- Trauma + ATLS

Содержание
- 2. The Advanced Trauma Life Support (ATLS) Safe and reliable method for the immediate treatment of injured
- 3. ABCDE: Airway with cervical spine protection Breathing Circulation, stop the bleeding Disability or neurologic status Exposure
- 4. A and B: Speech
- 7. Chin-Lift Maneuver: In the chin-lift maneuver, the fingers of one hand are placed under the mandible,
- 8. Jaw-Thrust Maneuver : The jaw-thrust maneuver is performed by grasping the angles of the lower jaw,
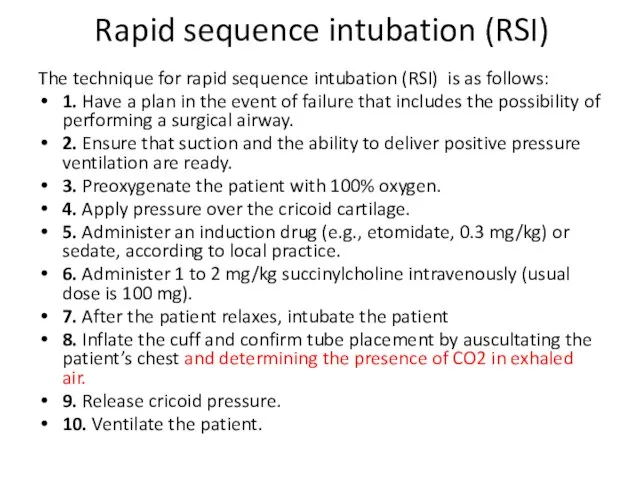
- 10. Rapid sequence intubation (RSI) The technique for rapid sequence intubation (RSI) is as follows: 1. Have
- 11. Approximate PaO2 Versus O2 Hemoglobin Saturation Levels PaO2 LEVELS O2 HEMOGLOBIN SATURATION LEVELS 90 mm Hg
- 12. Surgical Cricothyroidotomy
- 13. B: Breathing Evaluation: visualizing chest movement auscultating breath sounds measuring oxygen saturation What if problematic ?
- 14. C-circulation
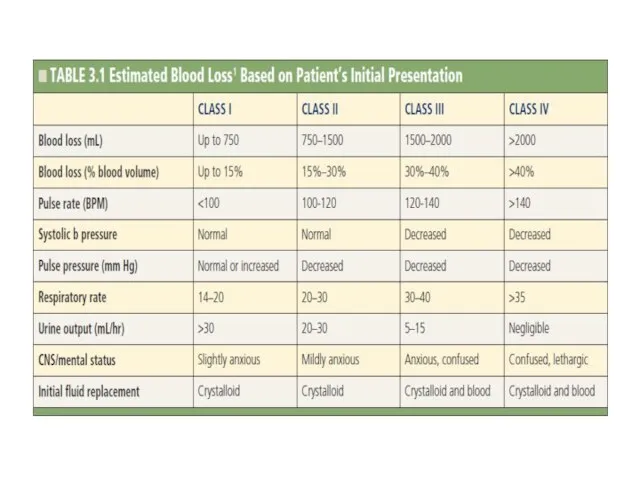
- 15. In most cases, tachycardia is the earliest measurable circulatory sign of shock
- 19. C: Venous access Intraosseous
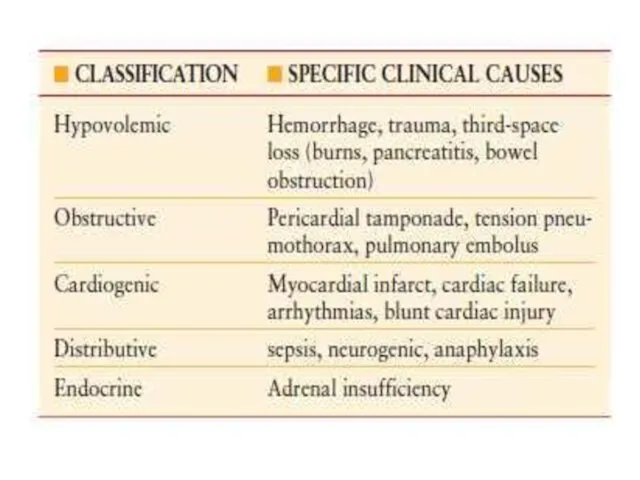
- 20. C: Circulation 5 Life-threating blood loss causes: external blood loss chest abdomen, Retroperitoneum (pelvic fracture) multiple
- 21. Resuscitative Thoracotomy When? ? critic injury and Cardiac arrest For what? Opportunity to open pericardium ?
- 23. REBOA resuscitative endovascular balloon occlusion of the aorta Obtainig temporary hemorrhage control in the agonal patient
- 24. D
- 26. D: Disability Neurological function evaluation: Neurogenic shock? Spinal cord injury? Body temprature? ? Keep the patient
- 27. :E Head to toe PR Xray FAST NGT Urine catheter
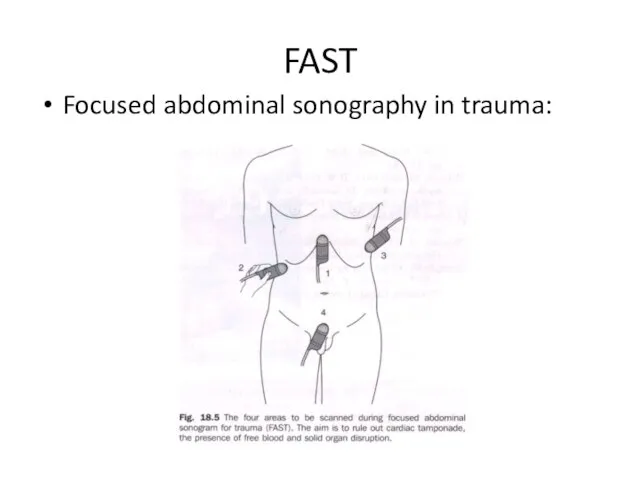
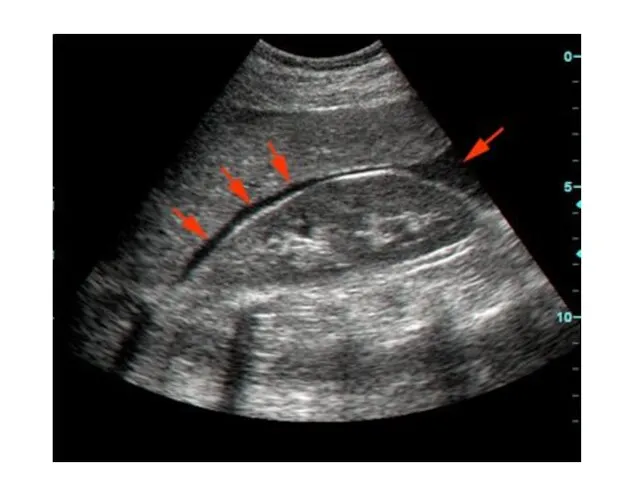
- 34. FAST Focused abdominal sonography in trauma:
- 37. HEAD INJURY
