- Omphalocele and Gastroschisis

Содержание
- 2. Background: Gastroschisis and omphalocele are among the most frequently encountered congenital anomalies in pediatric surgery. Combined
- 3. Background: Many babies have correctable lesions and simply require routine pediatric care. For others, the abdominal
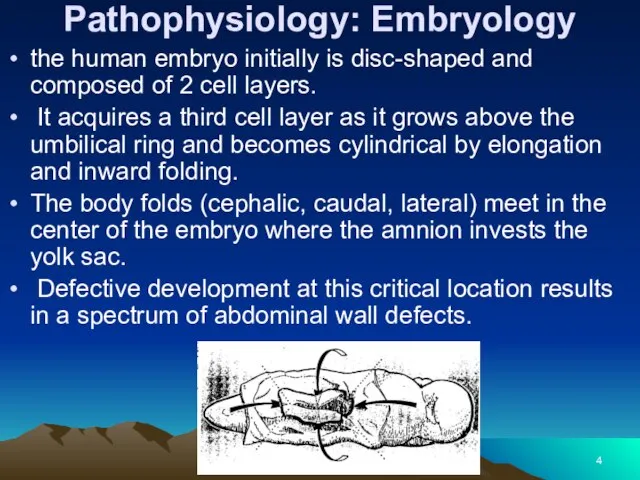
- 4. Pathophysiology: Embryology the human embryo initially is disc-shaped and composed of 2 cell layers. It acquires
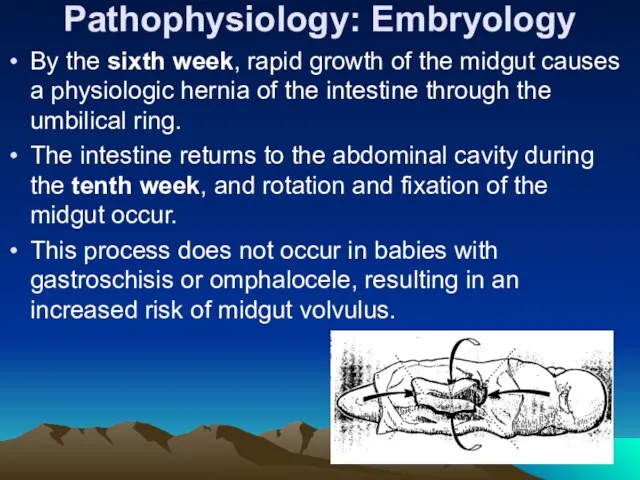
- 5. Pathophysiology: Embryology By the sixth week, rapid growth of the midgut causes a physiologic hernia of
- 6. Pathogenesis of omphalocele and gastroschisis Abdominal wall defects occur as a result of failure of the
- 7. Pathogenesis of Omphalocele In babies with omphalocele failure of central fusion at the umbilical ring by
- 8. Baby with an omphalocele.
- 9. Baby with a ruptured omphalocele.
- 10. Pathogenesis of gastroschisis Possible explanations of the embryology of abdominal wall defect in gastroschisis include the
- 11. Baby with an umbilical cord hernia.
- 12. Frequency: In the US: Combined incidence of omphalocele and gastroschisis is 1 in 2000 births. Incidence
- 13. Mortality/Morbidity: Over the past 30 years, the survival rate of babies with gastroschisis and omphalocele has
- 14. Mortality/Morbidity: Long-term morbidity from gastroschisis is related to intestinal dysfunction and wound problems. Short gut syndrome
- 15. Mortality/Morbidity: Management of babies with short gut syndrome also has improved significantly as a result of
- 16. Mortality/Morbidity: Poor healing of the abdominal wound usually results in a ventral hernia, which may require
- 17. Mortality/Morbidity: Even with successful repair, which usually requires a synthetic patch, and good clinical outcome, the
- 18. CLINICAL Physical: Omphalocele In babies with omphaloceles, the size of the abdominal wall defect ranges from
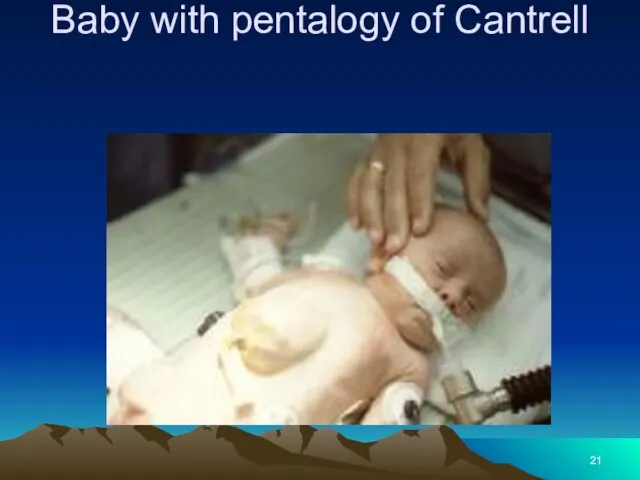
- 19. CLINICAL Babies with the Beckwith-Wiedemann syndrome (ie, macroglossia, gigantism) have large, rounded facial features, hypoglycemia from
- 20. Beckwith-Wiedemann syndrome
- 21. Baby with pentalogy of Cantrell
- 22. CLINICAL- Gastroschisis The defect is fairly uniform in size and location; a 5-cm vertical opening to
- 23. Baby with gastroschisis and associated intestinal atresia.
