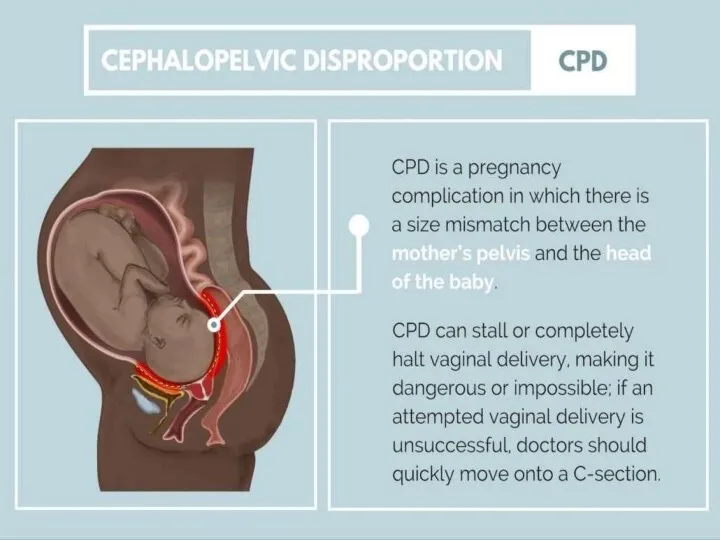
- Cephalo pelvic disproportion (Сpd)

Содержание
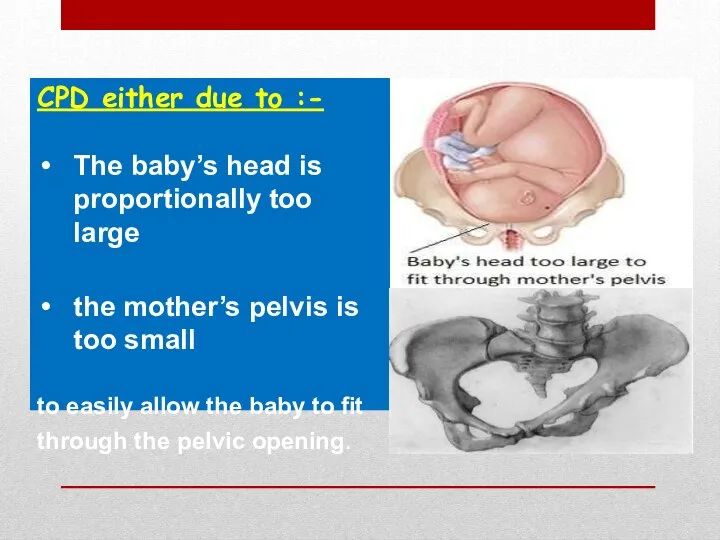
- 3. CPD either due to :- The baby’s head is proportionally too large the mother’s pelvis is
- 4. Causes :- Large baby due to: Hereditary factors Diabetes Postmaturity (still pregnant after due date has
- 5. Contracted Pelvis
- 6. Contracted Pelvis Definition: Anatomical definition: It is a pelvis in which one or more of its
- 7. Factors influencing the size and shape of the pelvis: Developmental factor: hereditary or congenital. Racial factor.
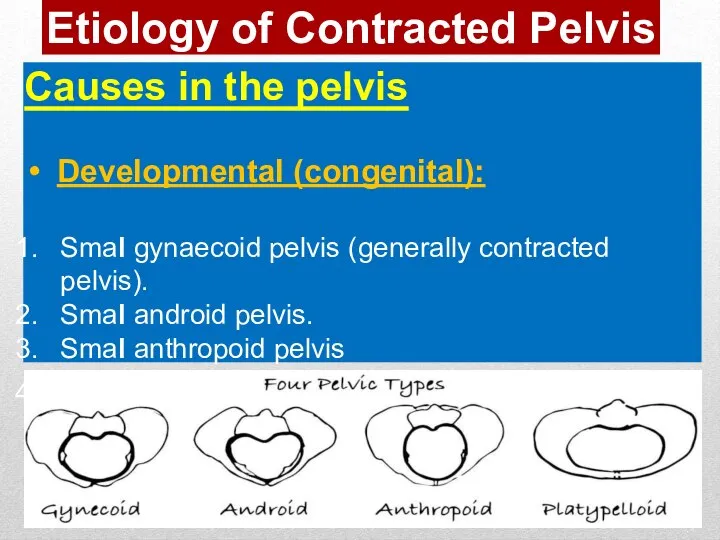
- 8. Etiology of Contracted Pelvis Causes in the pelvis Developmental (congenital): Smal gynaecoid pelvis (generally contracted pelvis).
