-
Сифилис (возбудитель - бледные трепонемы)

Содержание
- 2. Бледные трепонемы - возбудители сифилиса
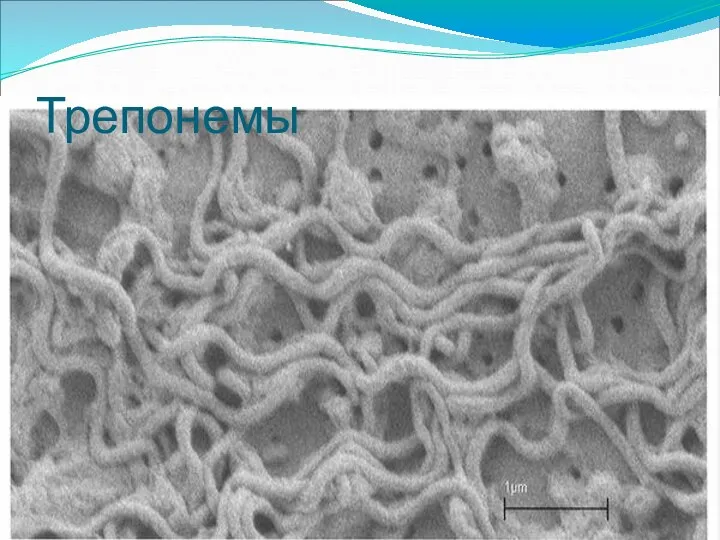
- 3. Трепонемы
- 4. Трепонемы
- 5. http://info.fujita-hu.ac.jp/~tsutsumi/case/case133.htm Бледные трепонемы в межклеточном пространстве
- 6. Возбудитель Сифилиса – Бледная Трепонема Бледная трепонема
- 7. Transmission electron micrograph of Treponema isolated from a bovine digital dermatitis lesion. The fixation treatment has
- 8. Электронный вид трепонем
- 9. Возбудитель Сифилиса – Бледная Трепонема Бледная трепонема
- 10. Dark field photomicrograph of Treponema pallidum bacteria. Nichol's strain of T. pallidum from a rabbit testicle,
- 11. Treponema pallidum, IFA
- 14. Диагностика
- 15. Diagnosis of syphilis The definitive diagnosis of primary syphilis is made by visualization of treponemes by
- 17. Treponema hyodysenteriae (возбудитель дизентерии свиней) http://vetfak.nsau.edu.ru/new/uchebnic/microbiology/stu/index_micro.htm
- 18. Treponema hyodysenteriae (возбудитель дизентерии свиней) http://vetfak.nsau.edu.ru/new/uchebnic/microbiology/stu/index_micro.htm
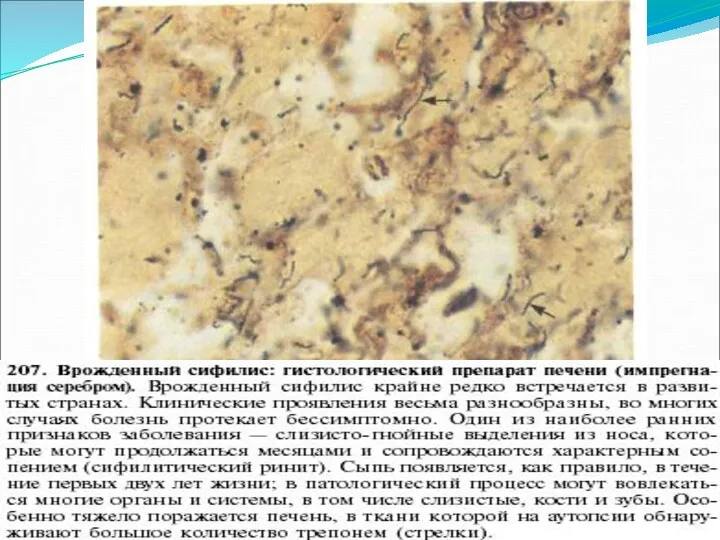
- 20. Врожденный сифилис
- 23. Сифилитическая ангина
- 24. Congenital syphilis, primary and secondary syphilis rates, by year -- United States, 1992-1998. Epidemiology, surveillance.
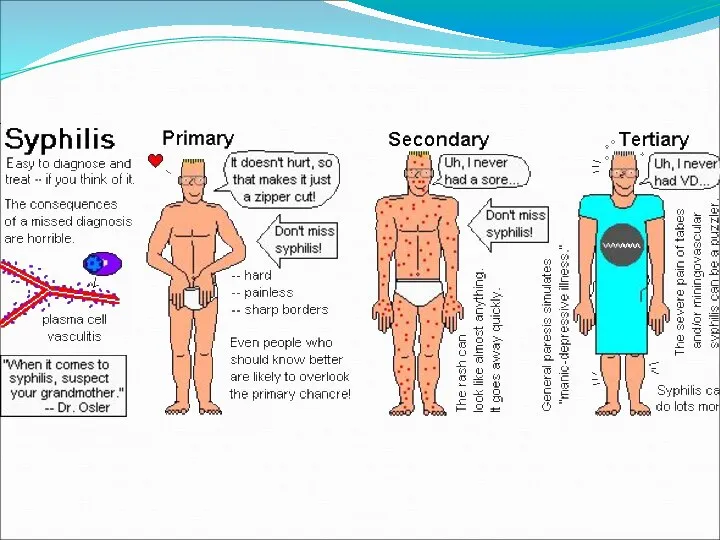
- 25. Clinical presentation of syphilis
- 27. Первичный сифилис
- 31. Primary and secondary syphilis—Age- and sex-specific rates: United States, 2006