- 24. baby with gastroschisis and colon atresia.
- 25. Causes: Factors associated with high-risk pregnancies, such as maternal illness and infection, drug use, smoking, and
- 26. DIFFERENTIALS Other Problems to be Considered: In babies with omphalocele, a 35-80% incidence of other clinical
- 27. WORKUP Lab Studies: Maternal serum alpha-fetoprotein Prenatal diagnosis of abdominal wall defects can be made by
- 28. WORKUP Imaging Studies: Fetal sonography may detect a genetic abnormality, with identification of a structural marker
- 29. TREATMENT Medical Care: Intestinal inflammation Intestinal inflammation may occur with either gastroschisis or ruptured omphalocele. The
- 30. TREATMENT Intact omphalocele Usually, neonates with intact omphalocele are in no distress, unless associated pulmonary hypoplasia
- 31. TREATMENT The omphalocele should be supported to avoid excessive traction to the mesentery. Give prophylactic antibiotics
- 32. TREATMENT Gastroschisis Respiratory distress in neonates with gastroschisis may respond to gastric decompression, although endotracheal intubation
- 33. TREATMENT-Surgical Care: Omphalocele Ambroise Pare, the 17th-century French surgeon, accurately described omphalocele and the dire consequences
- 34. TREATMENT-Surgical Care: Healing may be hastened by surgically mobilizing skin flaps sufficient to cover the omphalocele
- 35. TREATMENT-Surgical Care Gastroschisis In 1969, Allen and Wrenn adapted Schuster’s technique for treatment of gastroschisis. Silastic
- 36. TREATMENT-Surgical Care In addition, tight closure of the abdominal cavity impedes venous return to the heart,
- 37. Consultations: Neonatologists and pediatric surgeons usually care for babies with these anomalies. Consult with cardiology, pulmonology,
- 38. Diet: Babies with omphalocele usually do not require special formulas; their intestines are typically normal, with
- 39. Activity: A child with a repaired giant omphalocele has an epigastric liver. In this location, the
- 40. FOLLOW-UP Further Inpatient Care: Omphalocele Babies with omphalocele usually have rapid return of intestinal function after
- 41. FOLLOW-UP Gastroschisis Even if primary closure of the abdominal wall defect is obtained, a period of
- 42. Silo closure of a baby with gastroschisis.
- 43. FOLLOW-UP Further Outpatient Care: After hospital discharge, babies require close follow-up care to assess growth and
- 44. FOLLOW-UP Transfer: The best way to treat the exposed intestines of a baby with gastroschisis who
- 45. The patient’s condition improved dramatically once closure of the abdominal cavity was achieved. Again, the author
- 46. Prognosis: Omphalocele Prognosis is dependent upon the severity of the associated problems. Babies with omphalocele are
- 47. Prognosis Gastroschisis Prognosis is dependent mainly upon severity of associated problems, including prematurity, intestinal atresia, short
- 48. Patient Education: Instruct parents regarding the significance of bilious (green) vomiting, since these babies may develop
- 49. Special Concerns: Prenatal care and planning With increased availability of sonography, prenatal diagnosis is more frequent.
