- Mixed medicine case

Содержание
- 2. Case 1 Your next patient in general practice is a 45 year old Mr. Snider who
- 3. history I’m sorry that your brother passed away recently. I know that it is hard. Assess
- 4. History Diet: what kind of food you eat What is your level of exercise? SAD and
- 5. Physical examination General Appearance - Acromegaly- bossing of forehead, Cyanosis Vitals – Normal BMI – normal
- 6. Investigations FBE, U&E, BSL lipid profile, serum uric acid, TFTs, ECG Stress test
- 7. CVS chart
- 8. Without DM
- 9. Management All the investigations are normal. I could not find any abnormality in physical examination.. But
- 10. Management Alcohol – up to 2 standard drinks for 5 days a week Physical activity –
- 11. Case 2 A 63 year old car sales man, John, presents to the emergency department with
- 12. History John was woken up from an afternoon nap by sudden onset of severe, tearing pain
- 13. History Of Presenting Complaint- SOCRATES Site: where exactly do you have the pain? Onset: how did
- 14. Previous Episodes Is this the first episode or have you had similar episodes before? If previous
- 15. physical examination BP 155/100, no BP difference between right and left arm, P 78, RR 18,
- 16. Causes risk factors Bicuspid aortic disease Marfan syndrome and Ehlers-Danlos syndrome Other connective tissue disorders (Marfanoid)
- 17. Thoracic aortic dissection Aortic dissection is the tearing of the inner layer of the aortic wall,
- 19. Management Supportive: A B C Oxygen Analgesia Monitoring Arterial/CVP lines Medical Management: BP reduction to 100
- 20. CT scan of Type A
- 21. Case 3 You have a middle-aged clerical male coming to your GP practice with a 1-day
- 22. Differentials PSGN IgA Nephropathy Bladder cancer Renal cell cancer PCKD
- 23. History How bad is it? When did it start? What is the kind of pain? Is
- 24. History Have you noticed bleeding from anywhere else such as bruising or nosebleed? Any problem with
- 25. Explanation From the history most likely you have a condition called IgA nephropathy. Do you know
- 26. Mechanism
- 27. Difference Between Nephrotic and Nephritic Syndrome
- 30. Prognosis Is it risky? The prognosis is usually good especially in those who have normal BP
- 31. Case 4 76 year old Mr. Aaron Samuels, who is your patient for last 7 years
- 32. AAA
- 33. Guideline
- 34. 5 A’s approach Hello Aaron, How have been from last week? Hmm, you are excited about
- 35. Risk factors Can be completely asymptomatic, but occasionally can give back or tummy pain. Familial Smoking
- 36. The better news in your case is, it is It is still serious and we need
- 37. >5cm – Is it dangerous Doctor? Can I travel? When it is more than 5cm, you
- 38. Case 5 You are a HMO in the psychiatric department of the major hospital. You have
- 39. History CONFIDENTIALITY HOPC Psychiatry H/O - PTSD, depression, suicidal ideas HEADSS – alcohol, drug use is
- 40. Acute Stress Disorder is the term used when symptoms develop within the first month after a
- 41. Management DO YOU WANT TO REPORT THIS TO THE POLICE, so that the person who assaulted
- 42. Case 6 GP, 24 years old woman who is pregnant come to see you complain of
- 43. History Any injury, any infection, any pain any exposure to very loud noise Did you need
- 44. Physical examination Inspection -External ear - pulling ear -pain? -Press mastoid bone - tenderness ( cholesteatoma)
- 45. Examination Special test -Tunning fork ( 256 Hz) -Rinnie -mastoid and ear which one better? -Weber
- 47. weber’s test
- 48. causes of Sensorineural deafness -Cochlear degeneration -Acoustic neuroma -Drug -Ototoxicity - Streptomycin -Fracture of petrous temporal
- 49. Otoscelerosis Otosclerosis Common causes of hearing loss in adult -stapes bone stick to oval window, Normally
- 50. Management hearing contain 2 parts - air conduction and nerve conduction. your cases is air conduction
- 51. Case 7 A young woman at 10 weeks’ gestational age comes to see you in your
- 52. History GM, I am Dr. XYZ… how are you today? I understand that you are here
- 53. History Reassure her that she will be monitored. Antenatal screening should be discussed with all pregnant
- 54. First trimester screening test Combined Test- ■ A non-fasting blood test which is done at 9-13
- 55. risk factor Information from the ultrasound scan is reported to the pathology laboratory to allow the
- 56. 2nd trimester screening test 15 -17 weeks-solely blood tests. – Triple test (a, b, e) (detection
- 57. In high-risk pregnancies, diagnostic tests: ■ CVS – Done ideally at 11-14 weeks. – A needle
- 58. patient questions Are the tests painful? Many women find the diagnostic tests uncomfortable, and they are
- 59. Case 8 In a GP setting. An 17 year-old boy complaining of pain in the tummy
- 60. Differential Duodenal injury Local abdominal hematoma Gall bladder injury Testicular torison UTI Gall stone Strangulated inguinal
- 61. History Vital stability of the child – B.P. -100/60, P.R- 120, RR- 35 & O2 –
- 62. History BINDS – Heel prick test was done ?( thyroid) Any concern about development? Family situation
- 63. Physical examination General appearance – distress & in pain , no signs of dehydration VS: -
- 64. Explanation Your son has a Duodenal injury in the tummy as I could see bruise patch
- 65. Case: 10 26 year old John has been brought by the police from a local pub
- 66. Assess patient’s injury, offer pain management CONFIDENTIALITY History Can you tell me what happened at the
- 67. At hospital -> ever seen by a psychiatrist. Yes. I think there is nothing wrong with
- 68. Psychosocial H/O Home : Left home at 16 years. No contact with parents or siblings. Employment
- 69. Management Difficulty to treat because of late presentation and lack of insight In this patient, get
- 70. ANTISOCIAL PERSONALITY DISORDER (DSM V)
- 71. a mental disorder where a person shows no regard for right or wrong and is not
- 72. Symptoms Deceitfulness Non Conformity no respect for the law and have no boundaries. Impulsivity Aggression Irresponsibility
- 73. Reference https://wayahead.org.au/mental-health-information/fact-sheets/ mental-illness-and-related/antisocial-personality-disorder/
- 75. Скачать презентацию

