- Angina Pectoris

Содержание
- 2. Sudden coronary death Angina pectoris Acute myocardial infarction Painless myocardial ischaemia Heart failure Disturbences of rhythm
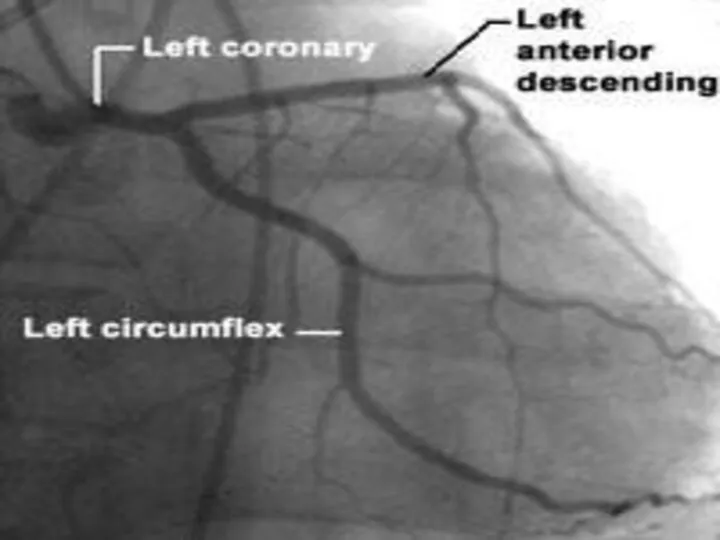
- 3. Ischaemic heart disease . Anterior Heart Arteries The coronary arteries supply blood to the heart muscle.
- 4. Ischaemic heart disease . Posterior Heart Arteries The coronary arteries supply blood to the heart muscle.
- 5. Ischaemic heart disease Ischaemic heart disease (Coronary artery disease) – is the most common form of
- 6. ANGINA PECTORIS-DEFINITION Angina pectoris is the clinical symptom complex caused by transient myocardial ischaemia and may
- 7. ANGINA PECTORIS-DEFINITION Angina pectoris is the medical term used to describe chest pains caused by poor
- 9. RISK FACTORS Nonmodifable : Age (> 45 ) Male gender Family history (genetic predisposition) Aethnic origin
- 11. AETIOLOGY There are 2 primary causes of angina. Coronary (heart) artery atherosclerosis In as many as
- 13. INCIDENCE The incidence of angina continuously rises with age in women while in men the incidence
- 14. Identifying ischaemic cardiac chest pain Ischaemic cardiac chest pain: Location - central, diffuse Radiation -Jaw/neck/shoulder/ arm/back
- 15. SIGNS N SYMPTOMS These are signs and symptoms of angina as well: An uncomfortable pressure, fullness,
- 20. CLASSIFICATION Types of Angina Pectoris Stable Angina Unstable Angina Prinzmetal’s or variant angina Microvascular angina
- 21. Stable Angina Stable angina is a repeating pattern of chest pain which has not changed in
- 22. Сanadian Cardiovascular Society Functional classification of Angina ССS separates patients with angina pectoris into groups based
- 23. Сanadian Cardiovascular Society Functional classification of Angina 3 class – marked limitation of ordinary activity. Angina
- 25. Unstable Angina Unstable angina is chest pain that is variable, either increasing in frequency or intensity
- 26. Unstable angina New onset angina pectoris – from first clinical signs of substernal anginal pain or
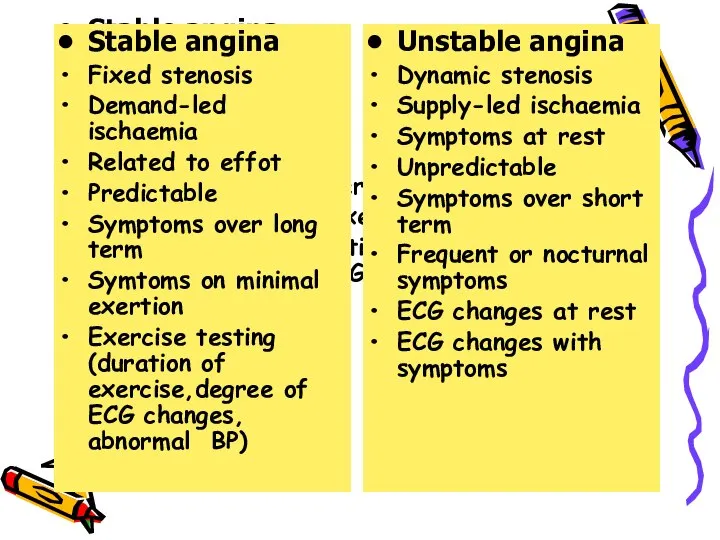
- 27. Stable angina Fixed stenosis Demand-led ischaemia Related to effot Predictable Symptoms over long term Symtoms on
- 28. Prinzmetal's Angina Prinzmetal’s or spontaneous or angiospastic angina is caused by a vasospasm, a spasm that
- 29. Microvascular Angina or Stable Angina Pectoris on angiographycally intact vessels or Coronary Syndrome X Microvascular angina,
- 30. Coronary Syndrome X Characterized by 3 specific, typical signs as : Classic anginal chest pain ST
- 31. Terminology Clarification One major association between microvascular angina and the insulin resistance syndrome has arisen from
- 32. Diabetes and Angina Insulin resistance and secondary hyperinsulinemia are recognized risk factors for development of atherosclerosis.
- 33. Diagnosis The diagnosis of angina pectoris usually involves a careful assessment and history of signs and
