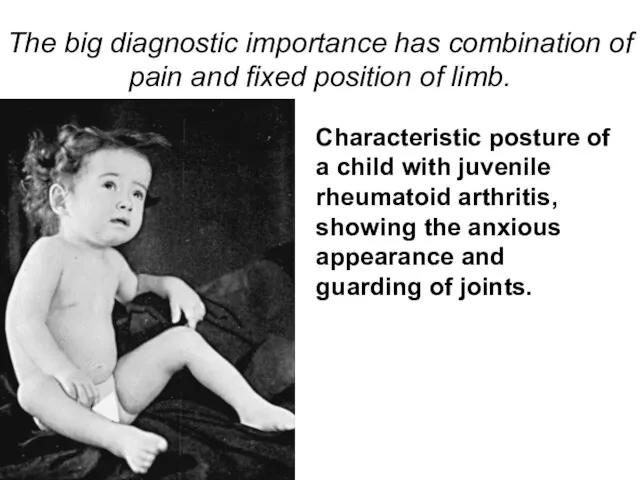
The big diagnostic importance has combination of pain and fixed position
The big diagnostic importance has combination of pain and fixed position
Visual inspection & palpation
The Objective investigation of the skeleton is
Visual inspection & palpation
The Objective investigation of the skeleton is
The skull
The skull
In newborns and early infants the skull has more developed brain
In newborns and early infants the skull has more developed brain
During the difficult labor the skull bone edges are crawling one
During the difficult labor the skull bone edges are crawling one
The pathological craniosynostosis
This newborn girl with venus suture craniosynostosis has
The pathological craniosynostosis
This newborn girl with venus suture craniosynostosis has
Three-week-old infant with premature sagittal craniosynostosis.
Lateral view demonstrates the elongated
Three-week-old infant with premature sagittal craniosynostosis.
Lateral view demonstrates the elongated
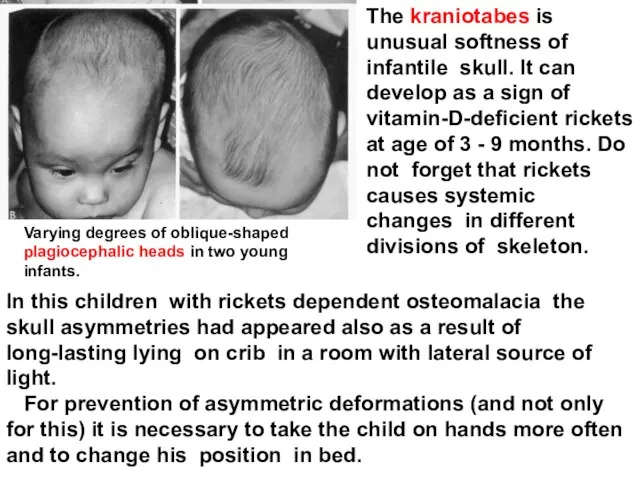
The kraniotabes is unusual softness of infantile skull. It can develop
The kraniotabes is unusual softness of infantile skull. It can develop
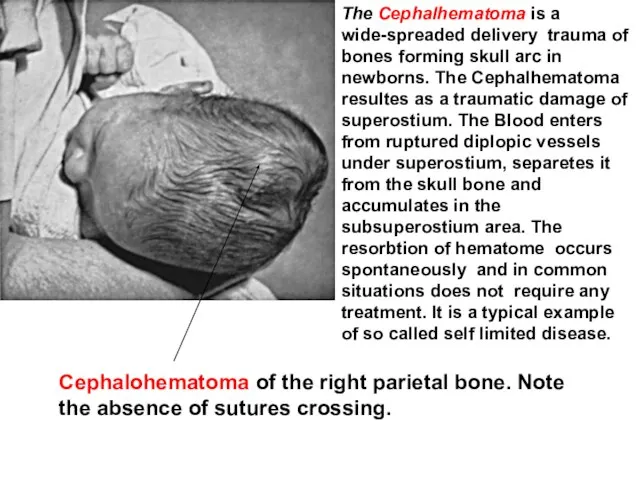
The Cephalhematoma is a wide-spreaded delivery trauma of bones forming skull
The Cephalhematoma is a wide-spreaded delivery trauma of bones forming skull
The Neck.
The Neck.