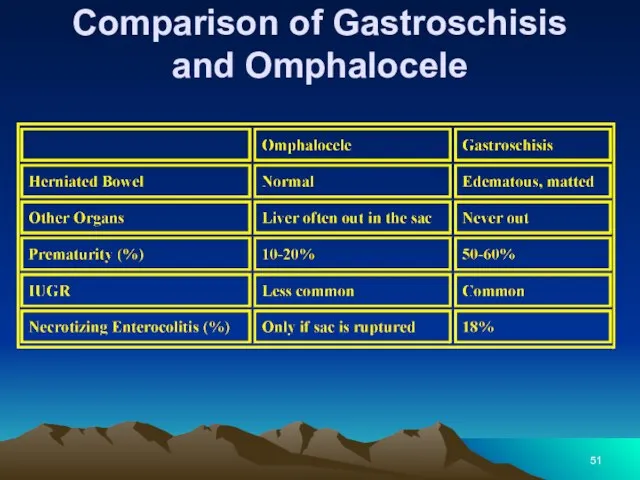
- 50. Comparison of Gastroschisis and Omphalocele
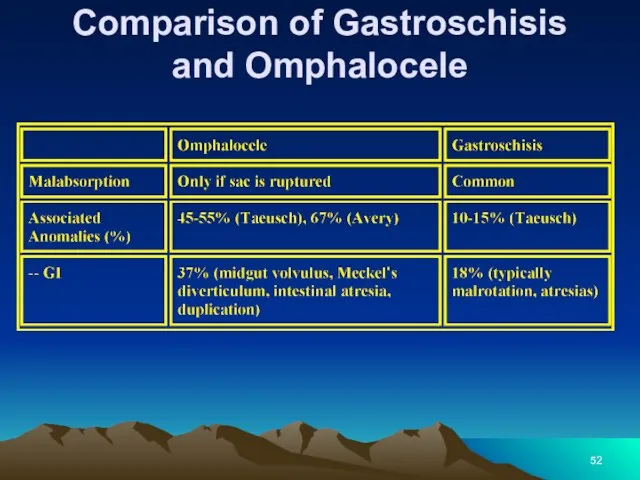
- 51. Comparison of Gastroschisis and Omphalocele
- 52. Comparison of Gastroschisis and Omphalocele
- 53. Completed reduction of the bowel contained within the silo; the silo is about to be removed
- 54. Baby with a giant omphalocele.
- 55. Same patient as in slide 54. Closure of the giant omphalocele using a synthetic patch.
- 56. Same patient as in slides 54-55. Tightening the abdominal wall closure
- 57. Same patient as in slides 54-56. Flank flaps were used to close the giant omphalocele in
- 59. Скачать презентацию
Background:
Gastroschisis and omphalocele are among the most frequently encountered congenital anomalies
Background:
Gastroschisis and omphalocele are among the most frequently encountered congenital anomalies
Background:
Many babies have correctable lesions and simply require routine pediatric care.
Background:
Many babies have correctable lesions and simply require routine pediatric care.
Pathophysiology: Embryology
the human embryo initially is disc-shaped and composed of 2
Pathophysiology: Embryology
the human embryo initially is disc-shaped and composed of 2
Pathophysiology: Embryology
By the sixth week, rapid growth of the midgut causes
Pathophysiology: Embryology
By the sixth week, rapid growth of the midgut causes
Pathogenesis of omphalocele and gastroschisis
Abdominal wall defects occur as a
Pathogenesis of omphalocele and gastroschisis
Abdominal wall defects occur as a
Pathogenesis of Omphalocele
In babies with omphalocele failure of central fusion at
Pathogenesis of Omphalocele
In babies with omphalocele failure of central fusion at

Baby with an omphalocele.
Baby with an omphalocele.
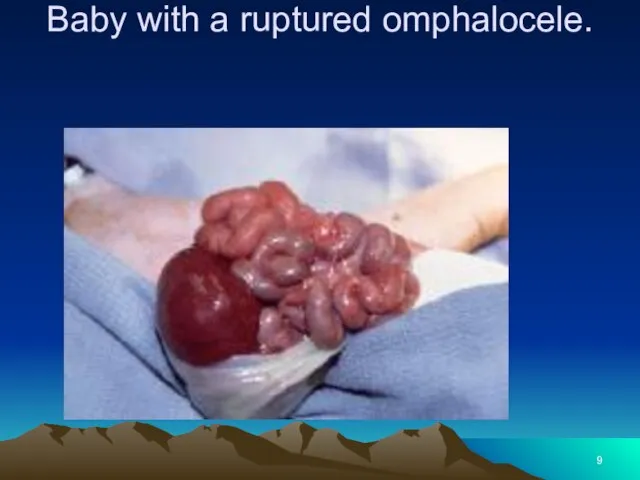
Baby with a ruptured omphalocele.
Baby with a ruptured omphalocele.