- 34. Сифилис
- 36. Сифилитический шанкр
- 37. Вторичный сифилис
- 39. Вторичный сифилис
- 40. Сифилис вторичный
- 44. Сифилис вторичный
- 46. Сифилис вторичный
- 48. Secondary syphilis - mouth mucosa Bristol Biomedical Archive
- 52. Secondary syphilis manifested perineal condyloma lata lesions, which presented as gray, raised papules that sometimes appear
- 53. Сифилис
- 55. Dürer Syphilis 1496
- 57. Лама
- 58. Primary and secondary syphilis — Rates: Total and by sex: United States, 1987–2006
- 60. Gummas, or soft ”gummy” tumors, are seen here on this liver specimen due to tertiary syphilis.
- 61. Гумма
- 62. Yaws is a crippling and disfiguring disease affecting some 50 million people in the world
- 63. A photograph of a patient with tertiary syphilis resulting in gummas seen here on the nose.
- 66. Сифилис. Уродства. Model of the head of a patient with tertiary syphilis
- 67. Primary syphilis After an incubation period of 2 to 6 weeks following exposure, a papule develops
- 68. Reported cases of syphilis by stage of infection: United States, 1941–2006
- 69. Epidemiology of clinically-apparent UTI (upper panel) and asymptomatic bacteriuria (lower panel) according to age and sex.
- 70. Сифилис
- 71. Уровни заболеваемости сифилисом (на 100 тыс. населения)
- 72. Количество случаев врожденного сифилиса по РФ
- 73. Клинические проявления Твердый шанкр
- 74. Вторичный сифилис(папулы)
- 75. Вторичный сифилис (алопеции)
- 76. Ранний врожденный сифилис
- 79. Скачать презентацию