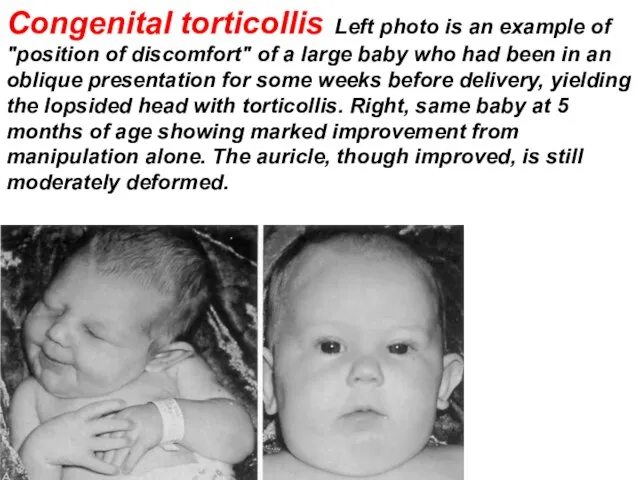
Congenital torticollis Left photo is an example of "position of discomfort"
Congenital torticollis Left photo is an example of "position of discomfort"
The chest
The chest
In small children the thorax has rounded form and starts to
In small children the thorax has rounded form and starts to
The place of diaphragm fixing inside thorax in severe respiratory disease
The place of diaphragm fixing inside thorax in severe respiratory disease
Other thorax deformations are typical for rickets (for instance, asimmertic
Other thorax deformations are typical for rickets (for instance, asimmertic
Other thorax deformations
The insulated thorax deformations most often are
Other thorax deformations
The insulated thorax deformations most often are
The spine.
The spine.
Spinal curves
In newborns the spine is direct with a small protuberance
Spinal curves
In newborns the spine is direct with a small protuberance
The spine deviations aside are never being physiological and are
The spine deviations aside are never being physiological and are
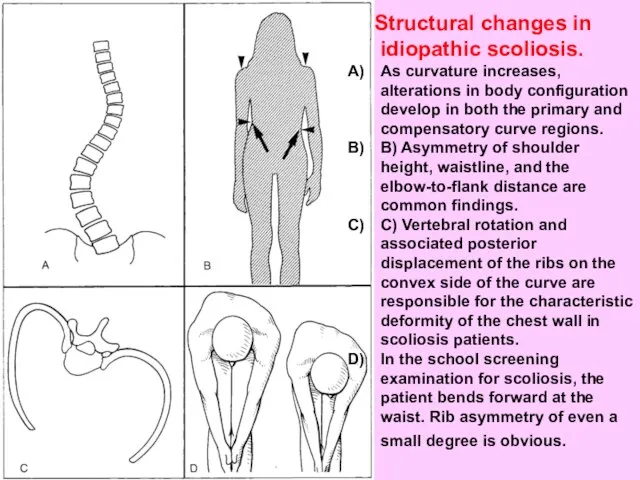
Structural changes in idiopathic scoliosis.
As curvature increases, alterations in body
As curvature increases, alterations in body
The limbs and tubular bones.

In young children the tubular bones are filled with the
In young children the tubular bones are filled with the
Limb` deformations
It is known that multiple symmetric deformations of upper and
Limb` deformations
It is known that multiple symmetric deformations of upper and
Skeleton` deformations
If the deformations of skeleton are conditioned by anatomical elements
Skeleton` deformations
If the deformations of skeleton are conditioned by anatomical elements
Congenital absence of clavicles
Congenital absence of clavicles
Often the palm abnormalities are symptoms of hereditary diseases.
Brachydactylity (short
Often the palm abnormalities are symptoms of hereditary diseases.
Brachydactylity (short

The symptoms of innate displastic/dislocative hip (DDH) in infants and
The symptoms of innate displastic/dislocative hip (DDH) in infants and
Acetabular hip dislocation as a complication of developmental dysplasia of the
Acetabular hip dislocation as a complication of developmental dysplasia of the
DDH evaluation
Limitation of hip abduction is indicative of soft
DDH evaluation
Limitation of hip abduction is indicative of soft
DDH evaluation
Barlow test is the most important maneuver in examination of
DDH evaluation
Barlow test is the most important maneuver in examination of
DDH evaluation
The Ortolani test is a maneuver to reduce a
DDH evaluation
The Ortolani test is a maneuver to reduce a
DDH evaluation
An asymmetric number of thigh skinfolds and apparent shortening
DDH evaluation
An asymmetric number of thigh skinfolds and apparent shortening
DDH evaluation
In older or walking children, complaints of limping, waddling
DDH evaluation
In older or walking children, complaints of limping, waddling
The teeth and teeth formula in children. The semiotics of teeth
The teeth and teeth formula in children. The semiotics of teeth
The teeth are a skin appurtenance because they are derived
The teeth are a skin appurtenance because they are derived
The appearing of baby teeth (or primary deciduous teeth) is
The appearing of baby teeth (or primary deciduous teeth) is
A 12 -15 mo old child as a rule has the
A 12 -15 mo old child as a rule has the
A 18 - 20 mo old child has the fangs (C)
A 18 - 20 mo old child has the fangs (C)
Unlike infantile teeth a succedaneous (secondary) teeth have a bone alveolus
Unlike infantile teeth a succedaneous (secondary) teeth have a bone alveolus
The incisors are changing at age 7-9 years:
6EDC21|12CDE6
6EDC21|12CDE6
At
The incisors are changing at age 7-9 years:
6EDC21|12CDE6
6EDC21|12CDE6
At
What is the “difficult" teething?