- 39. Epidural hematomas typically result from a lateral fracture of the cranium causing bleeding from the middle
- 40. Subdural hematomas are commonly caused by tearing of the bridging veins between the dura mater and
- 42. Parenchymal contusions of brain tissue result from the direct transmission of energy to the cranium and
- 43. Diffuse axonal injury describes the phenomenon of disruption of the axon from the neuronal body secondary
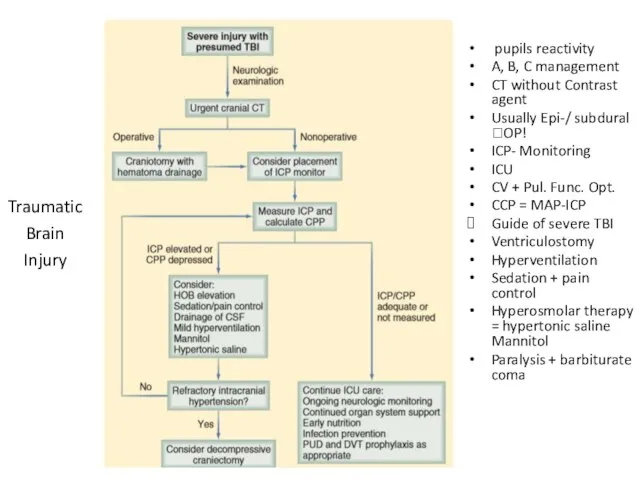
- 45. pupils reactivity A, B, C management CT without Contrast agent Usually Epi-/ subdural ?OP! ICP- Monitoring
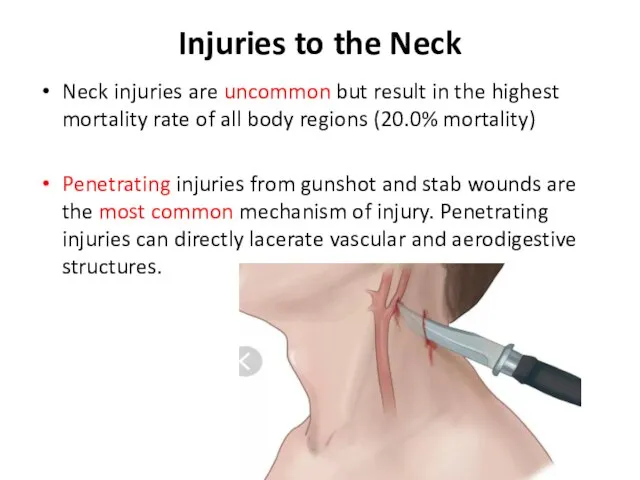
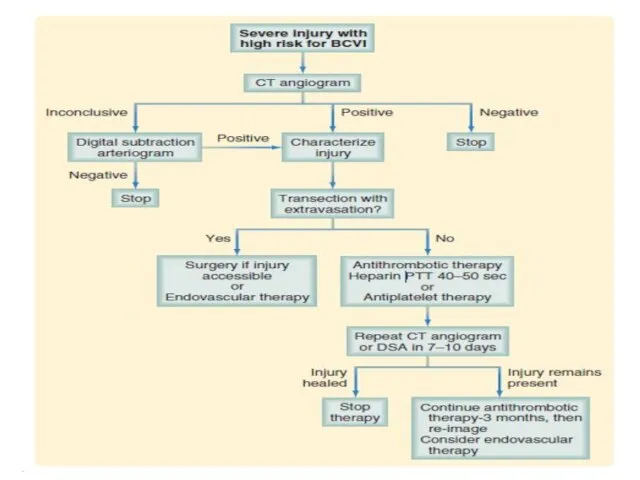
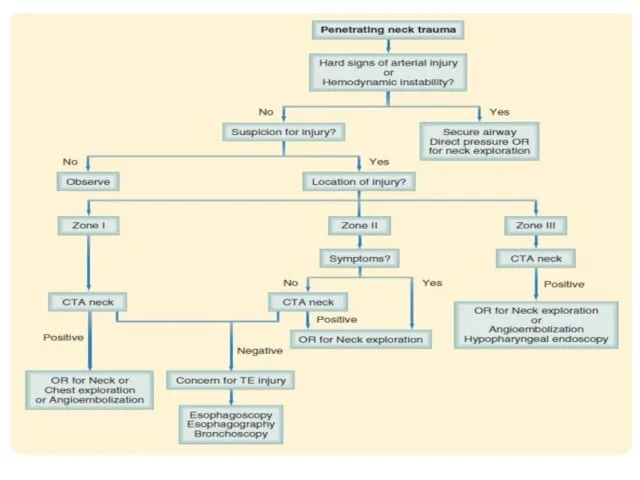
- 47. Injuries to the Neck Neck injuries are uncommon but result in the highest mortality rate of
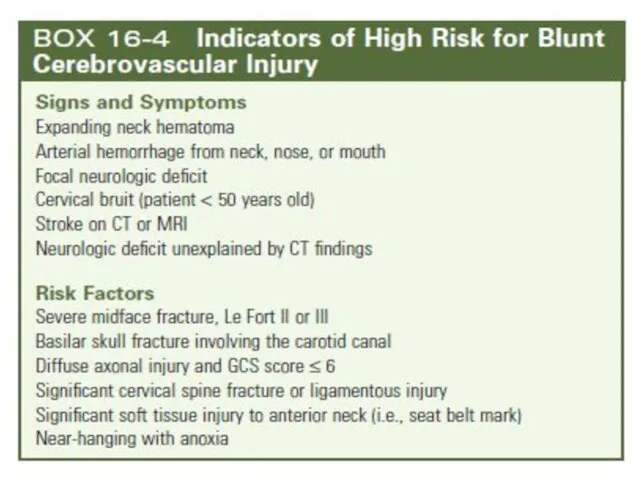
- 48. Blunt mechanisms can cause compression, with fracture of the larynx or trachea. Blunt pharyngeal or esophageal
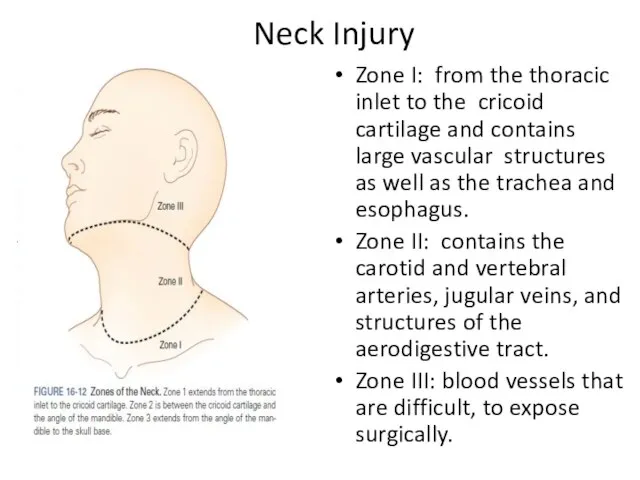
- 51. Neck Injury Zone I: from the thoracic inlet to the cricoid cartilage and contains large vascular
- 53. CHEST INJURY With more than 65% of blunt trauma patients sustaining one or more rib fractures,
- 54. Flail Chest : This condition usually results from trauma associated with multiple rib fractures—that is, two
- 55. Flail chest > Solitary independent movement of the Fx Paradoxical breathing Hypoxemia due to pulmonary contusion
- 57. Thoracic injury
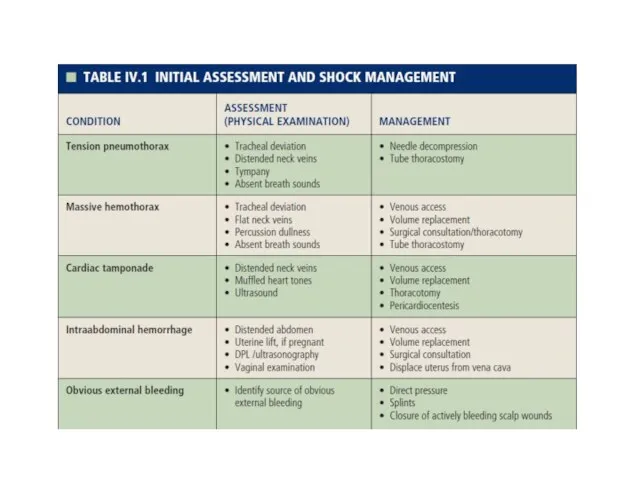
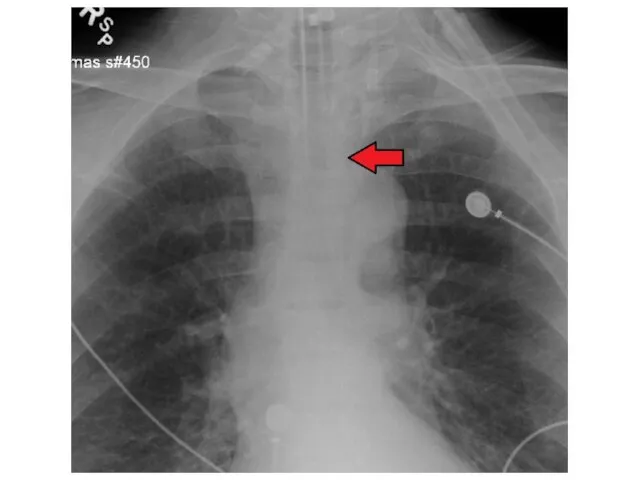
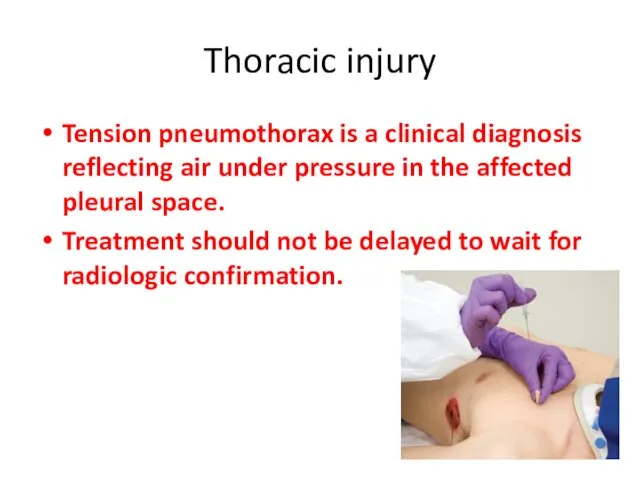
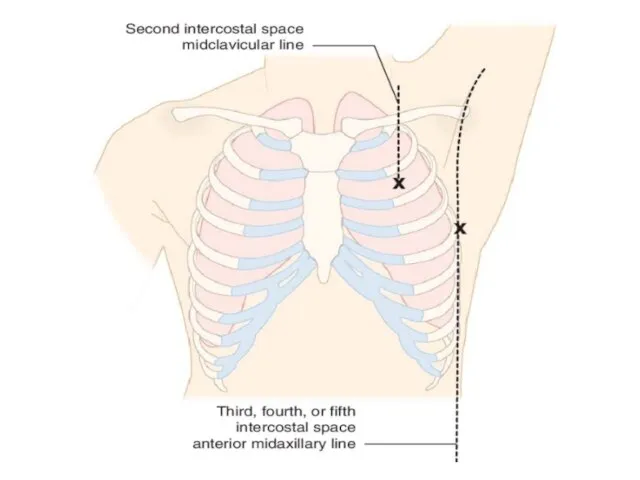
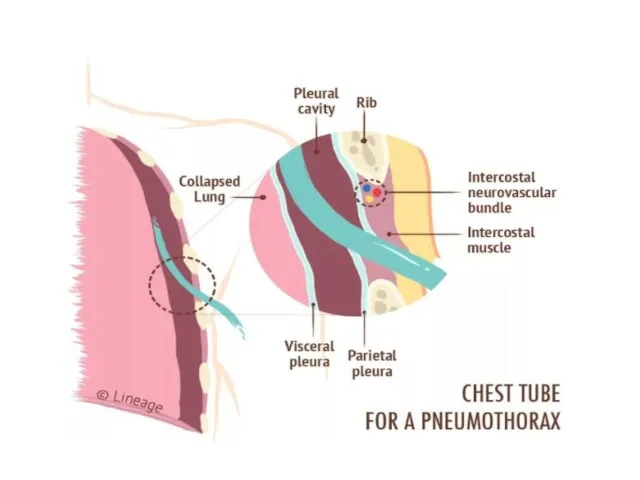
- 58. Thoracic injury Tension pneumothorax is a clinical diagnosis reflecting air under pressure in the affected pleural
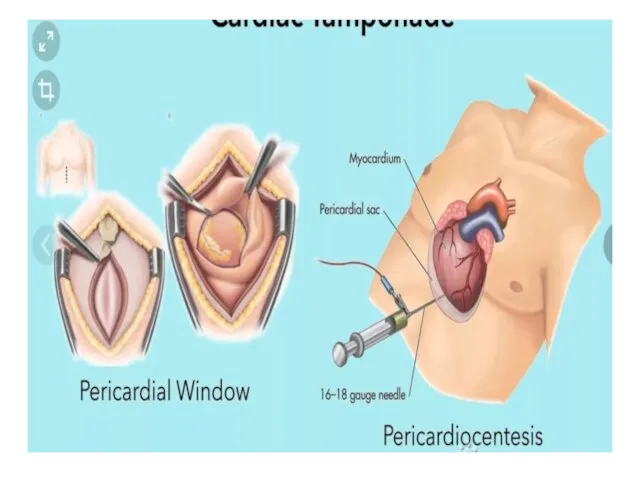
- 61. Cardiac tamponade is indicated by the presence of the classic diagnostic Beck’s triad: venous pressure elevation,