Бледные трепонемы - возбудители сифилиса
Бледные трепонемы - возбудители сифилиса

Трепонемы
Трепонемы
Трепонемы
Трепонемы

http://info.fujita-hu.ac.jp/~tsutsumi/case/case133.htm
Бледные трепонемы
в межклеточном пространстве
http://info.fujita-hu.ac.jp/~tsutsumi/case/case133.htm
Бледные трепонемы
в межклеточном пространстве
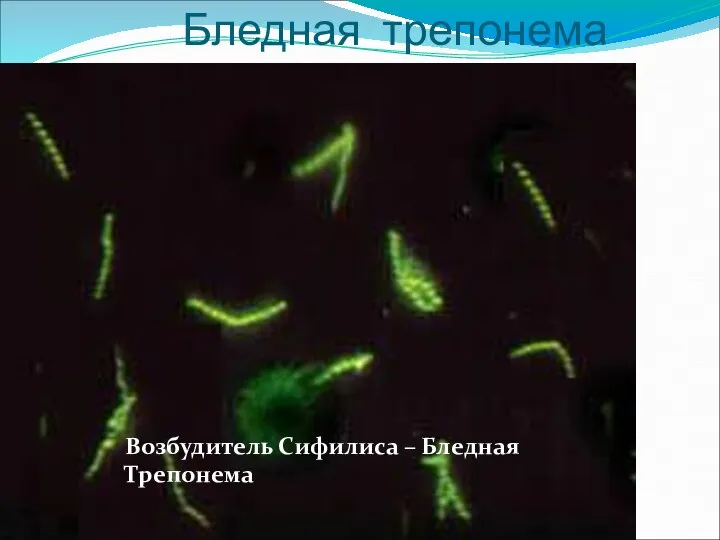
Возбудитель Сифилиса – Бледная Трепонема
Бледная трепонема
Возбудитель Сифилиса – Бледная Трепонема
Бледная трепонема
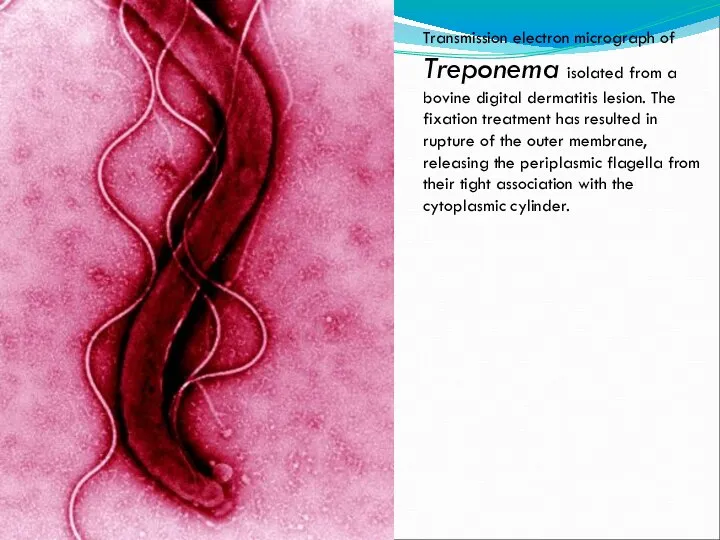
Transmission electron micrograph of Treponema isolated from a bovine digital dermatitis
Transmission electron micrograph of Treponema isolated from a bovine digital dermatitis

Электронный вид трепонем
Электронный вид трепонем

Возбудитель Сифилиса – Бледная Трепонема
Бледная трепонема
Возбудитель Сифилиса – Бледная Трепонема
Бледная трепонема

Dark field photomicrograph of Treponema pallidum bacteria. Nichol's strain of T.
Dark field photomicrograph of Treponema pallidum bacteria. Nichol's strain of T.
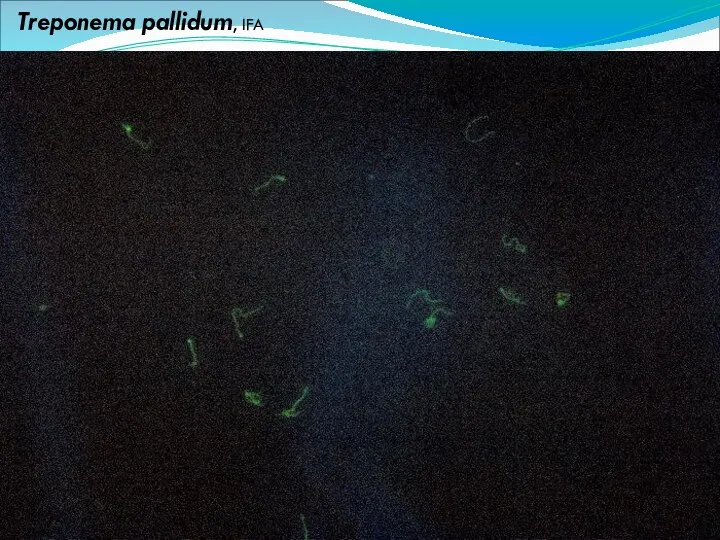
Treponema pallidum, IFA
Treponema pallidum, IFA