Pain, itching, hypersalivation.
Head cold.
What is the “difficult" teething?
Pain, itching, hypersalivation.
Head cold.
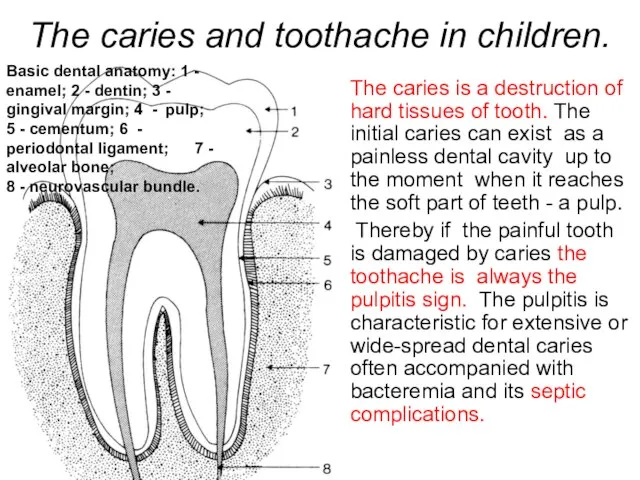
The caries and toothache in children.
The caries is a destruction of
The caries and toothache in children.
The caries is a destruction of
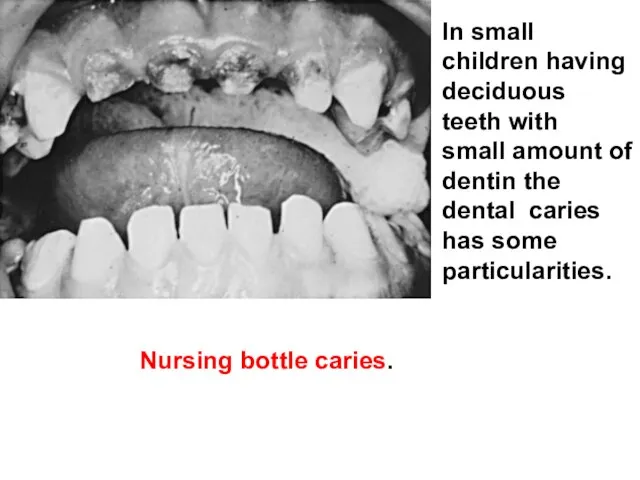
In small children having deciduous teeth with small amount of dentin
In small children having deciduous teeth with small amount of dentin
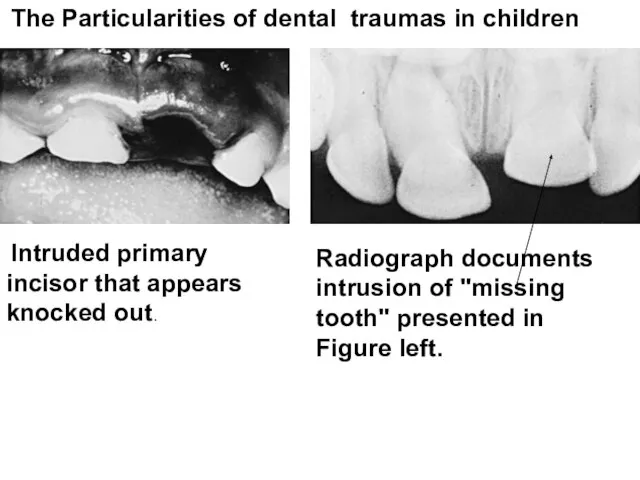
The Particularities of dental traumas in children
Intruded primary
The Particularities of dental traumas in children
Intruded primary
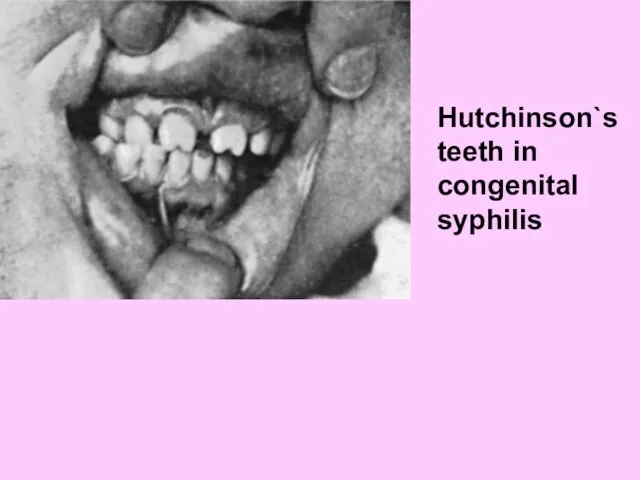
Hutchinson`s teeth in congenital syphilis
The features of muscles in children
Some features of muscles
The hystomorfological studies of muscular tissues in young
Some features of muscles
The hystomorfological studies of muscular tissues in young
The skeleton muscles clinical investigation
The complaints most often concern such subjective
The skeleton muscles clinical investigation
The complaints most often concern such subjective
А. Myodistrophy. The paraspinal muscles are very thin, and winging of
А. Myodistrophy. The paraspinal muscles are very thin, and winging of
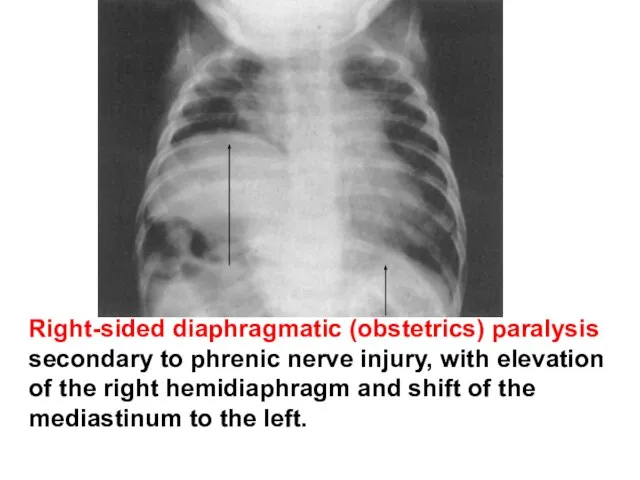
Right-sided diaphragmatic (obstetrics) paralysis secondary to phrenic nerve injury, with elevation
Right-sided diaphragmatic (obstetrics) paralysis secondary to phrenic nerve injury, with elevation
 Лабораторные методы исследования больных с заболеваниями органов мочевыделения
Лабораторные методы исследования больных с заболеваниями органов мочевыделения Система здравоохранения в Российской Федерации
Система здравоохранения в Российской Федерации Ранняя диагностика рака слизистой оболочки полости рта
Ранняя диагностика рака слизистой оболочки полости рта Перенашивание беременности
Перенашивание беременности Неонатальные желтухи
Неонатальные желтухи Острые респираторные вирусные инфекции
Острые респираторные вирусные инфекции Сердечно-легочная реанимация