- 9. Naegele’s pelvis: absence of one sacral ala Robert’s pelvis: absence of both sacral alae. High assimilation
- 10. Causes in the pelvis Metabolic: Rickets. Osteomalacia (triradiate pelvic brim). Traumatic: as fractures. Neoplastic: as osteoma.
- 11. Causes in the spine Lumbarkyphosis Lumbar scoliosis Spondylolisthesis: The 5th lumbar vertebra with the above vertebral
- 12. Causes in the lower limbs Dislocation of one or bothfemurs. Atrophy ofone or both lower limbs.
- 13. Pelvis History Rickets: is expected if there is a history of delayed walking and dentition. Trauma
- 14. Examination General examination: Gait: abnormal gait suggesting abnormalities in the pelvis, spines or lower limbs. Height:
- 15. Examinat ion General examination: Manifestations of rickets as: square head rosary beads in the costalridges. pigeon
- 16. Abdominal examination: Nonengagement of the head: in the last 3-4 weeks in primigravida. Pendulous abdomen: in
- 17. Pelvimetry : It is assessment of the pelvic diameters and capacity done at 38-39 weeks.It includes:
- 18. Pelvimetry: 2.Imaging pelvimetry: X-ray. Computed tomography (CT). Magnetic resonance imaging (MRI) . N.B. CTand MRI are
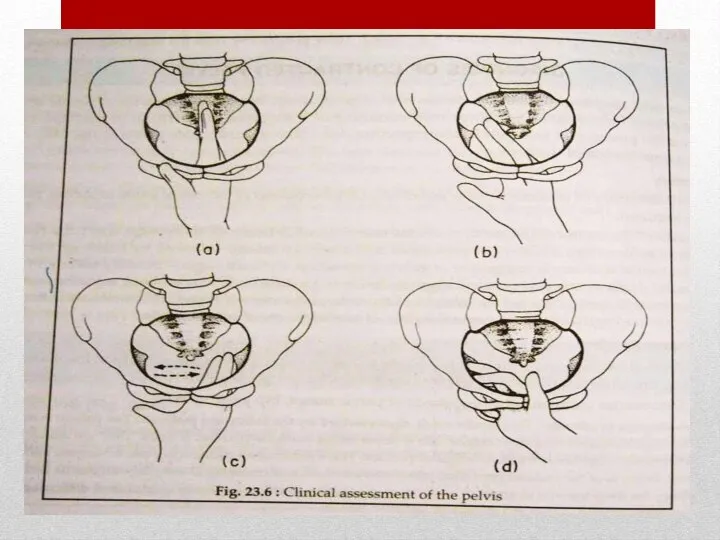
- 19. Internal pelvimetry is done through vaginalexamination 1. The inlet: Palpation of the forepelvis (pelvicbrim): The index
- 20. Internal pelvimetry 2.The cavity: Height, thickness and inclination of the symphysis. Shape and inclination of the
- 21. 2.The cavity: d.Ischial spines: Whether it is blunt (difficult to identify at all), prominent (easily felt
- 22. 2.The cavity: e.Interspinous diameter: By using the 2 examining fingers, if both spines can be touched
- 23. 3- The outlet: Subpubic angle: Normally, it admits 2fingers. Mobility of the coccyx: by pressing firmly
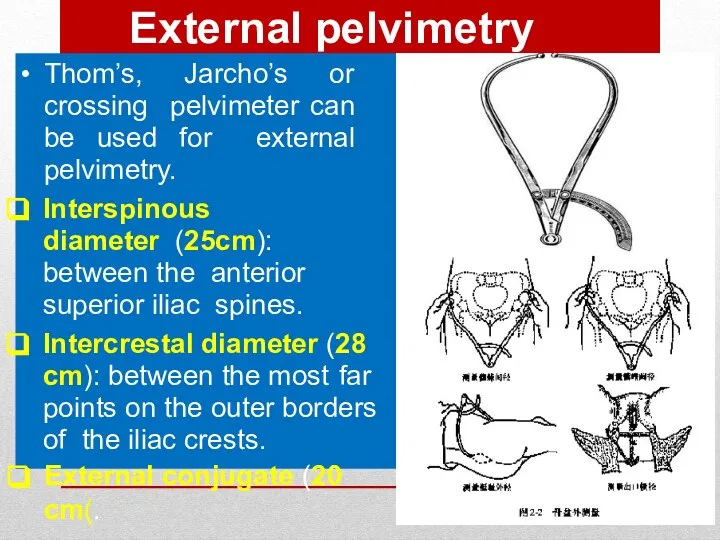
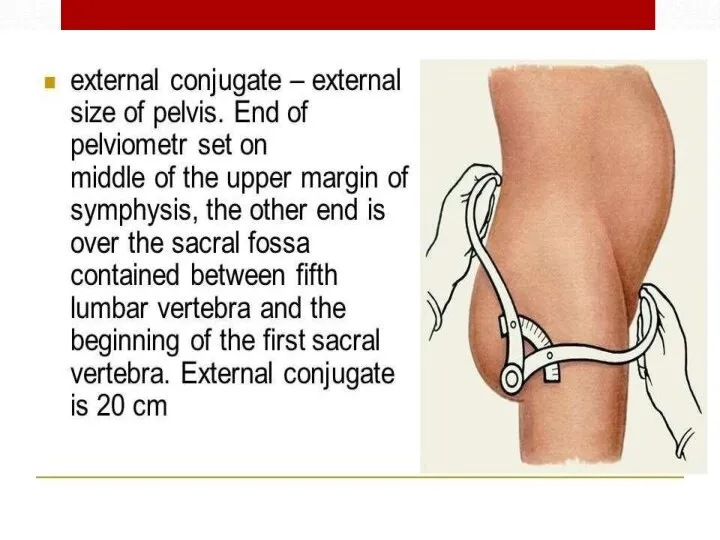