- 34. Laboratory investigations Obligatory indicators: Hb, Total Cholesterol, HDL-C, LDL-C, triglycerides, glucose, AST, ALT, creatinine (GFR) Additional
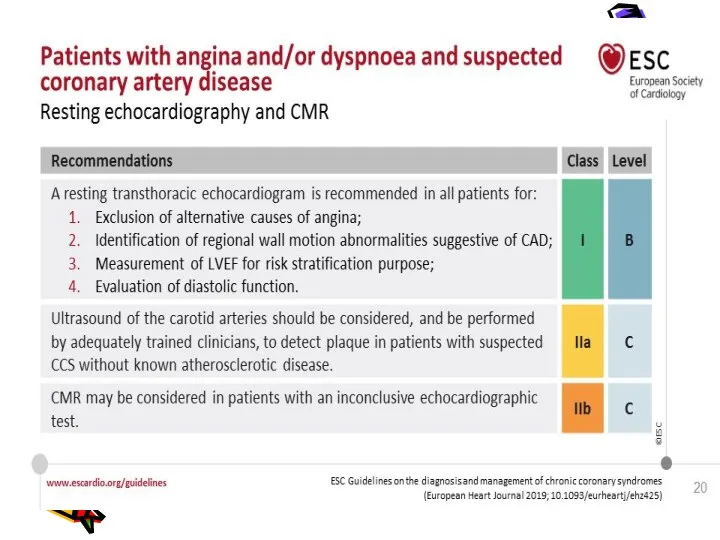
- 35. Investigations Resting ECG – reversible ST depression or elevation with or without T-wave inversion at the
- 36. Investigations Stress echocardiography – to identify ischaemic segments of myocardium and areas of infarction ( exhibit
- 41. Management The management of angina pectoris involves : A careful assessment of the likely extent and
- 46. Treatment Nitroglycerin is the drug most often used. It mainly relaxes the veins and relaxes the
- 47. Anti-anginals - B- blockers -1st line (metoprolol,bisoprolol,nebivolol,carvedilol) - Calcium antagonists (verapamil , amlodipin,diltiazem if b-blockers contraindicated)
- 48. Treatment ANTI-ANGINAL DRUG TREATMENT – GROUPS OF DRUGS ARE USED TO HELP RELIEVE OR PREVENT THE
- 49. Drugs,which improve prognosis - Antiplatelet drugs (aspirin,clopidogrel ) - Statins (lovastatin,simvastatin, atorva-statin,rosuvastatin ) - B-blockers (atenolol,metaprolol,bisoprolol,nebivolol,
- 50. Treatment Controlling the risk factors for angina pectoris, such as high blood pressure, cigarette smoking, high
- 51. What procedures are used to treat angina? Invasive techniques that improve the heart and the heart's
- 52. Coronary artery bypass graft surgery is also used. In it, a blood vessel is used to
- 53. How is variant angina or Prinzmetal's angina treated? Calcium antagonists are extremely effective in preventing the
- 54. Medical Treatment If you have come to the hospital emergency department, you may be sent to
- 55. Medical Treatment Regardless of where you are sent, several basic treatments may be started. Which are
- 56. Medical Treatment Treatment will depend on the severity of symptoms, severity of the underlying disease, and
- 57. Medical Treatment You may be given medication to lower blood pressure or heart rate. Beta blockers,
- 58. Metabolic therapy - Trimetazidine (preductal) - Riboxin - Mildronate (vasonate) - Tiotriozaline - Vitamins - Antioxidantes
- 59. Medical Treatment After reviewing your immediate test results, the hospital health care provider will make a
- 60. Medical Treatment If you keep having symptoms or your condition is unstable, you will be admitted
- 61. INVASIVE TREATMENT Angioplasty is a treatment used for people whose angina does not get better with
- 62. INVASIVE TREATMENT The catheter is threaded through the arteries and into the artery where the narrowing
- 63. Percutaneous transluminal angioplasty (1, 2)
- 64. Percutaneous transluminal angioplasty (3, 4)
- 72. Скачать презентацию
Sudden coronary death
Angina pectoris
Acute myocardial infarction
Painless myocardial ischaemia
Heart failure
Disturbences of
Sudden coronary death
Angina pectoris
Acute myocardial infarction
Painless myocardial ischaemia
Heart failure
Disturbences of