- 63. Massive hemothorax results from the rapid accumulation of more than 1500 mL of blood or one-third
- 65. Thoracic injury Pulmonary injuries. Lung injuries are common after chest trauma, with 31.9% of patients Mortality
- 66. Cardiac injuries uncommon, but most severe injuries sustained by patients after penetrating and blunt trauma. Penetrating
- 67. Blunt injury to the heart occurs less commonly, being seen in only 2.2% of blunt chest
- 68. Tracheobronchial injuries Tracheobronchial tree injuries are uncommon but are associated with significant morbidity and mortality. Penetrating
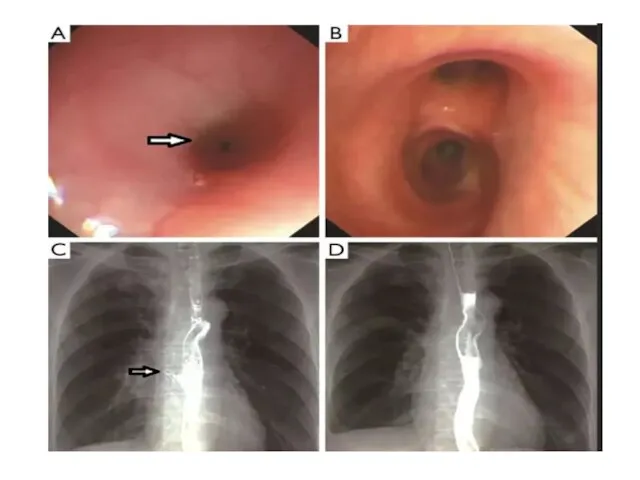
- 69. Esophageal injuries: The thoracic esophagus is uncommonly injured Penetrating injury is more common, but only 1.6%
- 70. The esophagus is best evaluated through a combination of contrast esophagography and esophagoscopy Together these two
- 72. The upper and midthoracic esophagus is best approached through a right posterolateral thoracotomy through the fourth
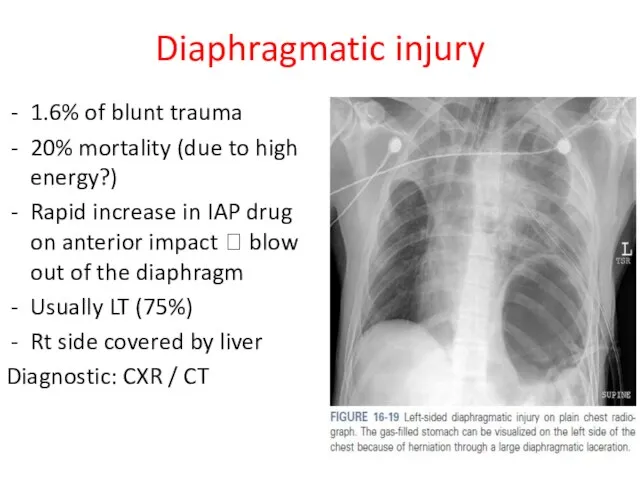
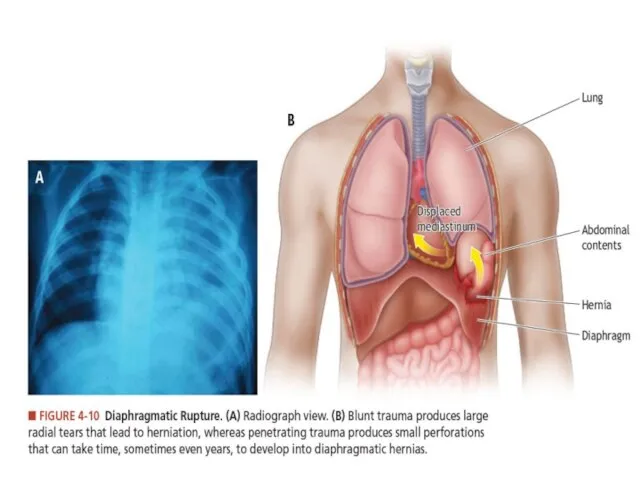
- 73. Diaphragmatic injury 1.6% of blunt trauma 20% mortality (due to high energy?) Rapid increase in IAP
- 75. Abdominal trauma
- 78. Indication for OR Penetration of fascia Unstable patient NGT-blood PR- blood
- 80. SPLEEN The spleen is the most commonly injured abdominal organ with 23.8% of patients with abdominal
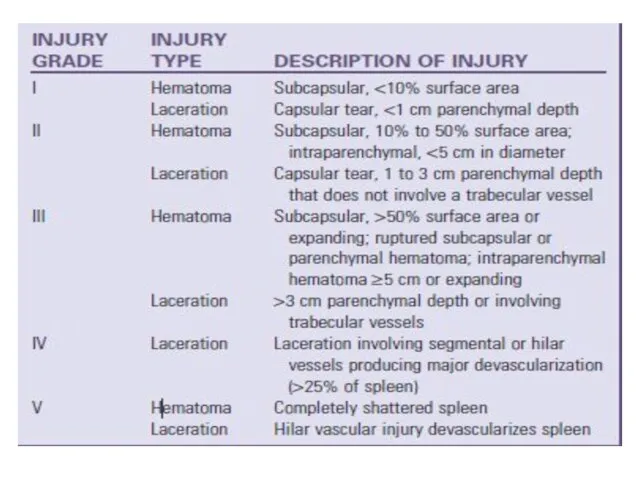
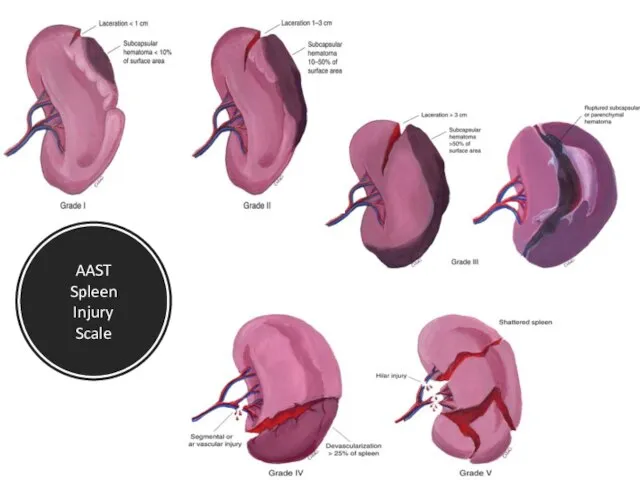
- 82. AAST Spleen Injury Scale
- 84. Management of spleen Injury No preferable management Depends on surgeon’s preference Recommended: I, II, III ?
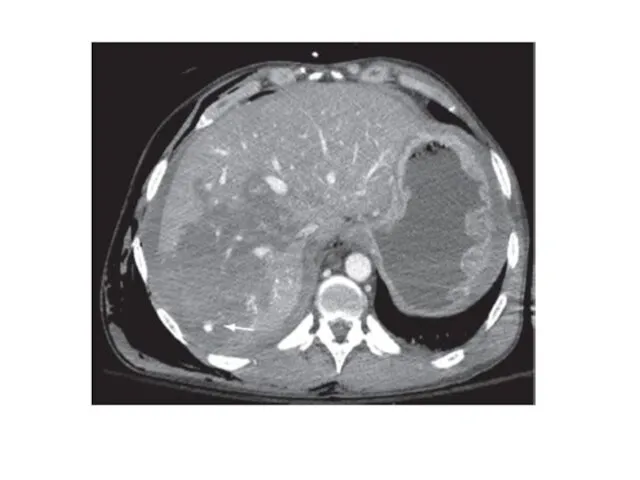
- 85. Hepatic injuries: Liver injuries are extremely common after blunt trauma; only the spleen demonstrates a higher
- 88. Hepatic Injury Mechanism: compression with direct parenchymal damage and shearing forces ? tears in hepatic tissues?