- 25. External pelvimetry Thom’s, Jarcho’s or crossing pelvimeter can be used for external pelvimetry. Interspinous diameter (25cm):
- 27. Radiological pelvimetry Lateral view: The patient stands with the X-ray tube on one side and the
- 28. Cephalometry Ultrasonography: is the safe accurate and easy method and can detect: The biparietal diameter (BPD)
- 29. Cephalopelvic disproportion tests These are done to detect contracted inlet if the head is not engaged
- 30. (2) Muller - Kerr’s method: It is more valuable in detection of the degree of disproportion.
- 31. Degrees of Disproportion Minor disproportion: The anterior surface of the head is in line with the
- 32. Degrees of Contracted Pelvis Minor degree: The true conjugate is 9-10 cm. It corresponds to minor
- 33. Management depends mainly on the degree of disproportion Minor vaginal delivery Moderate trial labor, if failed
- 34. Trial of Labour It is a clinical test for the factors that cannot be determined before
- 35. Procedure : Trial is carried out in a hospital where facilities for C.S is available. Adequate
- 36. Indications of trial of labour: Young primigravida of good health. Moderate disproportion. Vertex presentation. No contracted
- 37. Termination of trial of labour: Vaginal delivery: either spontaneously or by forceps if the head is
- 38. Indications of caesarean section in contracted pelvis Moderate disproportion if trial of labour is contraindicated or
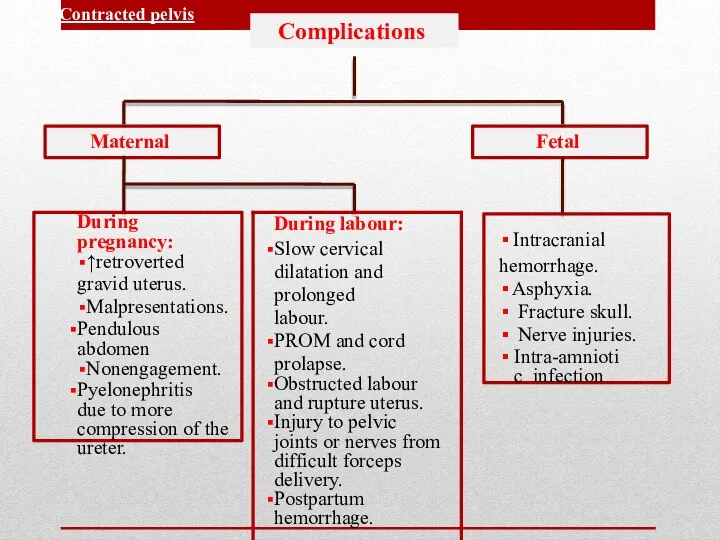
- 39. Complications Maternal Fetal Contracted pelvis
- 40. Maternal: During pregnancy: Incarcerated retroverted gravid uterus. Malpresentations. Pendulous abdomen. Nonengagement. Pyelonephritis especial y in high
- 41. Complications of Contracted Pelvis During labour: Inertia, slow cervical dilatation and prolonged labour. Premature rupture of
- 42. Foetal: Intracranial haemorrhage. Asphyxia. Fracture skull. Nerve injuries. Intra-amniotic infection. Complications of Contracted Pelvis