Case 1
Your next patient in general practice is a 45 year
Case 1
Your next patient in general practice is a 45 year

history
I’m sorry that your brother passed away recently. I know that
history
I’m sorry that your brother passed away recently. I know that

History
Diet: what kind of food you eat
What is your level of
History
Diet: what kind of food you eat
What is your level of
Physical examination
General Appearance - Acromegaly- bossing of forehead, Cyanosis
Vitals – Normal
BMI
Physical examination
General Appearance - Acromegaly- bossing of forehead, Cyanosis
Vitals – Normal
BMI

Investigations
FBE, U&E,
BSL lipid profile,
serum uric acid,
TFTs,
ECG Stress
Investigations
FBE, U&E,
BSL lipid profile,
serum uric acid,
TFTs,
ECG Stress
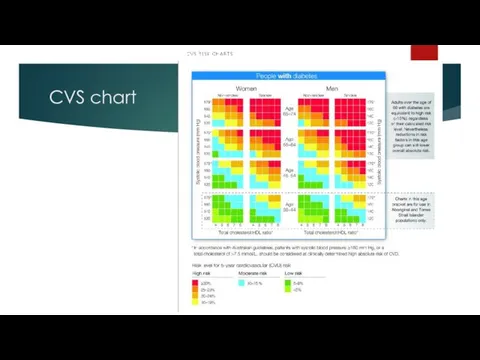
CVS chart
CVS chart
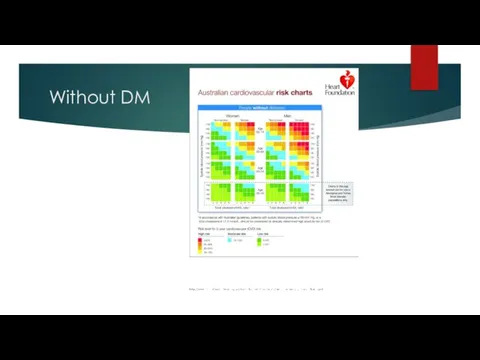
Without DM
Without DM