Ischaemic heart disease .
Anterior Heart Arteries
The coronary arteries supply blood to
Ischaemic heart disease .
Anterior Heart Arteries
The coronary arteries supply blood to

Ischaemic heart disease .
Posterior Heart Arteries
The coronary arteries supply blood to
Ischaemic heart disease .
Posterior Heart Arteries
The coronary arteries supply blood to

Ischaemic heart disease
Ischaemic heart disease (Coronary artery disease) – is the
Ischaemic heart disease
Ischaemic heart disease (Coronary artery disease) – is the
ANGINA PECTORIS-DEFINITION
Angina pectoris is the clinical symptom complex caused by
ANGINA PECTORIS-DEFINITION
Angina pectoris is the clinical symptom complex caused by
ANGINA PECTORIS-DEFINITION
Angina pectoris is the medical term used to describe chest
ANGINA PECTORIS-DEFINITION
Angina pectoris is the medical term used to describe chest

RISK FACTORS
Nonmodifable :
Age (> 45 )
Male gender
Family history (genetic predisposition)
Aethnic origin
RISK FACTORS
Nonmodifable :
Age (> 45 )
Male gender
Family history (genetic predisposition)
Aethnic origin

AETIOLOGY
There are 2 primary causes of angina.
Coronary (heart)
AETIOLOGY
There are 2 primary causes of angina.
Coronary (heart)