Pathogenesis of gastroschisis
Possible explanations of the embryology of abdominal wall defect
Pathogenesis of gastroschisis
Possible explanations of the embryology of abdominal wall defect
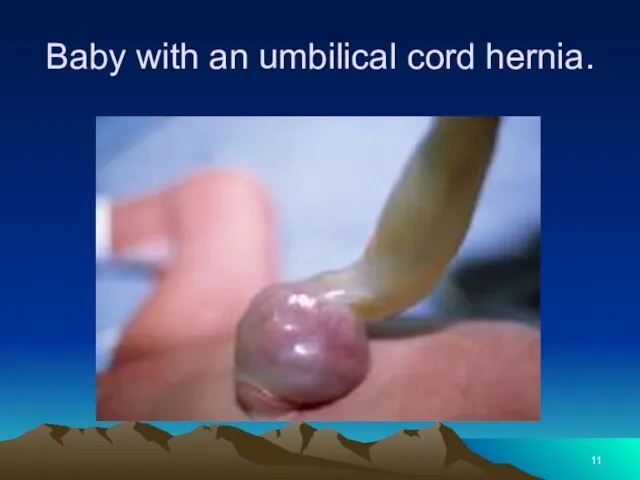
Baby with an umbilical cord hernia.
Baby with an umbilical cord hernia.
Frequency:
In the US: Combined incidence of omphalocele and gastroschisis is
Frequency:
In the US: Combined incidence of omphalocele and gastroschisis is
Mortality/Morbidity:
Over the past 30 years, the survival rate of babies with
Mortality/Morbidity:
Over the past 30 years, the survival rate of babies with
Mortality/Morbidity:
Long-term morbidity from gastroschisis is related to intestinal dysfunction and wound
Mortality/Morbidity:
Long-term morbidity from gastroschisis is related to intestinal dysfunction and wound
Mortality/Morbidity:
Management of babies with short gut syndrome also has improved significantly
Mortality/Morbidity:
Management of babies with short gut syndrome also has improved significantly
Mortality/Morbidity:
Poor healing of the abdominal wound usually results in a ventral
Mortality/Morbidity:
Poor healing of the abdominal wound usually results in a ventral
Mortality/Morbidity:
Even with successful repair, which usually requires a synthetic patch, and
Mortality/Morbidity:
Even with successful repair, which usually requires a synthetic patch, and
CLINICAL
Physical:
Omphalocele
In babies with omphaloceles, the size of the abdominal
CLINICAL
Physical:
Omphalocele
In babies with omphaloceles, the size of the abdominal
CLINICAL
Babies with the Beckwith-Wiedemann syndrome (ie, macroglossia, gigantism) have large,
CLINICAL
Babies with the Beckwith-Wiedemann syndrome (ie, macroglossia, gigantism) have large,

Beckwith-Wiedemann syndrome
Beckwith-Wiedemann syndrome
Baby with pentalogy of Cantrell
Baby with pentalogy of Cantrell
CLINICAL- Gastroschisis
The defect is fairly uniform in size and location; a
CLINICAL- Gastroschisis
The defect is fairly uniform in size and location; a

Baby with gastroschisis and associated intestinal atresia.
Baby with gastroschisis and associated intestinal atresia.

baby with gastroschisis and colon atresia.
baby with gastroschisis and colon atresia.