- 91. Hepatic Injury - Management Hemodynamically instable patient ? OPERATION Conditions or non-operative management: No tachycardia, no
- 92. Non-surgical hepatic injury treatment Complications abdominal compartment syndrome bile duct injury leading to bile peritonitis or
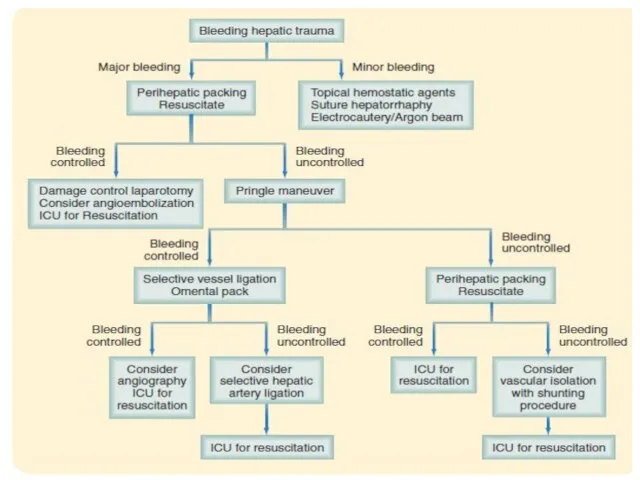
- 93. Surgical management of liver Injury options Packing Pringle Push Plug
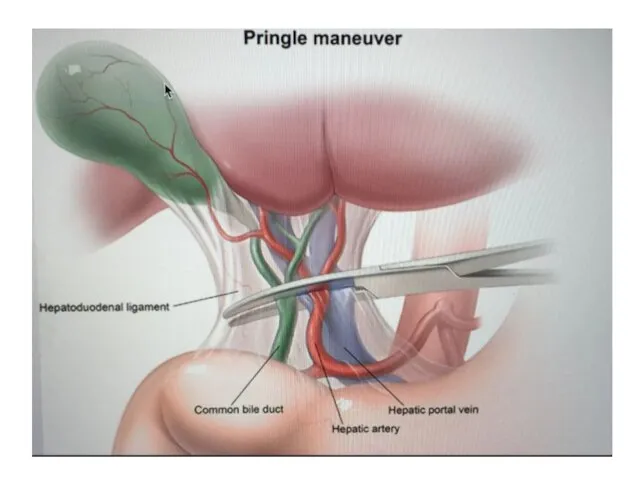
- 94. Surgical management of liver Injury Perihepatic sponges Manual pressure When stable – remove packing and reevaluate
- 96. Gastric injuries Penetrating mechanisms are the most common cause of injuries to the stomach, with these
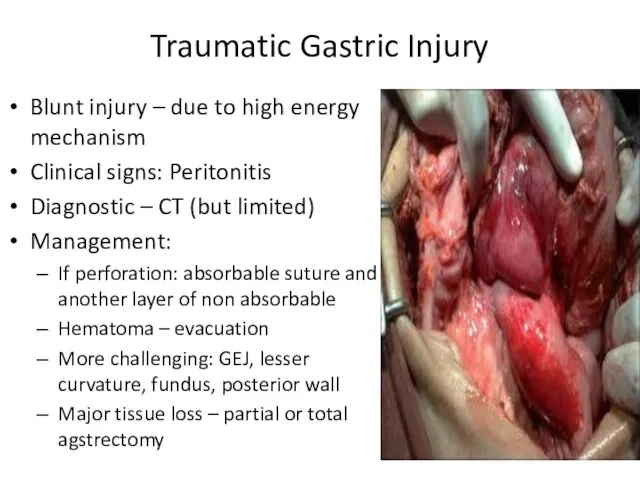
- 97. Traumatic Gastric Injury Blunt injury – due to high energy mechanism Clinical signs: Peritonitis Diagnostic –
- 98. Duodenal injuries Duodenal injuries are uncommon after blunt and penetrating trauma but can pose a diagnostic
- 99. Duodenal injury Children bicycle handlebar or steering wheel stucking in drivers Clinic: Do not expect peritonitis!
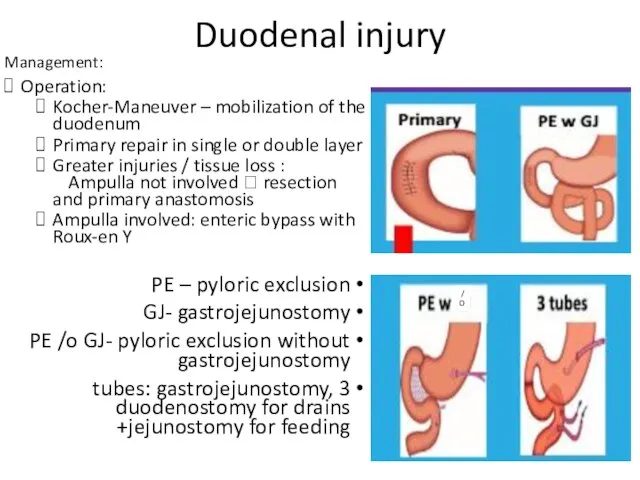
- 100. Duodenal injury Management: Operation: Kocher-Maneuver – mobilization of the duodenum Primary repair in single or double
- 101. Small bowel injuries The small intestine is one of the more frequently injured organs after penetrating
- 102. Small bowel injury Management: Primary repair – when no stricture Resection with anastomosis Resection without anastomosis
- 103. Colon injuries Colon and rectal injuries occur most commonly after penetrating abdominal trauma and rarely after
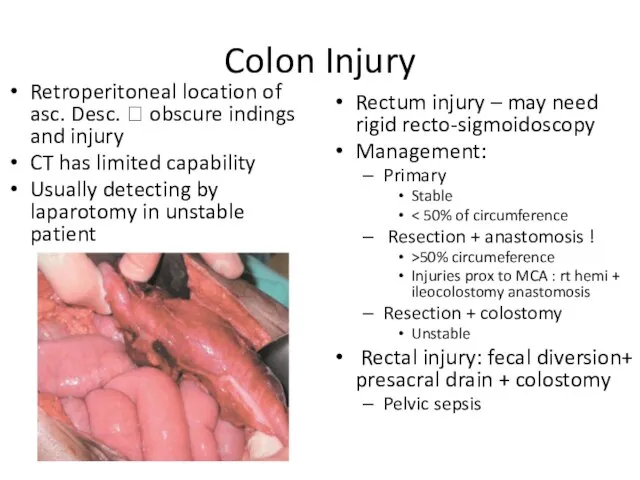
- 104. Colon Injury Retroperitoneal location of asc. Desc. ? obscure indings and injury CT has limited capability
- 105. Pancreatic injuries Pancreatic injuries commonly occur in association with injury to the duodenum because of their
- 106. Pancreas tissue injury can result from direct laceration of the organ or through the transmission of
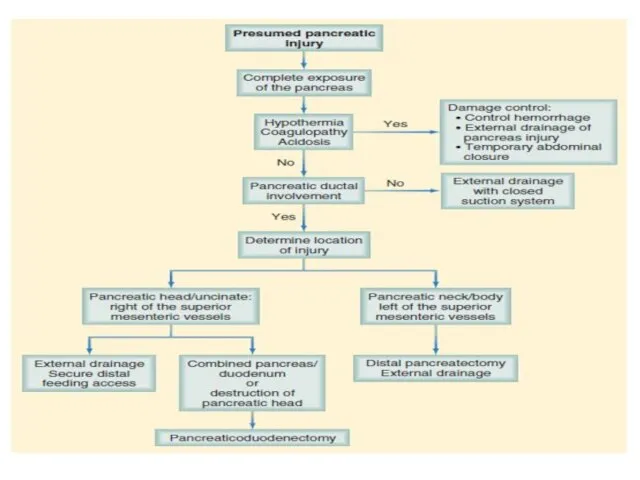
- 108. Management of Pancreatic Injury Operation in any significance Location of injury determines the surgical plan: Left
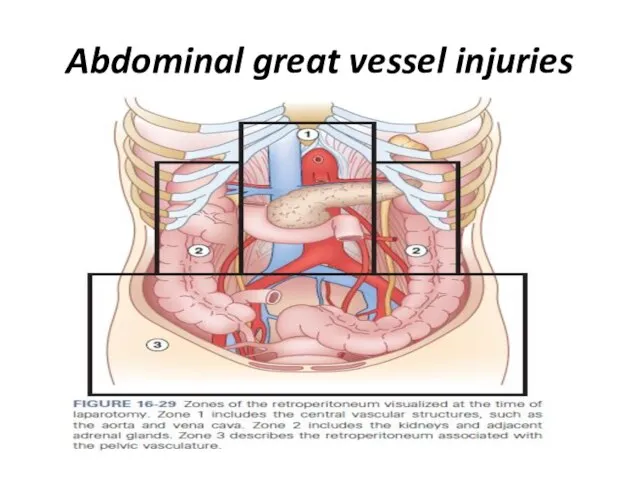
- 109. Abdominal great vessel injuries
- 110. The major blood vessels of the abdomen are predominantly located within the retroperitoneum, with some larger
- 111. The retroperitoneum can be divided into three zones: Zone 1 hematomas require exploration because these frequently
- 112. A hematoma in the region of zone 2, which predominantly contains the kidneys, should be explored
- 113. Abdominal great vessel Injuries I – central hematoma Aorta, prox. visceral vessels, inferior vena cava Always
- 114. Genitourinary injuries The genitourinary organs include the kidneys, ureters, bladder, and urethra, all of which are
- 115. Intraperitoneal bladder injuries can be repaired in two layers of absorbable suture and the bladder drained
- 116. Genitourinary Injury Kidney ureter bladder urethra Clinic: (gross hematuria), Bleeding , extravasation of urine Mechanism: energy
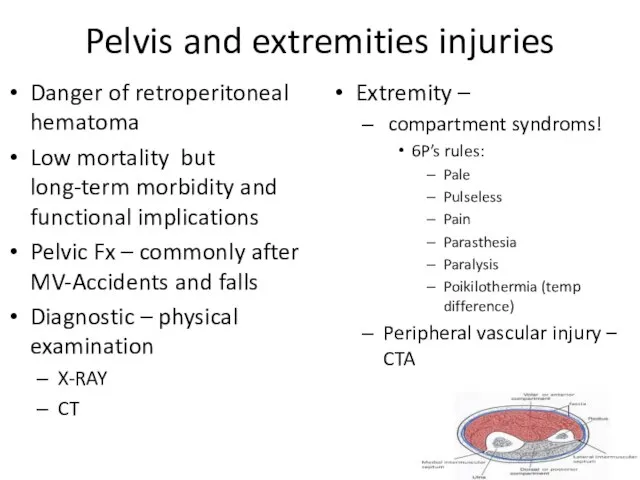
- 117. Pelvis and extremities injuries Danger of retroperitoneal hematoma Low mortality but long-term morbidity and functional implications
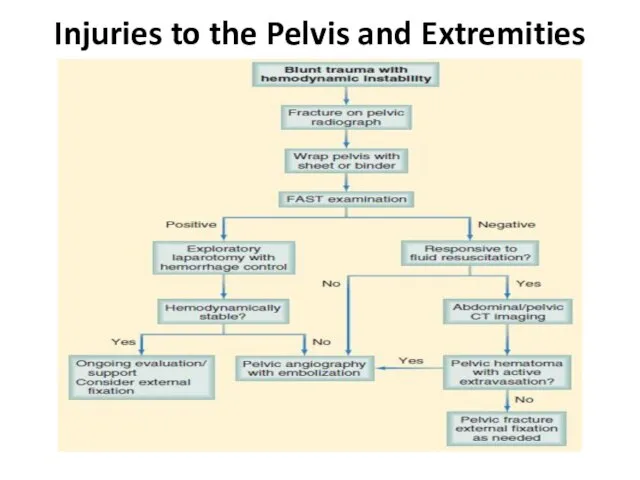
- 118. Injuries to the Pelvis and Extremities
- 119. In which of the following the pulse pressure is normal? A. Shock class I B. Shock
- 120. A 30 - year - old male is brought to the trauma unit due to chest
- 121. 22 - year - old male is brought to the trauma unit following a gun -
- 122. A 36 years old male was involved in a vehicle accident on exam at the ER
- 123. 21-years old man arrives in the emergency department with a stab wound to the left chest
- 124. A 40 years old male is status post-splenectomy following a motor vehicle accident 10 years ago,
- 125. A 15-years-old girl fall while cycling. in the ER. 8 hours later she complains of left
- 126. A 40 year old male is admitted to the ER following stab wound to the abdomen.