INCIDENCE
The incidence of angina continuously rises with age in women
INCIDENCE
The incidence of angina continuously rises with age in women
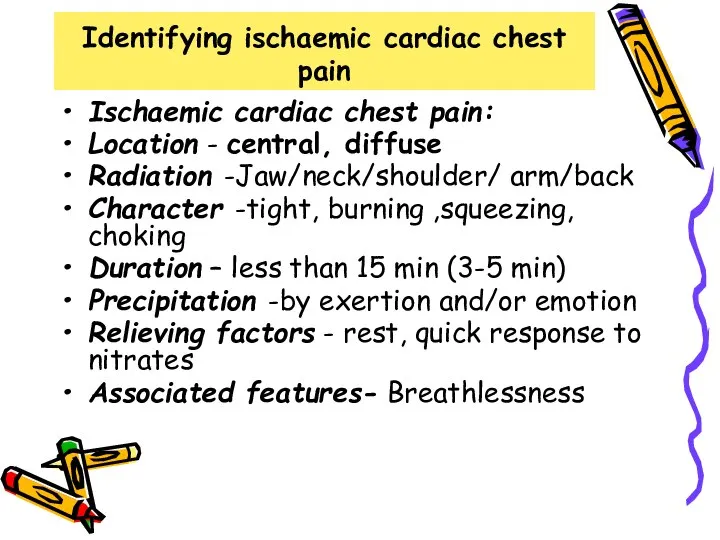
Identifying ischaemic cardiac chest pain
Ischaemic cardiac chest pain:
Location - central, diffuse
Radiation
Identifying ischaemic cardiac chest pain
Ischaemic cardiac chest pain:
Location - central, diffuse
Radiation

SIGNS N SYMPTOMS
These are signs and symptoms of angina as
SIGNS N SYMPTOMS
These are signs and symptoms of angina as





CLASSIFICATION
Types of Angina Pectoris
Stable Angina
Unstable Angina
Prinzmetal’s or variant angina
Types of Angina Pectoris
Stable Angina
Unstable Angina
Prinzmetal’s or variant angina
Stable Angina
Stable angina is a repeating pattern of chest
Stable Angina
Stable angina is a repeating pattern of chest
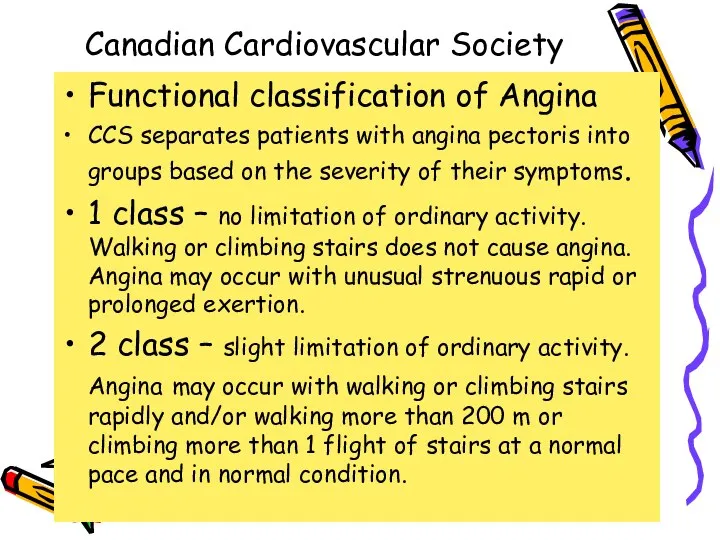
Сanadian Cardiovascular Society
Functional classification of Angina
ССS separates patients with angina pectoris
Сanadian Cardiovascular Society
Functional classification of Angina
ССS separates patients with angina pectoris
Сanadian Cardiovascular Society
Functional classification of Angina
3 class – marked limitation
Сanadian Cardiovascular Society
Functional classification of Angina
3 class – marked limitation

Unstable Angina
Unstable angina is chest pain that is variable,
Unstable Angina
Unstable angina is chest pain that is variable,

Unstable angina
New onset angina pectoris – from first clinical signs
Unstable angina
New onset angina pectoris – from first clinical signs
Stable angina
Fixed stenosis
Demand-led ischaemia
Related to effot
Predictable
Symptoms over long term
Symtoms on minimal
Stable angina
Fixed stenosis
Demand-led ischaemia
Related to effot
Predictable
Symptoms over long term
Symtoms on minimal
Prinzmetal's Angina
Prinzmetal’s or spontaneous or angiospastic angina is caused
Prinzmetal's Angina
Prinzmetal’s or spontaneous or angiospastic angina is caused