Management
All the investigations are normal. I could not find any abnormality
Management
All the investigations are normal. I could not find any abnormality

Management
Alcohol – up to 2 standard drinks for 5 days a
Management
Alcohol – up to 2 standard drinks for 5 days a

Case 2
A 63 year old car sales man, John, presents to
Case 2
A 63 year old car sales man, John, presents to

History
John was woken up from an afternoon nap by sudden onset
History
John was woken up from an afternoon nap by sudden onset
History Of Presenting Complaint- SOCRATES
Site: where exactly do you have the
History Of Presenting Complaint- SOCRATES
Site: where exactly do you have the

Previous Episodes
Is this the first episode or have you had similar
Previous Episodes
Is this the first episode or have you had similar
physical examination
BP 155/100, no BP difference between right and left arm,
physical examination
BP 155/100, no BP difference between right and left arm,
Causes risk factors
Bicuspid aortic disease
Marfan syndrome and Ehlers-Danlos syndrome
Other
Causes risk factors
Bicuspid aortic disease
Marfan syndrome and Ehlers-Danlos syndrome
Other

Thoracic aortic dissection
Aortic dissection is the tearing of the inner layer
Thoracic aortic dissection
Aortic dissection is the tearing of the inner layer


Management
Supportive: A
B
C
Oxygen Analgesia Monitoring
Arterial/CVP lines
Medical Management:
BP reduction
Management
Supportive: A
B
C
Oxygen Analgesia Monitoring
Arterial/CVP lines
Medical Management:
BP reduction
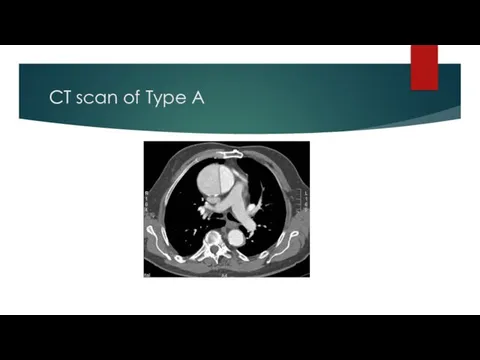
CT scan of Type A
CT scan of Type A

Case 3
You have a middle-aged clerical male coming to your GP
Case 3
You have a middle-aged clerical male coming to your GP

Differentials
PSGN
IgA Nephropathy
Bladder cancer
Renal cell cancer
PCKD
Differentials
PSGN
IgA Nephropathy
Bladder cancer
Renal cell cancer
PCKD
History
How bad is it? When did it start? What is the
History
How bad is it? When did it start? What is the

History
Have you noticed bleeding from anywhere else such as bruising or
History
Have you noticed bleeding from anywhere else such as bruising or