- 128. Скачать презентацию
The Advanced Trauma Life Support (ATLS)
Safe and reliable method for
The Advanced Trauma Life Support (ATLS)
Safe and reliable method for
ABCDE:
Airway with cervical spine protection
Breathing
Circulation, stop the bleeding
Disability or neurologic status
Exposure
ABCDE:
Airway with cervical spine protection
Breathing
Circulation, stop the bleeding
Disability or neurologic status
Exposure
A and B:
Speech
A and B:
Speech

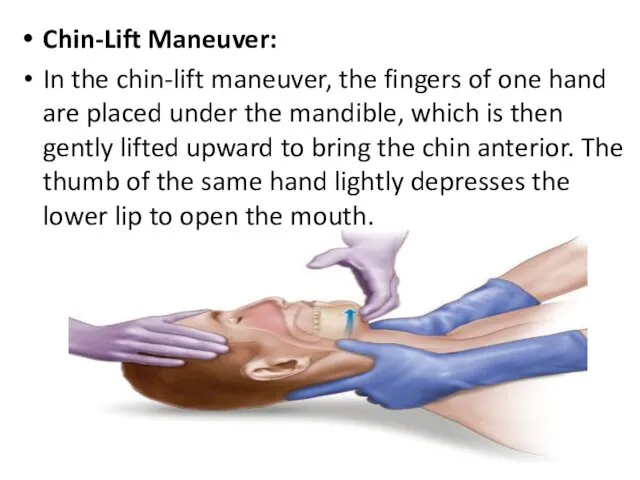
Chin-Lift Maneuver:
In the chin-lift maneuver, the fingers of one hand are
Chin-Lift Maneuver:
In the chin-lift maneuver, the fingers of one hand are
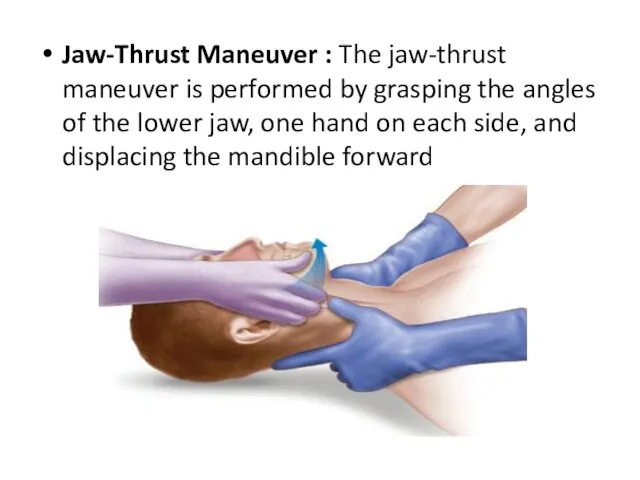
Jaw-Thrust Maneuver : The jaw-thrust maneuver is performed by grasping the
Jaw-Thrust Maneuver : The jaw-thrust maneuver is performed by grasping the

Rapid sequence intubation (RSI)
The technique for rapid sequence intubation (RSI) is
Rapid sequence intubation (RSI)
The technique for rapid sequence intubation (RSI) is
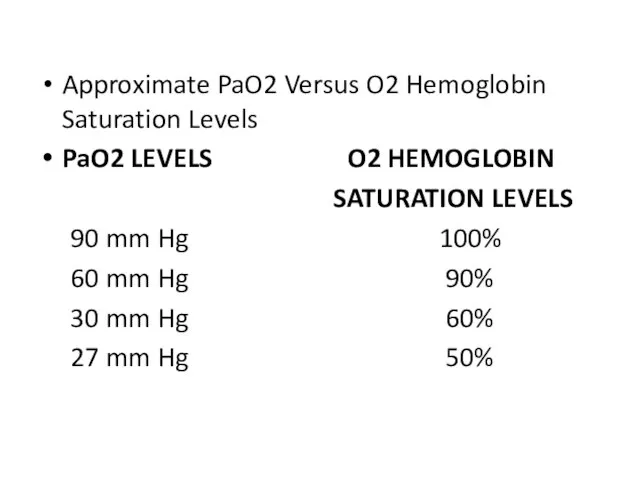
Approximate PaO2 Versus O2 Hemoglobin Saturation Levels
PaO2 LEVELS O2 HEMOGLOBIN
Approximate PaO2 Versus O2 Hemoglobin Saturation Levels
PaO2 LEVELS O2 HEMOGLOBIN
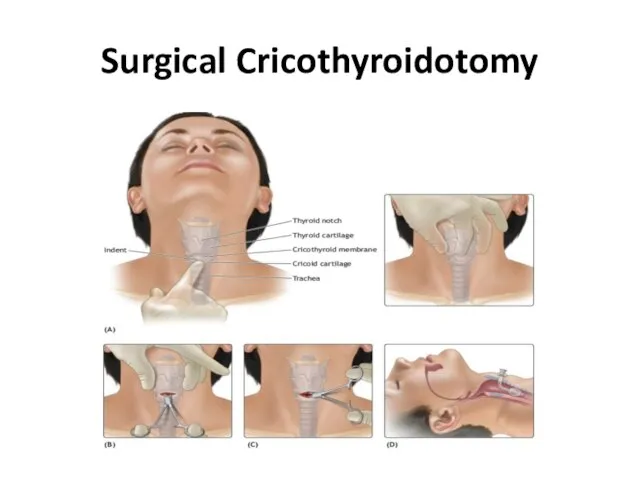
Surgical Cricothyroidotomy
Surgical Cricothyroidotomy
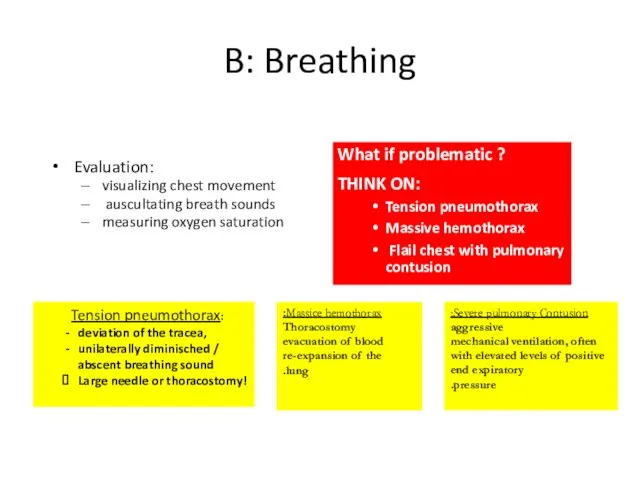
B: Breathing
Evaluation:
visualizing chest movement
auscultating breath sounds
measuring oxygen saturation
What