Causes:
Factors associated with high-risk pregnancies, such as maternal illness and
Causes:
Factors associated with high-risk pregnancies, such as maternal illness and
DIFFERENTIALS
Other Problems to be Considered:
In babies with omphalocele, a
DIFFERENTIALS
Other Problems to be Considered:
In babies with omphalocele, a
WORKUP
Lab Studies:
Maternal serum alpha-fetoprotein
Prenatal diagnosis of abdominal wall defects
WORKUP
Lab Studies:
Maternal serum alpha-fetoprotein
Prenatal diagnosis of abdominal wall defects
WORKUP
Imaging Studies:
Fetal sonography may detect a genetic abnormality, with
WORKUP
Imaging Studies:
Fetal sonography may detect a genetic abnormality, with
TREATMENT
Medical Care:
Intestinal inflammation
Intestinal inflammation may occur with either gastroschisis
TREATMENT
Medical Care:
Intestinal inflammation
Intestinal inflammation may occur with either gastroschisis
TREATMENT
Intact omphalocele
Usually, neonates with intact omphalocele are in no distress,
TREATMENT
Intact omphalocele
Usually, neonates with intact omphalocele are in no distress,
TREATMENT
The omphalocele should be supported to avoid excessive traction to the
TREATMENT
The omphalocele should be supported to avoid excessive traction to the
TREATMENT
Gastroschisis
Respiratory distress in neonates with gastroschisis may respond to gastric
TREATMENT
Gastroschisis
Respiratory distress in neonates with gastroschisis may respond to gastric
TREATMENT-Surgical Care:
Omphalocele
Ambroise Pare, the 17th-century French surgeon, accurately described omphalocele
TREATMENT-Surgical Care:
Omphalocele
Ambroise Pare, the 17th-century French surgeon, accurately described omphalocele
TREATMENT-Surgical Care:
Healing may be hastened by surgically mobilizing skin flaps sufficient
TREATMENT-Surgical Care:
Healing may be hastened by surgically mobilizing skin flaps sufficient
TREATMENT-Surgical Care
Gastroschisis
In 1969, Allen and Wrenn adapted Schuster’s technique for treatment
TREATMENT-Surgical Care
Gastroschisis
In 1969, Allen and Wrenn adapted Schuster’s technique for treatment
TREATMENT-Surgical Care
In addition, tight closure of the abdominal cavity impedes venous
TREATMENT-Surgical Care
In addition, tight closure of the abdominal cavity impedes venous
Consultations:
Neonatologists and pediatric surgeons usually care for babies with these
Consultations:
Neonatologists and pediatric surgeons usually care for babies with these
Diet:
Babies with omphalocele usually do not require special formulas; their intestines
Diet:
Babies with omphalocele usually do not require special formulas; their intestines
Activity:
A child with a repaired giant omphalocele has an epigastric liver.
Activity:
A child with a repaired giant omphalocele has an epigastric liver.
FOLLOW-UP
Further Inpatient Care:
Omphalocele
Babies with omphalocele usually have rapid return
FOLLOW-UP
Further Inpatient Care:
Omphalocele
Babies with omphalocele usually have rapid return
FOLLOW-UP
Gastroschisis
Even if primary closure of the abdominal wall defect is
FOLLOW-UP
Gastroschisis
Even if primary closure of the abdominal wall defect is

Silo closure of a baby with gastroschisis.
Silo closure of a baby with gastroschisis.
FOLLOW-UP
Further Outpatient Care:
After hospital discharge, babies require close follow-up
FOLLOW-UP
Further Outpatient Care:
After hospital discharge, babies require close follow-up
FOLLOW-UP
Transfer:
The best way to treat the exposed intestines of
FOLLOW-UP
Transfer:
The best way to treat the exposed intestines of
The patient’s condition improved dramatically once closure of the abdominal cavity
The patient’s condition improved dramatically once closure of the abdominal cavity
Prognosis:
Omphalocele
Prognosis is dependent upon the severity of the associated problems.
Prognosis:
Omphalocele
Prognosis is dependent upon the severity of the associated problems.
Prognosis