Диагностика
Диагностика

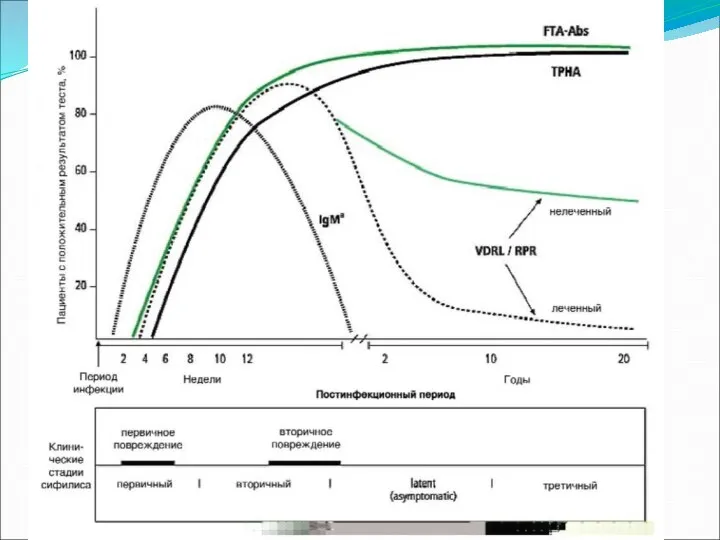
Diagnosis of syphilis
The definitive diagnosis of primary syphilis is made by
Diagnosis of syphilis The definitive diagnosis of primary syphilis is made by
Treponema hyodysenteriae
(возбудитель дизентерии свиней)
http://vetfak.nsau.edu.ru/new/uchebnic/microbiology/stu/index_micro.htm
Treponema hyodysenteriae
(возбудитель дизентерии свиней)
http://vetfak.nsau.edu.ru/new/uchebnic/microbiology/stu/index_micro.htm
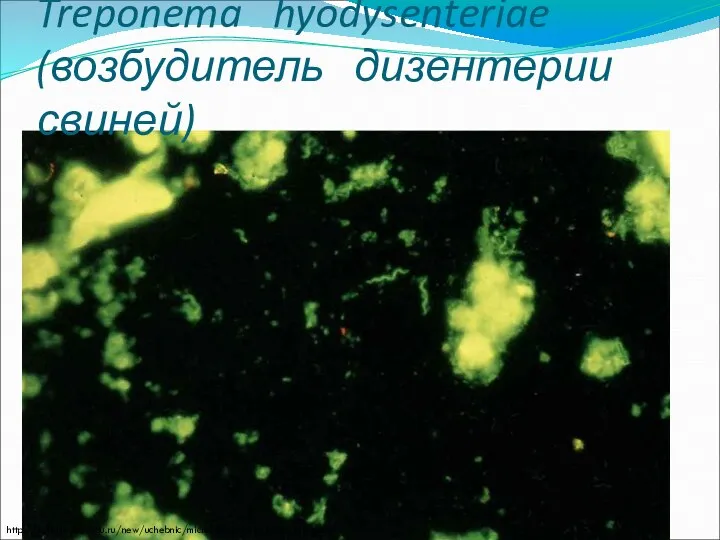
Treponema hyodysenteriae
(возбудитель дизентерии свиней)
http://vetfak.nsau.edu.ru/new/uchebnic/microbiology/stu/index_micro.htm
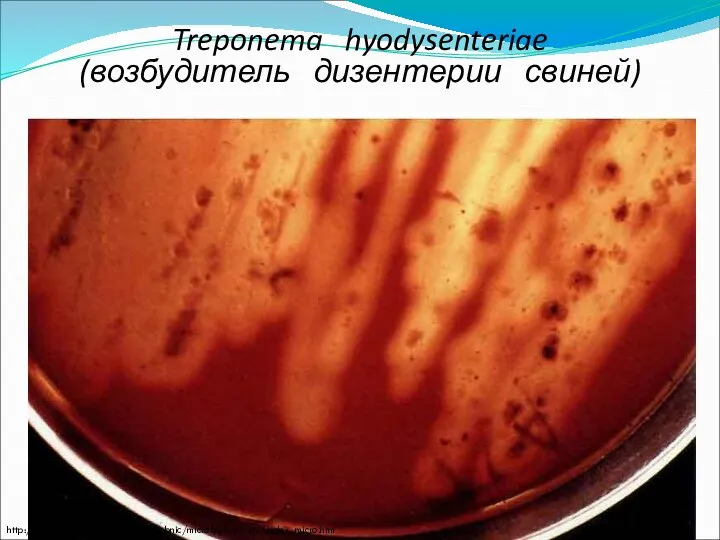
Treponema hyodysenteriae
(возбудитель дизентерии свиней)
http://vetfak.nsau.edu.ru/new/uchebnic/microbiology/stu/index_micro.htm