B: Breathing
Evaluation:
visualizing chest movement
auscultating breath sounds
measuring oxygen saturation
What
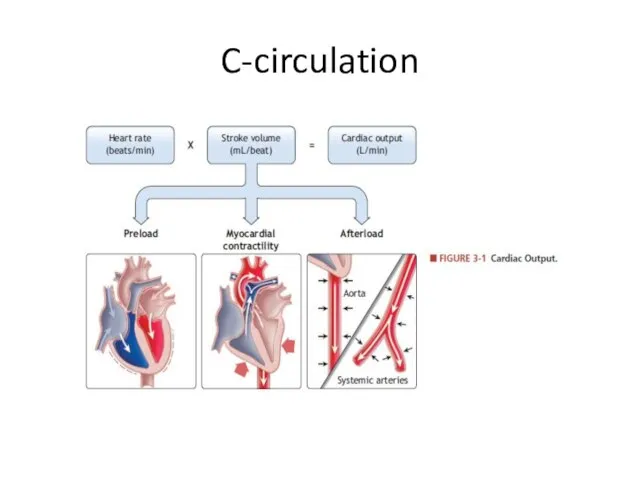
C-circulation
C-circulation
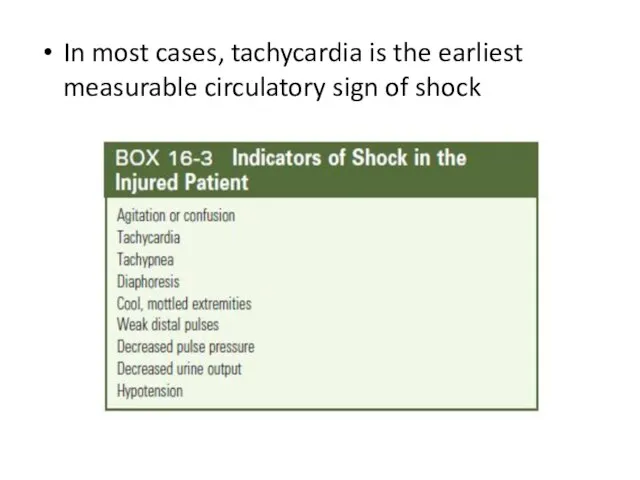
In most cases, tachycardia is the earliest measurable circulatory sign of
In most cases, tachycardia is the earliest measurable circulatory sign of
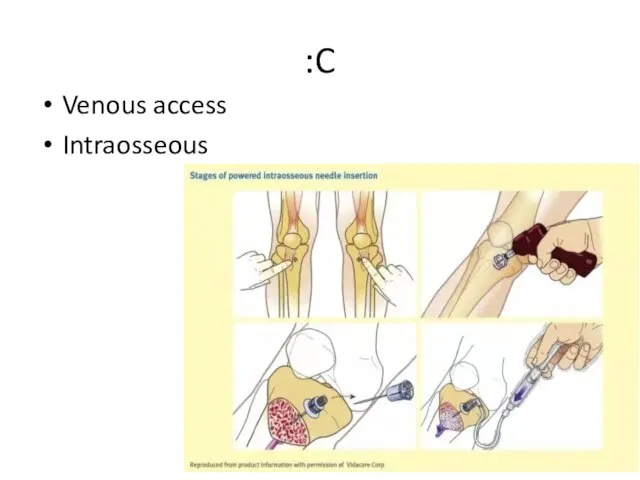
C:
Venous access
Intraosseous
C:
Venous access
Intraosseous
C: Circulation
5 Life-threating blood loss causes:
external blood loss
chest
abdomen,
Retroperitoneum (pelvic
C: Circulation
5 Life-threating blood loss causes:
external blood loss
chest
abdomen,
Retroperitoneum (pelvic
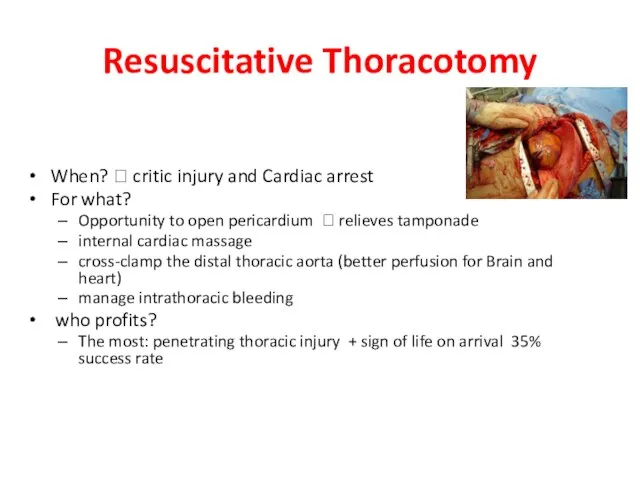
Resuscitative Thoracotomy
When? ? critic injury and Cardiac arrest
For what?
Opportunity to
Resuscitative Thoracotomy
When? ? critic injury and Cardiac arrest
For what?
Opportunity to

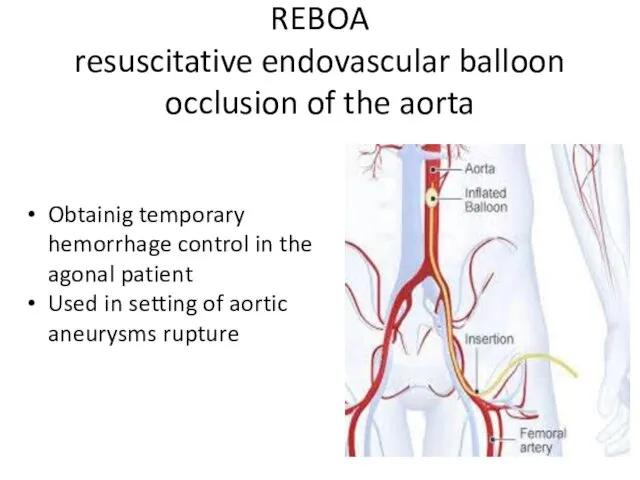
REBOA
resuscitative endovascular balloon occlusion of the aorta
Obtainig temporary hemorrhage control in
REBOA
resuscitative endovascular balloon occlusion of the aorta
Obtainig temporary hemorrhage control in
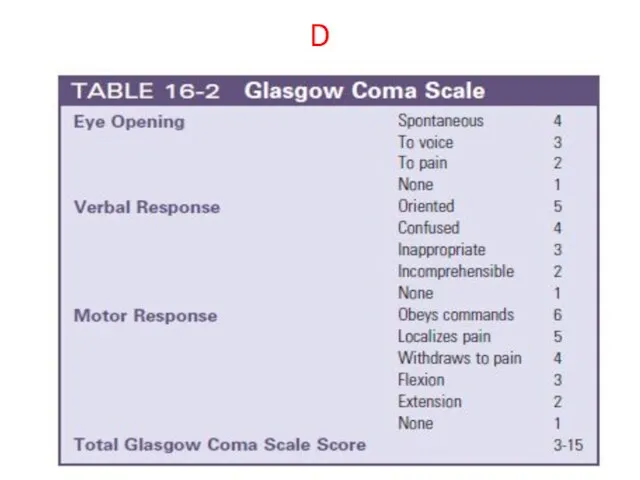
D
D
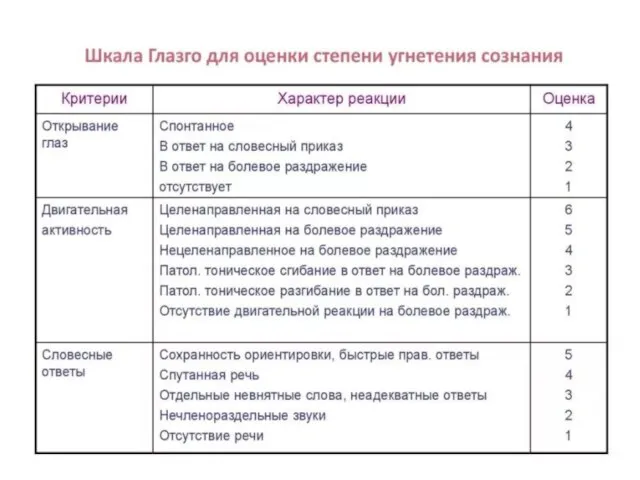
D: Disability
Neurological function evaluation:
Neurogenic shock?
Spinal cord injury?
Body temprature?
?
D: Disability
Neurological function evaluation:
Neurogenic shock?
Spinal cord injury?
Body temprature?
?