Microvascular Angina or Stable Angina Pectoris on angiographycally intact vessels
Microvascular Angina or Stable Angina Pectoris on angiographycally intact vessels

Coronary Syndrome X
Characterized by 3 specific, typical signs as :
Classic anginal
Coronary Syndrome X
Characterized by 3 specific, typical signs as :
Classic anginal
Terminology Clarification
One major association between microvascular angina and the insulin
Terminology Clarification
One major association between microvascular angina and the insulin
Diabetes and Angina
Insulin resistance and secondary hyperinsulinemia are recognized risk
Diabetes and Angina
Insulin resistance and secondary hyperinsulinemia are recognized risk
Diagnosis
The diagnosis of angina pectoris usually involves a careful assessment
Diagnosis
The diagnosis of angina pectoris usually involves a careful assessment
Laboratory investigations
Obligatory indicators:
Hb, Total Cholesterol, HDL-C, LDL-C, triglycerides, glucose, AST,
Laboratory investigations
Obligatory indicators: Hb, Total Cholesterol, HDL-C, LDL-C, triglycerides, glucose, AST,

Investigations
Resting ECG – reversible ST depression or elevation with or without
Investigations
Resting ECG – reversible ST depression or elevation with or without

Investigations
Stress echocardiography – to identify ischaemic segments of myocardium and areas
Investigations
Stress echocardiography – to identify ischaemic segments of myocardium and areas


Management
The management of angina pectoris involves :
A careful assessment of the
Management
The management of angina pectoris involves :
A careful assessment of the




Treatment
Nitroglycerin is the drug most often used. It mainly relaxes the
Treatment
Nitroglycerin is the drug most often used. It mainly relaxes the
Anti-anginals
- B- blockers -1st line (metoprolol,bisoprolol,nebivolol,carvedilol)
- Calcium antagonists (verapamil , amlodipin,diltiazem
Anti-anginals
- B- blockers -1st line (metoprolol,bisoprolol,nebivolol,carvedilol)
- Calcium antagonists (verapamil , amlodipin,diltiazem
Treatment
ANTI-ANGINAL DRUG TREATMENT – GROUPS OF DRUGS ARE USED TO HELP
Treatment
ANTI-ANGINAL DRUG TREATMENT – GROUPS OF DRUGS ARE USED TO HELP

Drugs,which improve prognosis
- Antiplatelet drugs (aspirin,clopidogrel )
- Statins (lovastatin,simvastatin, atorva-statin,rosuvastatin )
-
Drugs,which improve prognosis
- Antiplatelet drugs (aspirin,clopidogrel )
- Statins (lovastatin,simvastatin, atorva-statin,rosuvastatin )
-
Treatment
Controlling the risk factors for angina pectoris, such as high
Treatment Controlling the risk factors for angina pectoris, such as high
What procedures are used to treat angina?
Invasive techniques that improve the
What procedures are used to treat angina?
Invasive techniques that improve the
Coronary artery bypass graft surgery is also used. In it, a
Coronary artery bypass graft surgery is also used. In it, a
How is variant angina or Prinzmetal's angina treated?
Calcium antagonists are extremely
How is variant angina or Prinzmetal's angina treated?
Calcium antagonists are extremely

Medical Treatment
If you have come to the hospital emergency department, you
Medical Treatment
If you have come to the hospital emergency department, you

Medical Treatment
Regardless of where you are sent, several basic treatments may
Medical Treatment
Regardless of where you are sent, several basic treatments may
Medical Treatment Treatment will depend on the severity of symptoms,
Medical Treatment Treatment will depend on the severity of symptoms,

Medical Treatment
You may be given medication to lower blood pressure or
Medical Treatment
You may be given medication to lower blood pressure or