Врожденный сифилис
Врожденный сифилис


Сифилитическая ангина
Сифилитическая ангина
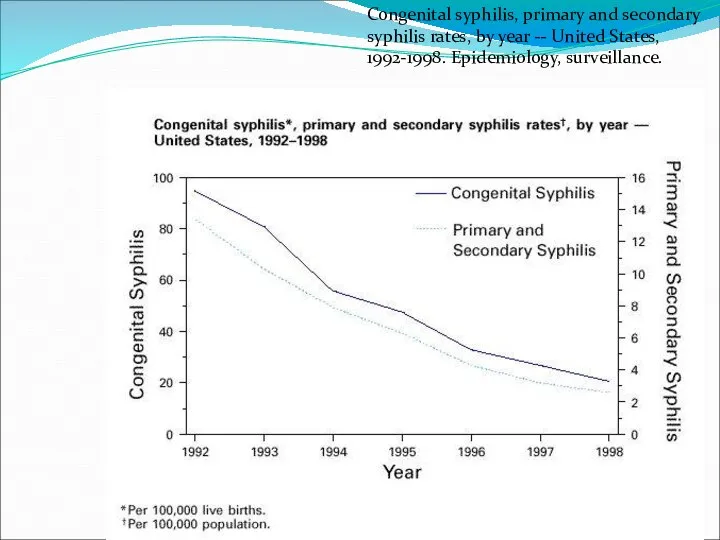
Congenital syphilis, primary and secondary syphilis rates, by year -- United
Congenital syphilis, primary and secondary syphilis rates, by year -- United

Clinical presentation of syphilis
Clinical presentation of syphilis

Первичный сифилис
Первичный сифилис




Primary and secondary syphilis—Age- and sex-specific rates: United States, 2006
Primary and secondary syphilis—Age- and sex-specific rates: United States, 2006



Сифилис
Сифилис


Сифилитический шанкр
Сифилитический шанкр

Вторичный сифилис
Вторичный сифилис


Вторичный сифилис
Вторичный сифилис

Сифилис вторичный
Сифилис вторичный




Сифилис вторичный
Сифилис вторичный


Сифилис вторичный
Сифилис вторичный


Secondary syphilis - mouth mucosa
Bristol Biomedical Archive
Secondary syphilis - mouth mucosa
Bristol Biomedical Archive