- 44. Скачать презентацию
CPD either due to :-
The baby’s head is proportionally too large
the
CPD either due to :-
The baby’s head is proportionally too large
the
Causes :-
Large baby due to:
Hereditary factors
Diabetes
Postmaturity (still pregnant after due date
Causes :-
Large baby due to:
Hereditary factors
Diabetes
Postmaturity (still pregnant after due date
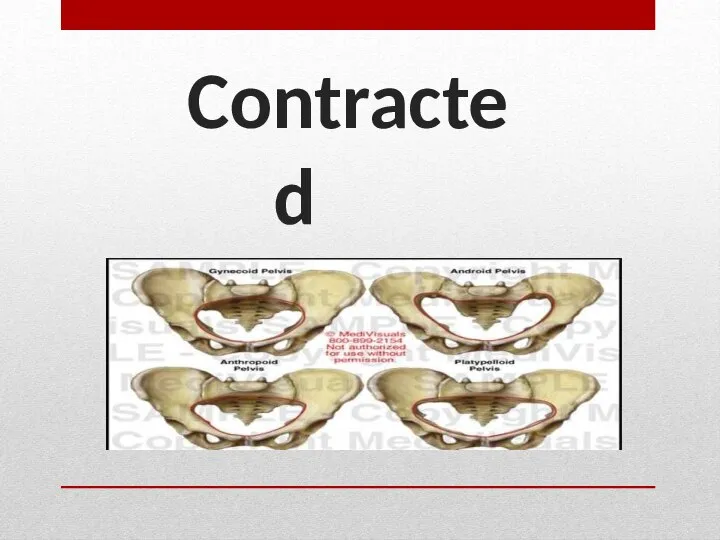
Contracted Pelvis
Contracted Pelvis
Contracted Pelvis
Definition:
Anatomical definition: It is a pelvis in which one or
Contracted Pelvis
Definition:
Anatomical definition: It is a pelvis in which one or
Factors influencing the size and shape
of the pelvis:
Developmental factor: hereditary or congenital.
Racial
Factors influencing the size and shape
of the pelvis:
Developmental factor: hereditary or congenital.
Racial
Etiology of Contracted Pelvis
Causes in the pelvis
Developmental (congenital):
Smal gynaecoid pelvis (generally
Etiology of Contracted Pelvis
Causes in the pelvis
Developmental (congenital):
Smal gynaecoid pelvis (generally
Naegele’s pelvis: absence of one sacral ala
Robert’s pelvis: absence of both
Naegele’s pelvis: absence of one sacral ala
Robert’s pelvis: absence of both
Causes in the pelvis
Metabolic:
Rickets.
Osteomalacia (triradiate pelvic brim).
Traumatic: as fractures.
Neoplastic: as osteoma.
Infection
Causes in the pelvis
Metabolic:
Rickets.
Osteomalacia (triradiate pelvic brim).
Traumatic: as fractures.
Neoplastic: as osteoma.
Infection
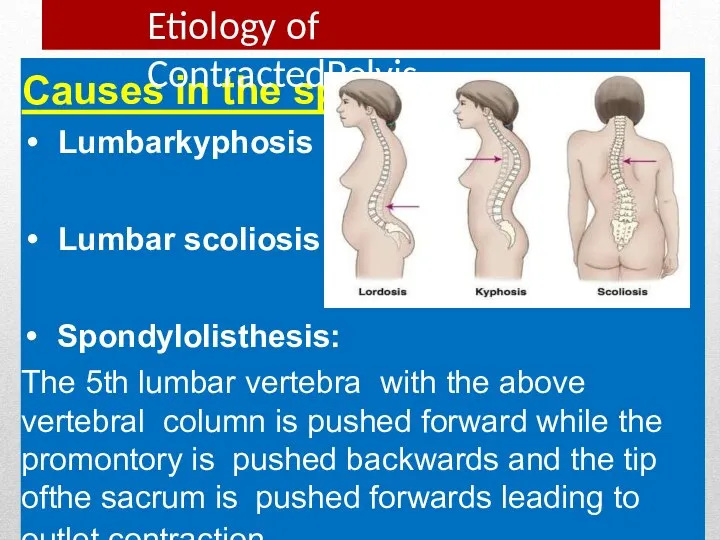
Causes in the spine
Lumbarkyphosis
Lumbar scoliosis
Spondylolisthesis:
The 5th lumbar vertebra with the above vertebral
Causes in the spine
Lumbarkyphosis
Lumbar scoliosis
Spondylolisthesis:
The 5th lumbar vertebra with the above vertebral
Causes in the lower limbs
Dislocation of one or bothfemurs.