Metabolic therapy
- Trimetazidine (preductal)
- Riboxin
- Mildronate (vasonate)
- Tiotriozaline
- Vitamins
- Antioxidantes
Metabolic therapy
- Trimetazidine (preductal)
- Riboxin
- Mildronate (vasonate)
- Tiotriozaline
- Vitamins
- Antioxidantes

Medical Treatment After reviewing your immediate test results, the hospital
Medical Treatment After reviewing your immediate test results, the hospital
Medical Treatment
If you keep having symptoms or your condition is unstable,
Medical Treatment
If you keep having symptoms or your condition is unstable,

INVASIVE TREATMENT Angioplasty is a treatment used for people whose
INVASIVE TREATMENT Angioplasty is a treatment used for people whose
INVASIVE TREATMENT
The catheter is threaded through the arteries and into the
INVASIVE TREATMENT
The catheter is threaded through the arteries and into the

Percutaneous transluminal angioplasty (1, 2)
Percutaneous transluminal angioplasty (1, 2)

Percutaneous transluminal angioplasty (3, 4)
Percutaneous transluminal angioplasty (3, 4)





 Физиология послеродового периода
Физиология послеродового периода Профилактика курения
Профилактика курения Профилактика употребления ПАВ в подростковой среде
Профилактика употребления ПАВ в подростковой среде Аноректальные пороки развития у детей
Аноректальные пороки развития у детей Инфекция. Бактериялар мен вирустардың патогендігі және вируленттігі
Инфекция. Бактериялар мен вирустардың патогендігі және вируленттігі Сымбат пиелонефрит
Сымбат пиелонефрит Аптека под ногами
Аптека под ногами Родительские послания: 10 фраз, которые определяют жизнь человека
Родительские послания: 10 фраз, которые определяют жизнь человека ЛФК при переломах
ЛФК при переломах Этиология и патогенез лихорадки
Этиология и патогенез лихорадки Общая патология, как отрасль медицины
Общая патология, как отрасль медицины Лимфатическая система. Кровь. Тема 21. ч1
Лимфатическая система. Кровь. Тема 21. ч1 Болезни желудочно-кишечного тракта
Болезни желудочно-кишечного тракта Скелет головы
Скелет головы Пероральные сахароснижающие ЛС
Пероральные сахароснижающие ЛС Измерение артериального давления
Измерение артериального давления Дифференциальная диагностика при гепатомегалии
Дифференциальная диагностика при гепатомегалии Взаимосвязь толерантности и агрессивности
Взаимосвязь толерантности и агрессивности Клінічні прояви психічних захворювань і їх судово-психіатрична оцінка. Тема 3
Клінічні прояви психічних захворювань і їх судово-психіатрична оцінка. Тема 3 Авторская психотерапевтическая программа «дизайн человека совершенного»
Авторская психотерапевтическая программа «дизайн человека совершенного» Препараты гормонов и их синтетические аналоги
Препараты гормонов и их синтетические аналоги Терапия. Задача. Диагноз: ХОБЛ, GOLD II, mMRC-2, степень риска В, вне обострения
Терапия. Задача. Диагноз: ХОБЛ, GOLD II, mMRC-2, степень риска В, вне обострения Психологическая уравновешенность. Стресс и его влияние на человека
Психологическая уравновешенность. Стресс и его влияние на человека Оттискные материалы
Оттискные материалы Хронічна серцева недостатність. Визначення. Класифікація. Клініка. Діаганостика. Лікування
Хронічна серцева недостатність. Визначення. Класифікація. Клініка. Діаганостика. Лікування Функциональная биохимия нервной ткани
Функциональная биохимия нервной ткани ВИЧ-инфекция. Термины, открытие, устойчивость вируса
ВИЧ-инфекция. Термины, открытие, устойчивость вируса Рациональное вскармливание детей первого года жизни
Рациональное вскармливание детей первого года жизни