Secondary syphilis manifested perineal condyloma lata lesions, which presented as gray,
Secondary syphilis manifested perineal condyloma lata lesions, which presented as gray,

Сифилис
Сифилис


Dürer Syphilis 1496
Dürer Syphilis 1496


Лама
Лама
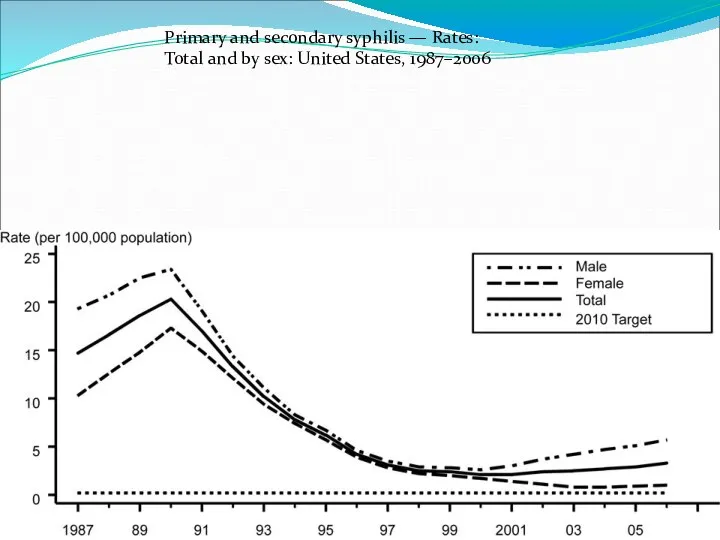
Primary and secondary syphilis — Rates: Total and by sex: United
Primary and secondary syphilis — Rates: Total and by sex: United


Gummas, or soft ”gummy” tumors, are seen here on this liver
Gummas, or soft ”gummy” tumors, are seen here on this liver

Гумма
Гумма

Yaws is a crippling and disfiguring disease affecting some 50 million
Yaws is a crippling and disfiguring disease affecting some 50 million

A photograph of a patient with tertiary syphilis resulting in gummas
A photograph of a patient with tertiary syphilis resulting in gummas

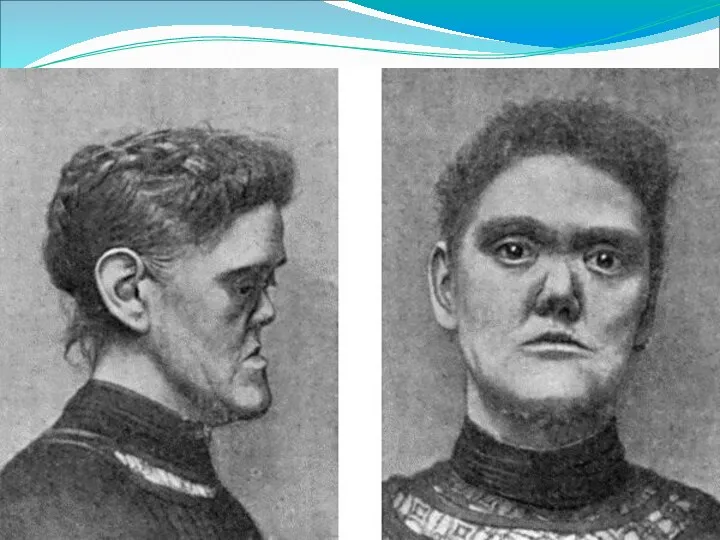

Сифилис. Уродства.
Model of the head of a patient with tertiary
Сифилис. Уродства.
Model of the head of a patient with tertiary

Primary syphilis
After an incubation period of 2 to 6 weeks following
Primary syphilis After an incubation period of 2 to 6 weeks following

Reported cases of syphilis by stage of infection: United States, 1941–2006
Reported cases of syphilis by stage of infection: United States, 1941–2006

Epidemiology of clinically-apparent UTI (upper panel) and asymptomatic bacteriuria (lower panel)
Epidemiology of clinically-apparent UTI (upper panel) and asymptomatic bacteriuria (lower panel)