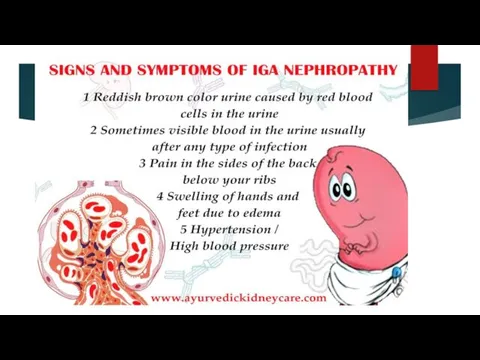
Explanation
From the history most likely you have a condition called IgA
Explanation
From the history most likely you have a condition called IgA
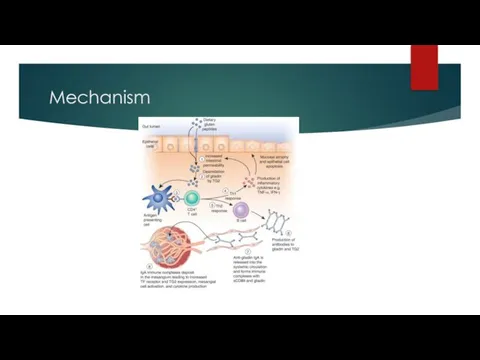
Mechanism
Mechanism
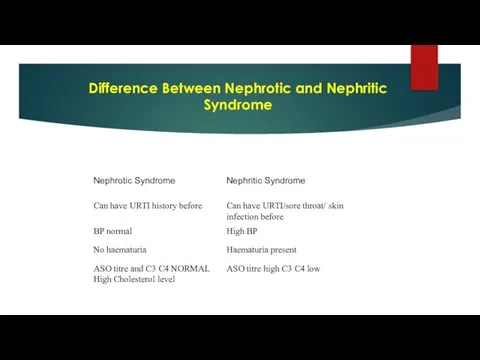
Difference Between Nephrotic and Nephritic Syndrome
Difference Between Nephrotic and Nephritic Syndrome

Prognosis
Is it risky? The prognosis is usually good especially in those
Prognosis
Is it risky? The prognosis is usually good especially in those

Case 4
76 year old Mr. Aaron Samuels, who is your patient
Case 4
76 year old Mr. Aaron Samuels, who is your patient

AAA
AAA

Guideline
Guideline

5 A’s approach
Hello Aaron, How have been from last week?
Hmm,
5 A’s approach
Hello Aaron, How have been from last week?
Hmm,
Risk factors
Can be completely asymptomatic, but occasionally can give back
Risk factors
Can be completely asymptomatic, but occasionally can give back
<5cm – Is it serious ? Can I go for trip
<5cm – Is it serious ? Can I go for trip
>5cm – Is it dangerous Doctor? Can I travel?
When it is
>5cm – Is it dangerous Doctor? Can I travel?
When it is
Case 5
You are a HMO in the psychiatric department of the
Case 5
You are a HMO in the psychiatric department of the

History
CONFIDENTIALITY
HOPC
Psychiatry H/O - PTSD, depression, suicidal ideas
HEADSS – alcohol, drug
History
CONFIDENTIALITY
HOPC
Psychiatry H/O - PTSD, depression, suicidal ideas
HEADSS – alcohol, drug

Acute Stress Disorder is the term used when symptoms develop within
Acute Stress Disorder is the term used when symptoms develop within

Management
DO YOU WANT TO REPORT THIS TO THE POLICE, so
Management
DO YOU WANT TO REPORT THIS TO THE POLICE, so

Case 6
GP, 24 years old woman who is pregnant come to
Case 6
GP, 24 years old woman who is pregnant come to

History
Any injury, any infection, any pain
any exposure to very loud noise
Did
History
Any injury, any infection, any pain
any exposure to very loud noise
Did
Physical examination
Inspection -External ear - pulling ear -pain?
-Press mastoid bone
Physical examination
Inspection -External ear - pulling ear -pain?
-Press mastoid bone

Examination
Special test
-Tunning fork ( 256 Hz)
-Rinnie -mastoid and ear which
Examination
Special test
-Tunning fork ( 256 Hz)
-Rinnie -mastoid and ear which