Atrophy ofone or
Causes in the lower limbs
Dislocation of one or bothfemurs.
Atrophy ofone or
Pelvis
History
Rickets: is expected if there is a history of delayed walking
Pelvis
History
Rickets: is expected if there is a history of delayed walking
Examination
General examination:
Gait: abnormal gait suggesting abnormalities in the pelvis, spines or
Examination
General examination:
Gait: abnormal gait suggesting abnormalities in the pelvis, spines or
Examinat ion
General examination:
Manifestations of rickets as:
square head
rosary beads in the costalridges.
pigeon
Examinat ion
General examination:
Manifestations of rickets as:
square head
rosary beads in the costalridges.
pigeon
Abdominal examination:
Nonengagement of the head:
in the last 3-4 weeks in primigravida.
Pendulous abdomen:
in
Abdominal examination:
Nonengagement of the head:
in the last 3-4 weeks in primigravida.
Pendulous abdomen:
in
Pelvimetry :
It is assessment of the pelvic diameters and capacity done at
Pelvimetry :
It is assessment of the pelvic diameters and capacity done at
Pelvimetry:
2.Imaging pelvimetry:
X-ray.
Computed tomography (CT).
Magnetic resonance imaging (MRI) .
N.B. CTand MRI are
Pelvimetry:
2.Imaging pelvimetry:
X-ray.
Computed tomography (CT).
Magnetic resonance imaging (MRI) .
N.B. CTand MRI are
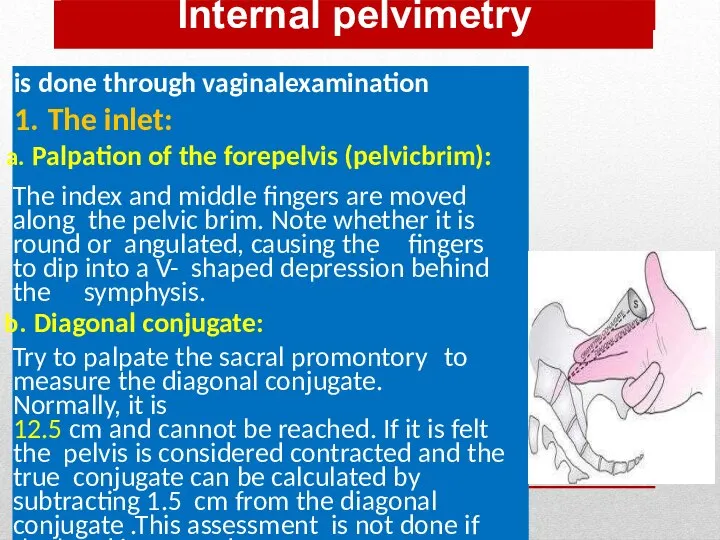
Internal pelvimetry
is done through vaginalexamination
1. The inlet:
Palpation of the forepelvis (pelvicbrim):
The index
Internal pelvimetry
is done through vaginalexamination
1. The inlet:
Palpation of the forepelvis (pelvicbrim):
The index
Internal pelvimetry
2.The cavity:
Height, thickness and inclination of the symphysis.
Shape and inclination
Internal pelvimetry
2.The cavity:
Height, thickness and inclination of the symphysis.
Shape and inclination
2.The cavity:
d.Ischial spines:
Whether it is blunt (difficult to identify at all), prominent
2.The cavity:
d.Ischial spines:
Whether it is blunt (difficult to identify at all), prominent
2.The cavity:
e.Interspinous diameter: By using the 2 examining fingers, if both
2.The cavity:
e.Interspinous diameter: By using the 2 examining fingers, if both
3- The outlet:
Subpubic angle: Normally, it admits 2fingers.