Сифилис
Сифилис

Уровни заболеваемости сифилисом
(на 100 тыс. населения)
Уровни заболеваемости сифилисом
(на 100 тыс. населения)

Количество случаев
врожденного сифилиса по РФ
Количество случаев
врожденного сифилиса по РФ

Клинические проявления
Твердый шанкр
Клинические проявления
Твердый шанкр

Вторичный сифилис(папулы)
Вторичный сифилис(папулы)
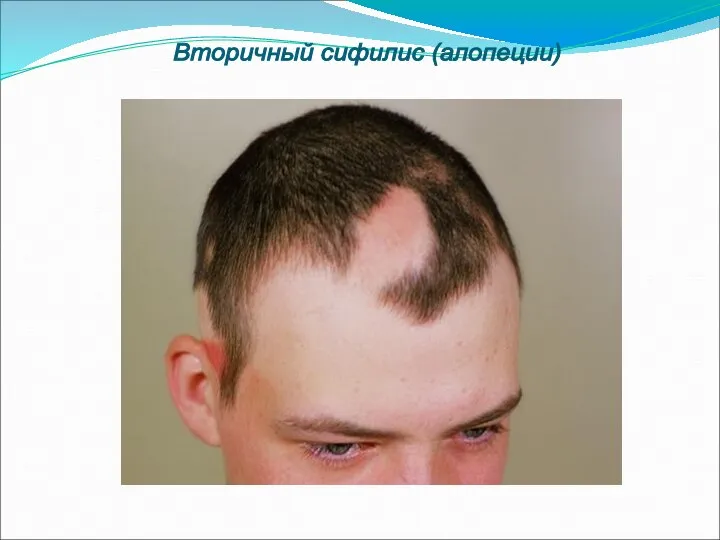
Вторичный сифилис (алопеции)
Вторичный сифилис (алопеции)