weber’s test
weber’s test
causes of Sensorineural deafness
-Cochlear degeneration
-Acoustic neuroma
-Drug -Ototoxicity - Streptomycin
-Fracture of
causes of Sensorineural deafness
-Cochlear degeneration
-Acoustic neuroma
-Drug -Ototoxicity - Streptomycin
-Fracture of
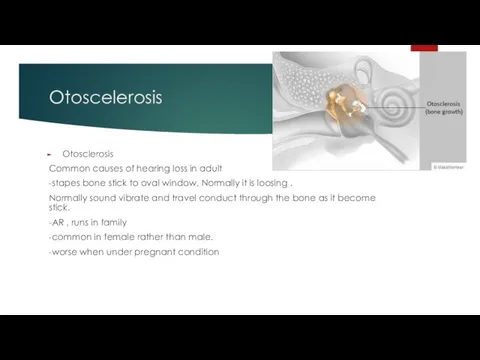
Otoscelerosis
Otosclerosis
Common causes of hearing loss in adult
-stapes bone stick to
Otoscelerosis
Otosclerosis
Common causes of hearing loss in adult
-stapes bone stick to
Management
hearing contain 2 parts - air conduction and nerve conduction.
your cases
Management
hearing contain 2 parts - air conduction and nerve conduction.
your cases

Case 7
A young woman at 10 weeks’ gestational age comes to
Case 7
A young woman at 10 weeks’ gestational age comes to

History
GM, I am Dr. XYZ… how are you today? I understand
History
GM, I am Dr. XYZ… how are you today? I understand

History
Reassure her that she will be monitored. Antenatal screening should be
History
Reassure her that she will be monitored. Antenatal screening should be

First trimester screening test
Combined Test-
■ A non-fasting blood test
First trimester screening test
Combined Test-
■ A non-fasting blood test

risk factor
Information from the ultrasound scan is reported to the pathology
risk factor
Information from the ultrasound scan is reported to the pathology
2nd trimester screening test
15 -17 weeks-solely blood tests.
– Triple
2nd trimester screening test
15 -17 weeks-solely blood tests.
– Triple

In high-risk pregnancies, diagnostic tests:
■ CVS
– Done ideally at
In high-risk pregnancies, diagnostic tests:
■ CVS
– Done ideally at

patient questions
Are the tests painful? Many women find the diagnostic tests
patient questions
Are the tests painful? Many women find the diagnostic tests

Case 8
In a GP setting. An 17 year-old boy complaining of
Case 8
In a GP setting. An 17 year-old boy complaining of

Differential
Duodenal injury
Local abdominal hematoma
Gall bladder injury
Testicular torison
UTI
Gall stone
Strangulated inguinal hernia
UTI
Ureter colic/stone
Adhesion
Differential
Duodenal injury
Local abdominal hematoma
Gall bladder injury
Testicular torison
UTI
Gall stone
Strangulated inguinal hernia
UTI
Ureter colic/stone
Adhesion

History
Vital stability of the child – B.P. -100/60, P.R- 120, RR-
History
Vital stability of the child – B.P. -100/60, P.R- 120, RR-

History
BINDS – Heel prick test was done ?( thyroid) Any concern
History
BINDS – Heel prick test was done ?( thyroid) Any concern
Physical examination
General appearance – distress & in pain , no signs
Physical examination
General appearance – distress & in pain , no signs
Explanation
Your son has a Duodenal injury in the tummy as I
Explanation
Your son has a Duodenal injury in the tummy as I
Case: 10
26 year old John has been brought by the police
Case: 10
26 year old John has been brought by the police
Assess patient’s injury, offer pain management
CONFIDENTIALITY
History
Can you tell me what happened
Assess patient’s injury, offer pain management
CONFIDENTIALITY
History
Can you tell me what happened
At hospital -> ever seen by a psychiatrist.
Yes. I think there
At hospital -> ever seen by a psychiatrist.
Yes. I think there
Psychosocial H/O
Home : Left home at 16 years. No contact with parents
Psychosocial H/O
Home : Left home at 16 years. No contact with parents
Management
Difficulty to treat because of late presentation and lack of
Management
Difficulty to treat because of late presentation and lack of
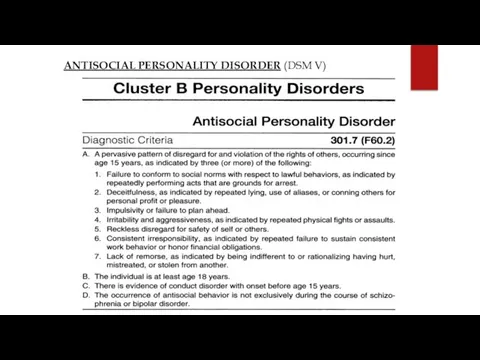
ANTISOCIAL PERSONALITY DISORDER (DSM V)
ANTISOCIAL PERSONALITY DISORDER (DSM V)