:E
Head to toe
PR
Xray
FAST
NGT
Urine catheter
:E
Head to toe
PR
Xray
FAST
NGT
Urine catheter




FAST
Focused abdominal sonography in trauma:
FAST
Focused abdominal sonography in trauma:
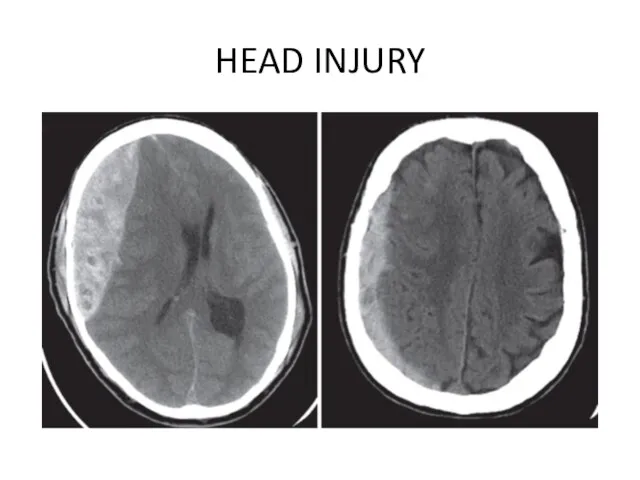
HEAD INJURY
HEAD INJURY
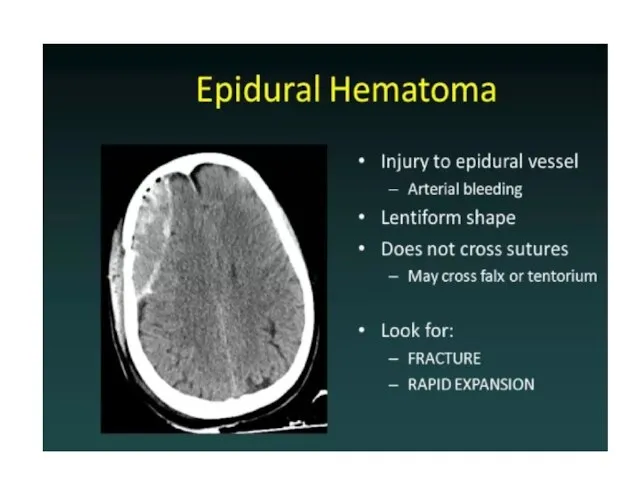
Epidural hematomas typically result from a lateral fracture of the cranium
Epidural hematomas typically result from a lateral fracture of the cranium
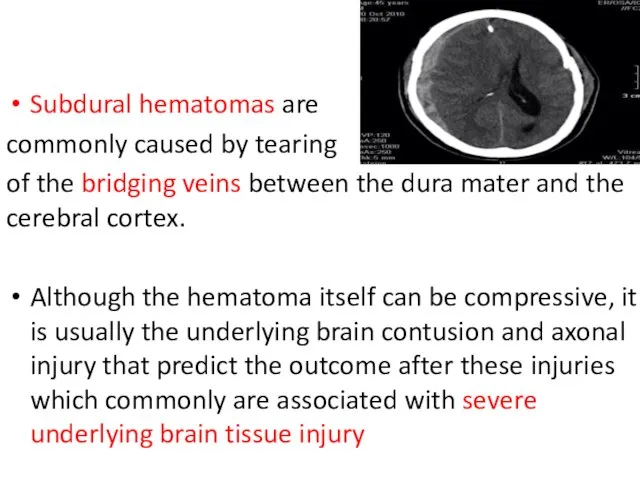
Subdural hematomas are
commonly caused by tearing
of the bridging veins
commonly caused by tearing
of the bridging veins

Parenchymal contusions of brain tissue result from the direct transmission of
Parenchymal contusions of brain tissue result from the direct transmission of
Diffuse axonal injury describes the phenomenon of disruption of the axon
Diffuse axonal injury describes the phenomenon of disruption of the axon
pupils reactivity
A, B, C management
CT without Contrast agent
Usually Epi-/
pupils reactivity
A, B, C management
CT without Contrast agent
Usually Epi-/
Injuries to the Neck
Neck injuries are uncommon but result in the
Injuries to the Neck
Neck injuries are uncommon but result in the
Blunt mechanisms can cause compression, with fracture of the larynx or
Blunt mechanisms can cause compression, with fracture of the larynx or
Neck Injury
Zone I: from the thoracic inlet to the cricoid
Neck Injury
Zone I: from the thoracic inlet to the cricoid
CHEST INJURY
With more than 65% of blunt trauma patients sustaining
CHEST INJURY
With more than 65% of blunt trauma patients sustaining
Flail Chest : This condition usually results from trauma associated with
Flail Chest : This condition usually results from trauma associated with
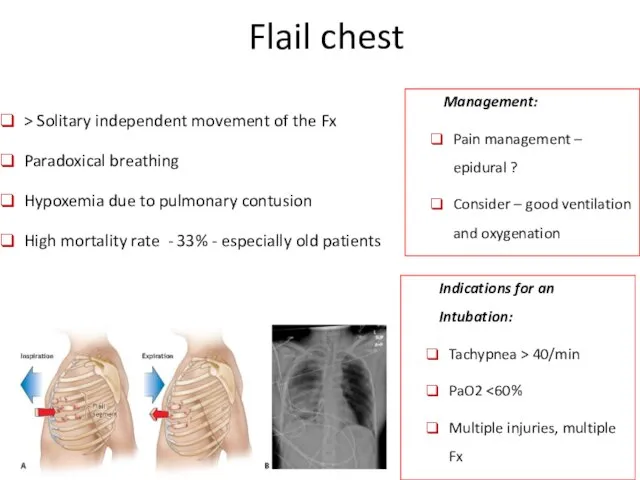
Flail chest
> Solitary independent movement of the Fx
Paradoxical breathing
Flail chest
> Solitary independent movement of the Fx
Paradoxical breathing
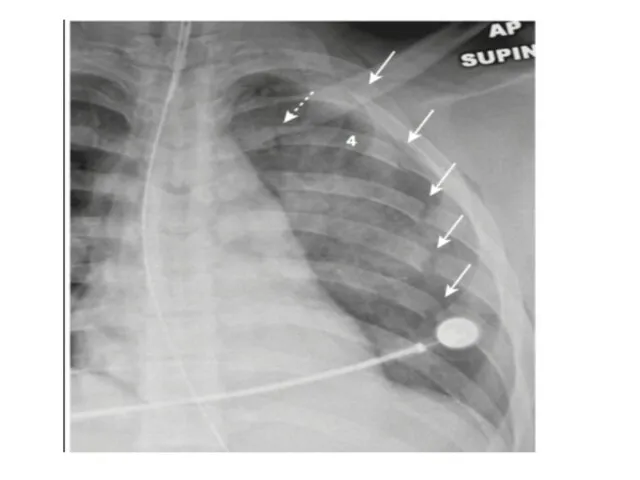
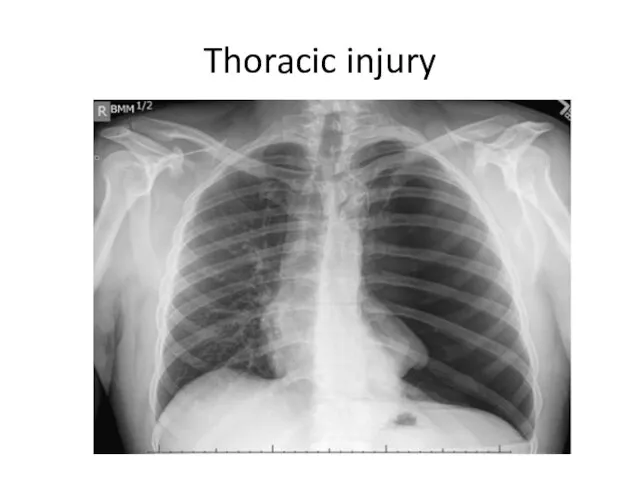
Thoracic injury
Thoracic injury
Thoracic injury
Tension pneumothorax is a clinical diagnosis reflecting air under pressure
Thoracic injury
Tension pneumothorax is a clinical diagnosis reflecting air under pressure
Cardiac tamponade is indicated by the presence of the classic diagnostic
Cardiac tamponade is indicated by the presence of the classic diagnostic
Massive hemothorax results from the rapid accumulation of more than 1500
Massive hemothorax results from the rapid accumulation of more than 1500

Thoracic injury
Pulmonary injuries. Lung injuries are common after chest trauma, with
Thoracic injury
Pulmonary injuries. Lung injuries are common after chest trauma, with
Cardiac injuries uncommon, but most severe injuries sustained by patients after
Cardiac injuries uncommon, but most severe injuries sustained by patients after
Blunt injury to the heart occurs less commonly, being seen in
Blunt injury to the heart occurs less commonly, being seen in
Tracheobronchial injuries
Tracheobronchial tree injuries are uncommon but are associated with significant
Tracheobronchial injuries
Tracheobronchial tree injuries are uncommon but are associated with significant
Esophageal injuries:
The thoracic esophagus is uncommonly injured
Penetrating injury is more
Esophageal injuries:
The thoracic esophagus is uncommonly injured
Penetrating injury is more
The esophagus is best evaluated through a combination of contrast esophagography
The esophagus is best evaluated through a combination of contrast esophagography
The upper and midthoracic esophagus is best approached through a right
The upper and midthoracic esophagus is best approached through a right
Diaphragmatic injury
1.6% of blunt trauma
20% mortality (due to high energy?)
Diaphragmatic injury
1.6% of blunt trauma
20% mortality (due to high energy?)
Abdominal trauma
Abdominal trauma

Indication for OR
Penetration of fascia
Unstable patient
NGT-blood
PR- blood
Indication for OR
Penetration of fascia
Unstable patient
NGT-blood
PR- blood
SPLEEN
The spleen is the most commonly injured abdominal organ with 23.8%
SPLEEN
The spleen is the most commonly injured abdominal organ with 23.8%
AAST
Spleen
Injury
Scale
AAST
Spleen
Injury
Scale
Management of spleen Injury
No preferable management
Depends on surgeon’s preference
Recommended:
Management of spleen Injury
No preferable management
Depends on surgeon’s preference
Recommended:
Hepatic injuries:
Liver injuries are extremely common after blunt trauma; only the
Hepatic injuries:
Liver injuries are extremely common after blunt trauma; only the
Hepatic Injury
Mechanism: compression with direct parenchymal damage and shearing forces ?
Hepatic Injury
Mechanism: compression with direct parenchymal damage and shearing forces ?