Mobility of the coccyx:
3- The outlet:
Subpubic angle: Normally, it admits 2fingers.
Mobility of the coccyx:
External pelvimetry
Thom’s, Jarcho’s or crossing pelvimeter can be used for external
External pelvimetry
Thom’s, Jarcho’s or crossing pelvimeter can be used for external
Radiological pelvimetry
Lateral view:
The patient stands with the X-ray tube on one side and
Radiological pelvimetry
Lateral view:
The patient stands with the X-ray tube on one side and
Cephalometry
Ultrasonography: is the safe accurate and easy method and can detect:
The
Cephalometry
Ultrasonography: is the safe accurate and easy method and can detect:
The
Cephalopelvic disproportion tests
These are done to detect contracted inlet if the head
Cephalopelvic disproportion tests
These are done to detect contracted inlet if the head
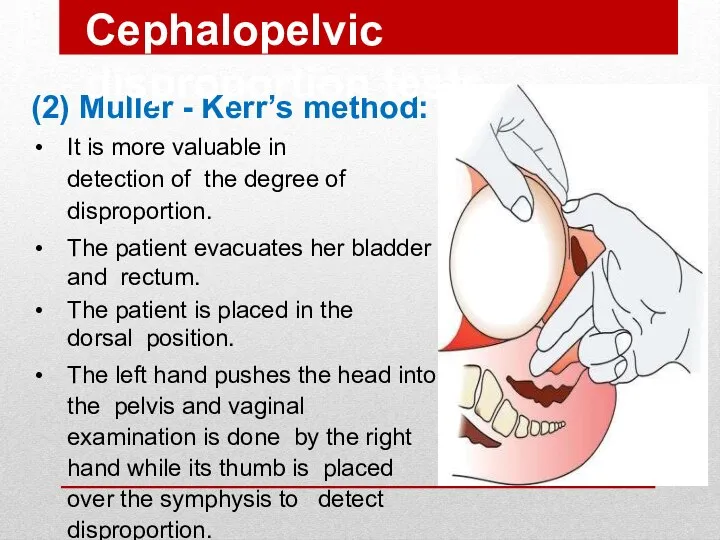
(2) Muller - Kerr’s method:
It is more valuable in detection of
(2) Muller - Kerr’s method:
It is more valuable in detection of
Degrees of Disproportion
Minor disproportion:
The anterior surface of the head is in
Degrees of Disproportion
Minor disproportion:
The anterior surface of the head is in
Degrees of Contracted Pelvis
Minor degree: The true conjugate is 9-10 cm.
Degrees of Contracted Pelvis
Minor degree: The true conjugate is 9-10 cm.
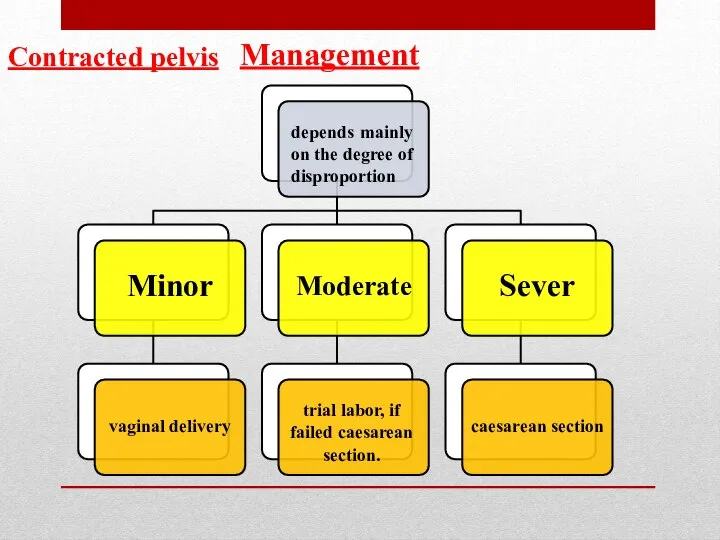
Management
depends mainly on the degree of disproportion
Minor
vaginal delivery
Moderate
trial labor, if failed
Management
depends mainly on the degree of disproportion
Minor
vaginal delivery
Moderate
trial labor, if failed
Trial of Labour
It is a clinical test for the factors that
Trial of Labour
It is a clinical test for the factors that
Procedure :
Trial is carried out in a hospital where facilities for
Procedure :
Trial is carried out in a hospital where facilities for
Indications of trial of labour:
Young primigravida of good health.