a mental disorder where a person shows no regard for right
a mental disorder where a person shows no regard for right
Symptoms
Deceitfulness
Non Conformity no respect for the law and have no boundaries.
Impulsivity
Aggression
Irresponsibility
Causes
Symptoms
Deceitfulness
Non Conformity no respect for the law and have no boundaries.
Impulsivity
Aggression
Irresponsibility
Causes

Reference
https://wayahead.org.au/mental-health-information/fact-sheets/
mental-illness-and-related/antisocial-personality-disorder/
Reference
https://wayahead.org.au/mental-health-information/fact-sheets/
mental-illness-and-related/antisocial-personality-disorder/
 Основы формирования здоровья детей: от 1 года до 3 лет
Основы формирования здоровья детей: от 1 года до 3 лет Сестринская помощь при вегетососудистой дистонии. Лекция 10
Сестринская помощь при вегетососудистой дистонии. Лекция 10 Энтеровирусная инфекция (ЭВИ) у детей
Энтеровирусная инфекция (ЭВИ) у детей Ультразвуковая диагностика заболеваний молочных желёз
Ультразвуковая диагностика заболеваний молочных желёз Синдром Бругада
Синдром Бругада Жировая эмболия
Жировая эмболия Партнерские роды
Партнерские роды Психика и сознание
Психика и сознание Еңбек жағдайын гигиеналықфизиологиялық бағалау: еңбектің ауырлығымен қарқындылығын, зияндылығы мен қауіптілігін
Еңбек жағдайын гигиеналықфизиологиялық бағалау: еңбектің ауырлығымен қарқындылығын, зияндылығы мен қауіптілігін Кумарины. Лекарственные растения и сырье, содержащие кумарины
Кумарины. Лекарственные растения и сырье, содержащие кумарины Вклад научных достижений кафедры хирургии в повышении качества медико-социальной экспертизы
Вклад научных достижений кафедры хирургии в повышении качества медико-социальной экспертизы Кровотечения в последовом и раннем послеродовом периодах
Кровотечения в последовом и раннем послеродовом периодах Миеломная болезнь (плазмоцитома)
Миеломная болезнь (плазмоцитома) Общение как взаимодействие. Интерактивная сторона общения
Общение как взаимодействие. Интерактивная сторона общения Основы микробиологии, санитарии и гигиены в пищевом производстве
Основы микробиологии, санитарии и гигиены в пищевом производстве Теория мотивации Д. Катца и Р. Кана
Теория мотивации Д. Катца и Р. Кана Парацельс – основатель ятрохимии
Парацельс – основатель ятрохимии Оптимизация процесса предоставления медицинской услуги в республиканской стоматологии
Оптимизация процесса предоставления медицинской услуги в республиканской стоматологии Первая помощь при прочих состояниях (ожоги, обморожения, отравления)
Первая помощь при прочих состояниях (ожоги, обморожения, отравления) О вкусном и полезном питании
О вкусном и полезном питании Виды лечения опухолей
Виды лечения опухолей Нановакцины и нанолекарства
Нановакцины и нанолекарства Трансплантация тарихы
Трансплантация тарихы Профилактика рака желудка
Профилактика рака желудка Сестринская помощь при артериальной гипертонии. Тема 4.2
Сестринская помощь при артериальной гипертонии. Тема 4.2 Анатомия, кровоснабжение, иннервация, физиология поджелудочной железы
Анатомия, кровоснабжение, иннервация, физиология поджелудочной железы Психология управленческой деятельности
Психология управленческой деятельности Наркомания
Наркомания