Gastroschisis
Prognosis is dependent mainly upon severity of associated problems, including prematurity,
Prognosis
Gastroschisis
Prognosis is dependent mainly upon severity of associated problems, including prematurity,
Patient Education:
Instruct parents regarding the significance of bilious (green) vomiting,
Patient Education:
Instruct parents regarding the significance of bilious (green) vomiting,
Special Concerns:
Prenatal care and planning
With increased availability of sonography, prenatal
Special Concerns:
Prenatal care and planning
With increased availability of sonography, prenatal
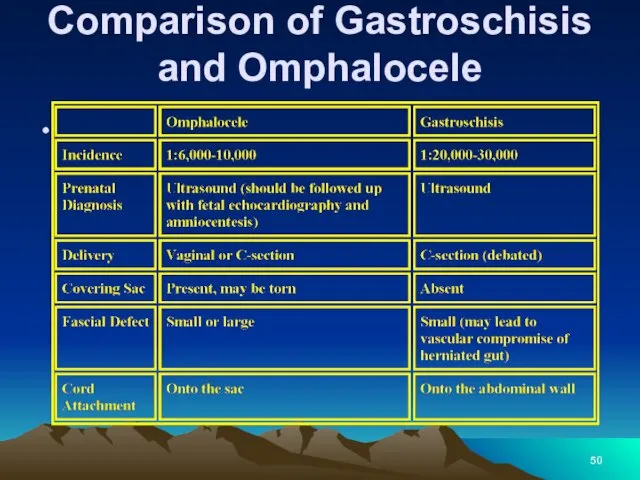
Comparison of Gastroschisis and Omphalocele
Comparison of Gastroschisis and Omphalocele
Comparison of Gastroschisis and Omphalocele
Comparison of Gastroschisis and Omphalocele
Comparison of Gastroschisis and Omphalocele
Comparison of Gastroschisis and Omphalocele
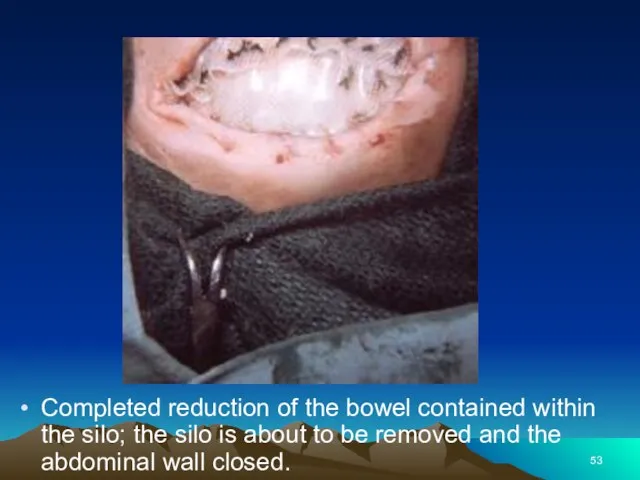
Completed reduction of the bowel contained within the silo; the silo
Completed reduction of the bowel contained within the silo; the silo

Baby with a giant omphalocele.
Baby with a giant omphalocele.

Same patient as in slide 54. Closure of the giant omphalocele
Same patient as in slide 54. Closure of the giant omphalocele

Same patient as in slides 54-55. Tightening the abdominal wall closure
Same patient as in slides 54-55. Tightening the abdominal wall closure

Same patient as in slides 54-56. Flank flaps were used to
Same patient as in slides 54-56. Flank flaps were used to
 Основы помповой инсулинотерапии
Основы помповой инсулинотерапии Острый аппендицит у детей
Острый аппендицит у детей Наследственные болезни человека
Наследственные болезни человека Диагноз: вторичное частичное отсутствие зубов
Диагноз: вторичное частичное отсутствие зубов Зарядка для глаз
Зарядка для глаз Заболевания мочевыводящих путей у беременных
Заболевания мочевыводящих путей у беременных Нарушения внимания при локальных поражениях мозга
Нарушения внимания при локальных поражениях мозга Бешенство. Вирус бешенства
Бешенство. Вирус бешенства Reflexes
Reflexes Хронический фиброзный периодонтит. Особенности клинического течения и диагностики
Хронический фиброзный периодонтит. Особенности клинического течения и диагностики ВІЛ-інфекція Історія відкриття. Етіологія. Епідеміологія. Патогенез. Клінічні прояви
ВІЛ-інфекція Історія відкриття. Етіологія. Епідеміологія. Патогенез. Клінічні прояви Эндовидеохирургия
Эндовидеохирургия Созылмалы өкпе текті жүрек
Созылмалы өкпе текті жүрек Малярия
Малярия Уақытша еңбекке жарамсыздық
Уақытша еңбекке жарамсыздық Облитерирующий атеросклероз аорты и артерий нижних конечностей
Облитерирующий атеросклероз аорты и артерий нижних конечностей Остановка сердца
Остановка сердца Становление естественнонаучных знаний в эпоху Возрождения
Становление естественнонаучных знаний в эпоху Возрождения Лекарственные средства, влияющие на функции органов дыхания
Лекарственные средства, влияющие на функции органов дыхания Охрана окружающей среды как мера профилактики заболеваний органов дыхания
Охрана окружающей среды как мера профилактики заболеваний органов дыхания Неврологиялық қарау әдістері
Неврологиялық қарау әдістері Идиопатический анкилозирующий спондилоартрит (болезнь Бехтерева)
Идиопатический анкилозирующий спондилоартрит (болезнь Бехтерева) Тератогенные факторы. Фармакологические тератогенны
Тератогенные факторы. Фармакологические тератогенны Развитие гемоперикарда при чрескожном коронарном вмешательстве
Развитие гемоперикарда при чрескожном коронарном вмешательстве Физическое воспитание ребенка первого года жизни
Физическое воспитание ребенка первого года жизни Методы лучевой диагностики в неврологии
Методы лучевой диагностики в неврологии Жатырдың тусуі
Жатырдың тусуі Реанимация новорожденных (программа реанимации новорожденных)
Реанимация новорожденных (программа реанимации новорожденных)