Moderate disproportion.
Vertex presentation.
No
Indications of trial of labour:
Young primigravida of good health.
Moderate disproportion.
Vertex presentation.
No
Termination of trial of labour:
Vaginal delivery: either spontaneously or by forceps if
Termination of trial of labour:
Vaginal delivery: either spontaneously or by forceps if
Indications of caesarean section in contracted pelvis
Moderate disproportion if trial of labour is
Indications of caesarean section in contracted pelvis
Moderate disproportion if trial of labour is
Complications
Maternal
Fetal
Contracted pelvis
Complications
Maternal
Fetal
Contracted pelvis
Maternal:
During pregnancy:
Incarcerated retroverted gravid uterus.
Malpresentations.
Pendulous abdomen.
Nonengagement.
Pyelonephritis especial y in high assimilation
Maternal:
During pregnancy:
Incarcerated retroverted gravid uterus.
Malpresentations.
Pendulous abdomen.
Nonengagement.
Pyelonephritis especial y in high assimilation
Complications of Contracted Pelvis
During labour:
Inertia, slow cervical dilatation and prolonged labour.
Premature rupture
Complications of Contracted Pelvis
During labour:
Inertia, slow cervical dilatation and prolonged labour.
Premature rupture
Foetal:
Intracranial haemorrhage.
Asphyxia.
Fracture skull.
Nerve injuries.
Intra-amniotic infection.
Complications of Contracted Pelvis
Foetal:
Intracranial haemorrhage.
Asphyxia.
Fracture skull.
Nerve injuries.
Intra-amniotic infection.
Complications of Contracted Pelvis
 Проект Прикамский фермер
Проект Прикамский фермер Материалы для дистанционной поддержки учащихся по дополнительной программе
Материалы для дистанционной поддержки учащихся по дополнительной программе Отчет Твой друг ПишиСчитай
Отчет Твой друг ПишиСчитай Аналого-цифровые преобразователи (АЦП)
Аналого-цифровые преобразователи (АЦП) Этот День Победы!
Этот День Победы! Анализ сравнения тампонажного материала на основе применения алюмосиликатных микросфер
Анализ сравнения тампонажного материала на основе применения алюмосиликатных микросфер Новелла
Новелла Творим вместе – мастер классы для творчества всей семьей
Творим вместе – мастер классы для творчества всей семьей 10-1
10-1 Работа с картами
Работа с картами ДОПОЛНИТЕЛЬНЫЕ ЗАДАНИЯ 1
ДОПОЛНИТЕЛЬНЫЕ ЗАДАНИЯ 1 тема16, 10 вопрос
тема16, 10 вопрос Выявление антропогенных изменений в экосистемах своей местности
Выявление антропогенных изменений в экосистемах своей местности Общие сведения о компьютере
Общие сведения о компьютере День матери
День матери 03.Тема Будь человеком,С.Михалков
03.Тема Будь человеком,С.Михалков 20120409_krymskaya_voyna1853-1856_gg_034
20120409_krymskaya_voyna1853-1856_gg_034 20140213_rytsarskiy_turnir_-_prezentatsiya
20140213_rytsarskiy_turnir_-_prezentatsiya Сегодня самый прекрасный день
Сегодня самый прекрасный день Цифровое религиоведение
Цифровое религиоведение Проблема строительства зданий в зоне вечной мерзлоты
Проблема строительства зданий в зоне вечной мерзлоты Сверление металла
Сверление металла Интеллектуальная игра по мотивам шоу Где логика
Интеллектуальная игра по мотивам шоу Где логика Схема проезда в компанию Konica Minolta
Схема проезда в компанию Konica Minolta Star Wars. В гонке за космическими ресурсами
Star Wars. В гонке за космическими ресурсами Будни шиномонтажников СберТеха: как Gradle помогает собирать крупнейшую Корпоративную сервисную шину
Будни шиномонтажников СберТеха: как Gradle помогает собирать крупнейшую Корпоративную сервисную шину Дидактическая игра Назови и расскажи о главных православных праздниках
Дидактическая игра Назови и расскажи о главных православных праздниках Изуальный осмотр помещений, проводимый для выявления возможно внедрённых средств съёма информации
Изуальный осмотр помещений, проводимый для выявления возможно внедрённых средств съёма информации