Hepatic Injury - Management
Hemodynamically instable patient ? OPERATION
Conditions or non-operative management:
Hepatic Injury - Management
Hemodynamically instable patient ? OPERATION
Conditions or non-operative management:
Non-surgical hepatic injury treatment
Complications
abdominal compartment syndrome
bile duct injury leading to bile
Non-surgical hepatic injury treatment
Complications
abdominal compartment syndrome
bile duct injury leading to bile
Surgical management of liver Injury
options
Packing
Pringle
Push
Plug
Surgical management of liver Injury
options
Packing
Pringle
Push
Plug
Surgical management of liver Injury
Perihepatic sponges
Manual pressure
When stable – remove
Surgical management of liver Injury
Perihepatic sponges
Manual pressure
When stable – remove
Gastric injuries
Penetrating mechanisms are the most common cause of injuries to
Gastric injuries
Penetrating mechanisms are the most common cause of injuries to
Traumatic Gastric Injury
Blunt injury – due to high energy mechanism
Traumatic Gastric Injury
Blunt injury – due to high energy mechanism
Duodenal injuries
Duodenal injuries are uncommon after blunt and penetrating trauma but
Duodenal injuries
Duodenal injuries are uncommon after blunt and penetrating trauma but
Duodenal injury
Children bicycle handlebar or steering wheel stucking in drivers
Clinic:
Duodenal injury
Children bicycle handlebar or steering wheel stucking in drivers
Clinic:
Duodenal injury
Management:
Operation:
Kocher-Maneuver – mobilization of the duodenum
Primary
Duodenal injury
Management:
Operation:
Kocher-Maneuver – mobilization of the duodenum
Primary
Small bowel injuries
The small intestine is one of the more frequently
Small bowel injuries
The small intestine is one of the more frequently
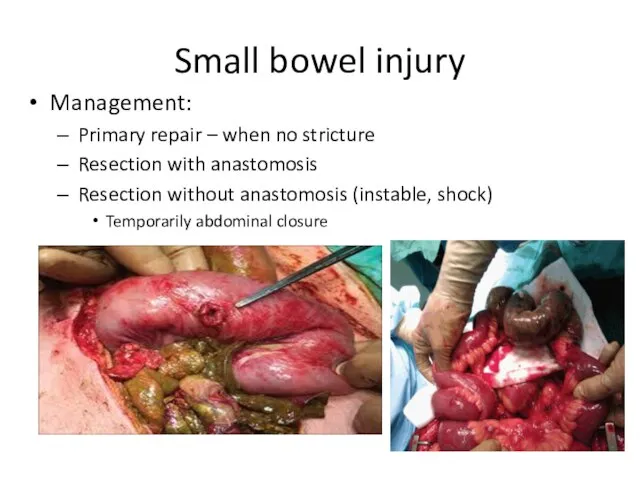
Small bowel injury
Management:
Primary repair – when no stricture
Resection with
Small bowel injury
Management:
Primary repair – when no stricture
Resection with
Colon injuries
Colon and rectal injuries occur most commonly after penetrating
Colon injuries
Colon and rectal injuries occur most commonly after penetrating
Colon Injury
Retroperitoneal location of asc. Desc. ? obscure indings and
Colon Injury
Retroperitoneal location of asc. Desc. ? obscure indings and
Pancreatic injuries
Pancreatic injuries commonly occur in association with injury to the
Pancreatic injuries
Pancreatic injuries commonly occur in association with injury to the
Pancreas tissue injury can result from direct laceration of the organ
Pancreas tissue injury can result from direct laceration of the organ
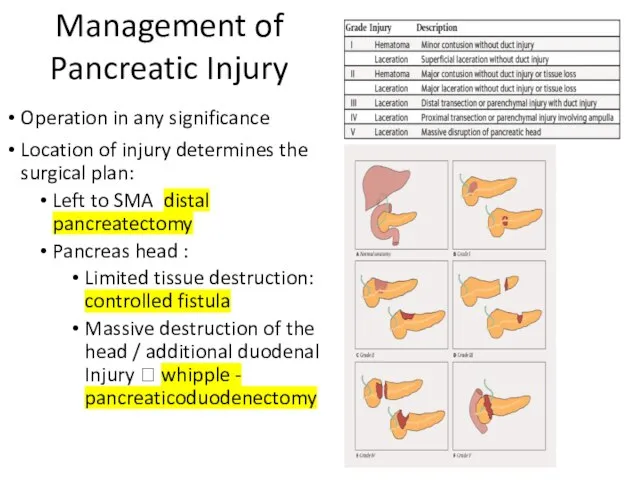
Management of Pancreatic Injury
Operation in any significance
Location of injury determines
Management of Pancreatic Injury
Operation in any significance
Location of injury determines
Abdominal great vessel injuries
Abdominal great vessel injuries
The major blood vessels of the abdomen are predominantly located within
The major blood vessels of the abdomen are predominantly located within
The retroperitoneum can be divided into three zones:
Zone 1 hematomas require
The retroperitoneum can be divided into three zones:
Zone 1 hematomas require
A hematoma in the region of zone 2, which predominantly contains
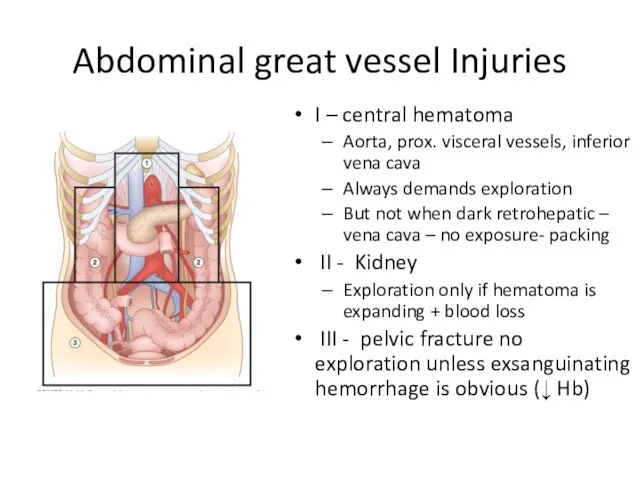
Abdominal great vessel Injuries
I – central hematoma
Aorta, prox. visceral vessels, inferior
Abdominal great vessel Injuries
I – central hematoma
Aorta, prox. visceral vessels, inferior
Genitourinary injuries
The genitourinary organs include the kidneys, ureters, bladder, and urethra,
Genitourinary injuries
The genitourinary organs include the kidneys, ureters, bladder, and urethra,
Intraperitoneal bladder injuries can be repaired in two layers of absorbable
Intraperitoneal bladder injuries can be repaired in two layers of absorbable
Genitourinary Injury
Kidney ureter bladder urethra
Clinic: (gross hematuria), Bleeding ,
Genitourinary Injury
Kidney ureter bladder urethra
Clinic: (gross hematuria), Bleeding ,
Pelvis and extremities injuries
Danger of retroperitoneal hematoma
Low mortality but long-term morbidity
Pelvis and extremities injuries
Danger of retroperitoneal hematoma
Low mortality but long-term morbidity
Injuries to the Pelvis and Extremities
Injuries to the Pelvis and Extremities
In which of the following the pulse pressure is normal? A.
In which of the following the pulse pressure is normal? A.
A 30 - year - old male is brought to the
A 30 - year - old male is brought to the
22 - year - old male is brought to the trauma
22 - year - old male is brought to the trauma
A 36 years old male was involved in a vehicle accident
A 36 years old male was involved in a vehicle accident
21-years old man arrives in the emergency department with a stab
21-years old man arrives in the emergency department with a stab
A 40 years old male is status post-splenectomy following a motor
A 40 years old male is status post-splenectomy following a motor
A 15-years-old girl fall while cycling. in the ER. 8 hours
A 15-years-old girl fall while cycling. in the ER. 8 hours
A 40 year old male is admitted to the ER following
A 40 year old male is admitted to the ER following
 КНИГА ПАМЯТИ 1 класса
КНИГА ПАМЯТИ 1 класса Онлайн-голосование по отбору общественных территорий. Формирование комфортной городской среды
Онлайн-голосование по отбору общественных территорий. Формирование комфортной городской среды Workforce Circa
Workforce Circa лит чт 04 02
лит чт 04 02 Сверление стен
Сверление стен Очистка сточных вод и характеристика очистных сооружений Свердловской области
Очистка сточных вод и характеристика очистных сооружений Свердловской области Вольфрамовые электроды
Вольфрамовые электроды М. И. Карасев Муха-Цокотуха
М. И. Карасев Муха-Цокотуха Дорогая Гузель!
Дорогая Гузель! Промышленность Свердловской области
Промышленность Свердловской области Виды тканей
Виды тканей Постройка и фантазия
Постройка и фантазия Основные сведения о древесине
Основные сведения о древесине Иллюстрация к произведению Чехова
Иллюстрация к произведению Чехова Сепсис новорождённого
Сепсис новорождённого Газобаллонное оборудование 5 поколения
Газобаллонное оборудование 5 поколения Исследование напряженно-деформированного состояния дискретно армированного стеклопластика на основе термопластичной матрицы
Исследование напряженно-деформированного состояния дискретно армированного стеклопластика на основе термопластичной матрицы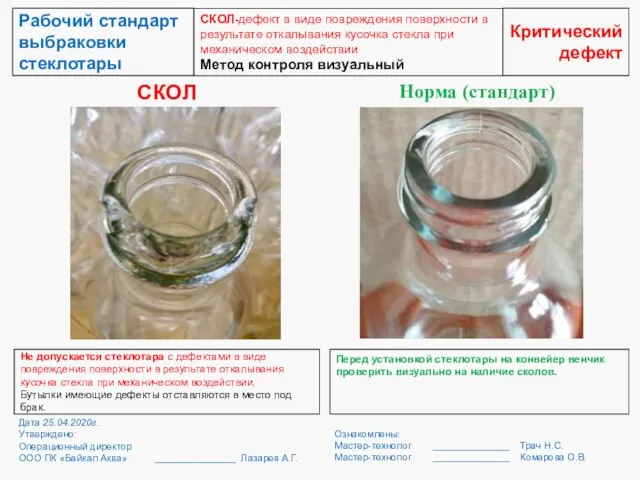 Рабочий стандарт выбраковки стеклотары
Рабочий стандарт выбраковки стеклотары ОС_Презентація_особливої_сесії_EdCamp_in_a_Box_6_0_14_05_21_1
ОС_Презентація_особливої_сесії_EdCamp_in_a_Box_6_0_14_05_21_1 Отчетная документация по педагогической практике
Отчетная документация по педагогической практике Поэты, не вернувшиеся с войны, или До последнего дыхания
Поэты, не вернувшиеся с войны, или До последнего дыхания Электромонтажные и проектные работы. Лаборатория электроизмерений АВС-электро
Электромонтажные и проектные работы. Лаборатория электроизмерений АВС-электро модные часы _ by Artem Morozov
модные часы _ by Artem Morozov Судовое обеспечение подводных работ
Судовое обеспечение подводных работ Основные этапы развития электронной техники
Основные этапы развития электронной техники Современная Российская система образования
Современная Российская система образования О благословении князя Дмитрия Донского на Куликовскую битву
О благословении князя Дмитрия Донского на Куликовскую битву Путешествие в мир сказок
Путешествие в мир сказок