Ранний врожденный сифилис
Ранний врожденный сифилис

 Ями на дорогах
Ями на дорогах Циклические алгоритмы. Оператор цикла For.Тело цикла
Циклические алгоритмы. Оператор цикла For.Тело цикла Sonja Gerhardt
Sonja Gerhardt Крест и крестное знамение
Крест и крестное знамение Повторение прошедших тем. Логические выражения
Повторение прошедших тем. Логические выражения Функции элементов нервной системы
Функции элементов нервной системы  Инновационная деятельность в образовании
Инновационная деятельность в образовании  Структура учебно-тренировочного процесса
Структура учебно-тренировочного процесса ГТО – это спорт! Спорт – это жизнь!
ГТО – это спорт! Спорт – это жизнь! коллекция русских икон
коллекция русских икон ТАКТИЧЕСКИЕ ХАРАКТЕРИСТИКИ, ВОЗМОЖНОСТИ И ОСОБЕННОСТИ ЭКСПЛУАТАЦИИ БРОНЕТЕХНИКИ, МОТОЦИКЛОВ, САМОЛЁТОВ И ВЕРТОЛЁТОВ, ИСПОЛЬЗУЕМ
ТАКТИЧЕСКИЕ ХАРАКТЕРИСТИКИ, ВОЗМОЖНОСТИ И ОСОБЕННОСТИ ЭКСПЛУАТАЦИИ БРОНЕТЕХНИКИ, МОТОЦИКЛОВ, САМОЛЁТОВ И ВЕРТОЛЁТОВ, ИСПОЛЬЗУЕМ Синдром жировой эмболии Проф. Н.Е.Буров
Синдром жировой эмболии Проф. Н.Е.Буров Анализ педагогических результатов на основе мониторинга учащихся средней школы ТИНУС ВАЛЕНТИНА МИХАЙЛОВНА учитель физической
Анализ педагогических результатов на основе мониторинга учащихся средней школы ТИНУС ВАЛЕНТИНА МИХАЙЛОВНА учитель физической Азбука архитектуры
Азбука архитектуры Презентация Фотографические принадлежности. Характеристика, классификация, ассортимент
Презентация Фотографические принадлежности. Характеристика, классификация, ассортимент Аналоговые элементы
Аналоговые элементы Noel et Nouvel An en France. Traditions et coutumes
Noel et Nouvel An en France. Traditions et coutumes Единый урок прав человека
Единый урок прав человека Морфофункциональные особенности строения брюшины
Морфофункциональные особенности строения брюшины Земельные, водные и биологические ресурсы России Подготовила Студентка группы Э122б Арсёнова В.
Земельные, водные и биологические ресурсы России Подготовила Студентка группы Э122б Арсёнова В. Реорганизация структурных подразделений ОТ, ТБ и ООС КПО
Реорганизация структурных подразделений ОТ, ТБ и ООС КПО Формы правления. Формы государственно-территориального устройства. Политические режимы
Формы правления. Формы государственно-территориального устройства. Политические режимы Народные промыслы Центрального района России
Народные промыслы Центрального района России К доске
К доске Предмет исторической
Предмет исторической 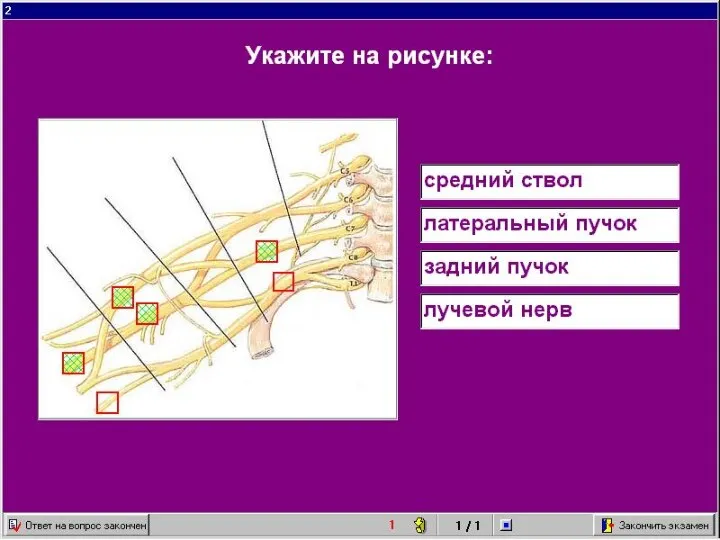 ангиология неврология
ангиология неврология 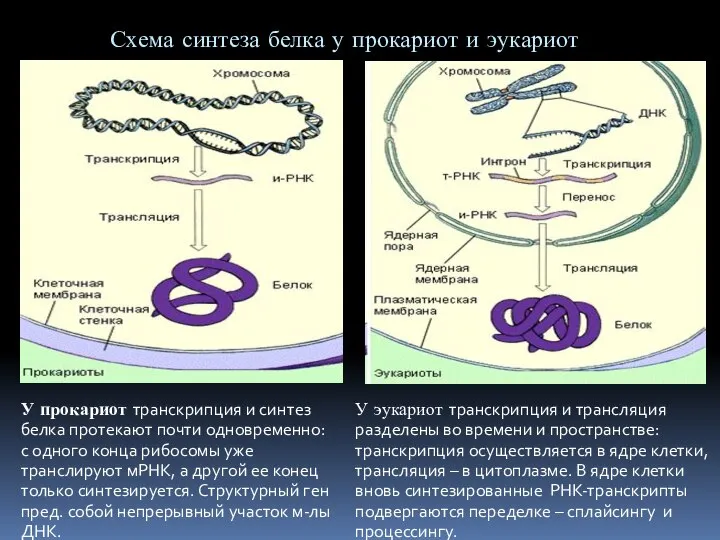 Регуляция синтеза белка
Регуляция синтеза белка Структура команд и режимы адресации на примере PDP-11
Структура команд и режимы адресации на примере PDP-11