Сердечно-легочная реанимация Пироплазмоз (бабезиоз) собак
Пироплазмоз (бабезиоз) собак Синтетические лекарственные препараты
Синтетические лекарственные препараты Biological rhythms and their medical values
Biological rhythms and their medical values Участие медсестры в инструментальных методах исследования
Участие медсестры в инструментальных методах исследования Болезнь Такаясу (неспецифический аортоартериит)
Болезнь Такаясу (неспецифический аортоартериит) Особенности осмотра больных при подозрении на ущемление грыжи
Особенности осмотра больных при подозрении на ущемление грыжи Десмургия. Перевязочный материал
Десмургия. Перевязочный материал Алгоритм ведения больных с инсультом на догоспитальном этапе
Алгоритм ведения больных с инсультом на догоспитальном этапе Воспаление и его причины
Воспаление и его причины Қант диабеті науқастары комплайенс
Қант диабеті науқастары комплайенс Гепатиты и циррозы печени
Гепатиты и циррозы печени Жүре пайда болған (ЖИТС, СПИД ағылш. AIDS)
Жүре пайда болған (ЖИТС, СПИД ағылш. AIDS) Современные методы лечения острой кровопотери
Современные методы лечения острой кровопотери Непрерывное медицинское образование: процедура вступления, состояние проблемы
Непрерывное медицинское образование: процедура вступления, состояние проблемы Гормональное ожирение
Гормональное ожирение Физическая работоспособность и ее связь с показателями здоровья
Физическая работоспособность и ее связь с показателями здоровья «Мы разные, мы равные, нам интересно вместе!». Образовательная система «Диалог»
«Мы разные, мы равные, нам интересно вместе!». Образовательная система «Диалог» Мұрын фурункулезі және оның асқынуы
Мұрын фурункулезі және оның асқынуы Механизм и локализации обезболивающего действия наркотических анальгетиков
Механизм и локализации обезболивающего действия наркотических анальгетиков Полипы прямой кишки у детей
Полипы прямой кишки у детей Особенности психического развития ребенка в период новорожденности
Особенности психического развития ребенка в период новорожденности