- Pathomorphology of lungs lesions in new coronavirus infection Covid-19

Содержание
- 2. First Autopsy Case Report Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C,
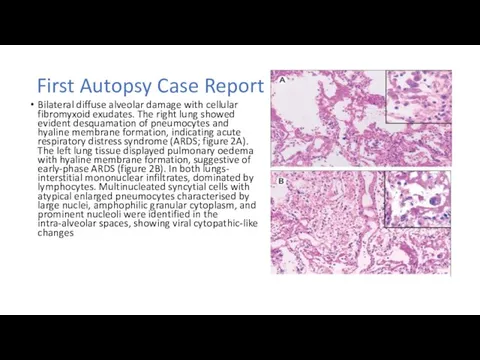
- 3. First Autopsy Case Report Bilateral diffuse alveolar damage with cellular fibromyxoid exudates. The right lung showed
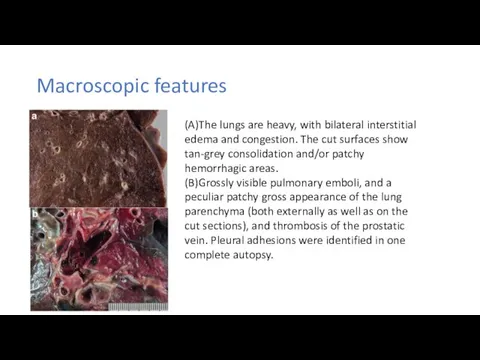
- 4. Macroscopic features (A)The lungs are heavy, with bilateral interstitial edema and congestion. The cut surfaces show
- 5. Imaging
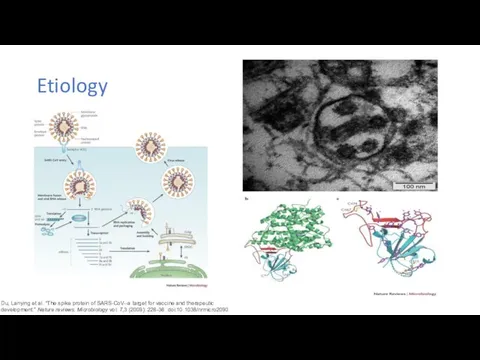
- 6. Etiology Du, Lanying et al. “The spike protein of SARS-CoV--a target for vaccine and therapeutic development.”
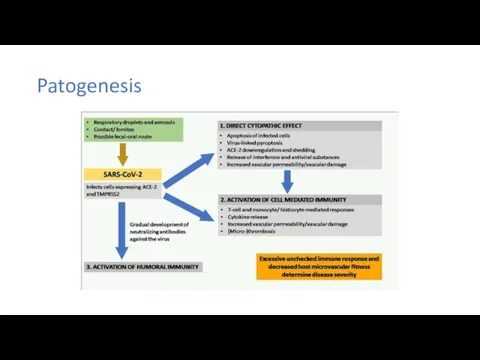
- 7. Patogenesis
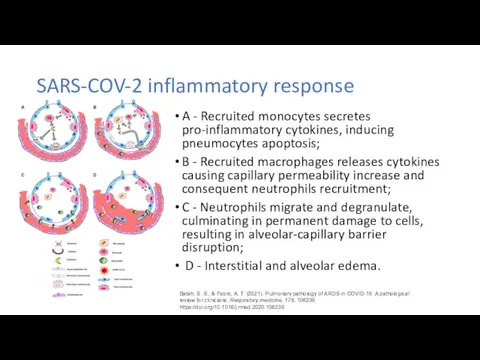
- 8. SARS-COV-2 inflammatory response A - Recruited monocytes secretes pro-inflammatory cytokines, inducing pneumocytes apoptosis; B - Recruited
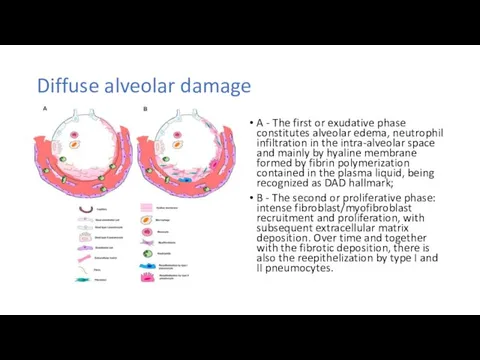
- 9. Diffuse alveolar damage A - The first or exudative phase constitutes alveolar edema, neutrophil infiltration in
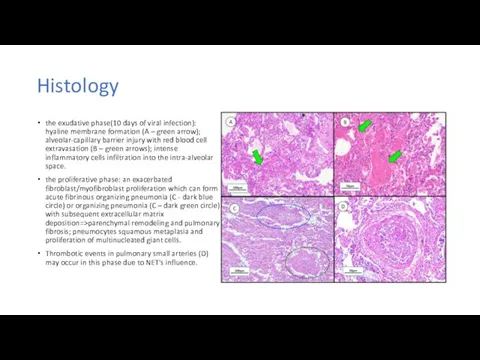
- 10. Histology the exudative phase(10 days of viral infection): hyaline membrane formation (A – green arrow); alveolar-capillary
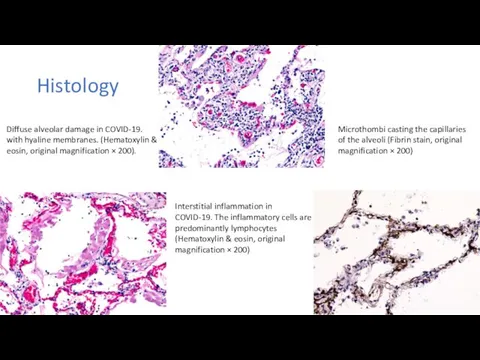
- 11. Histology Microthombi casting the capillaries of the alveoli (Fibrin stain, original magnification × 200) Interstitial inflammation
- 12. Airway inflammation in COVID-19: a Chronic inflammation composed mainly of lymphocytes, involving the bronchial mucosa (Hematoxylin
- 13. Endothelial cell dysfunction Post-mortem lung specimen showed thickened lung septa, including a large arterial vessel with
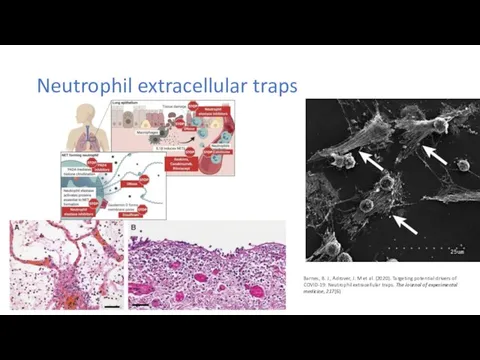
- 14. Neutrophil extracellular traps Barnes, B. J., Adrover, J. M et al. (2020). Targeting potential drivers of
- 15. Complement associated microvascular injury and thrombosis
- 16. Demonstration of co-localization of complement components with SARS-CoV2 spike glycoprotein in the lung (A)Deposition of C4d
- 17. Is it “typical” ARDS? Li X, Ma X. Acute respiratory failure in COVID-19: is it "typical"
- 19. Скачать презентацию
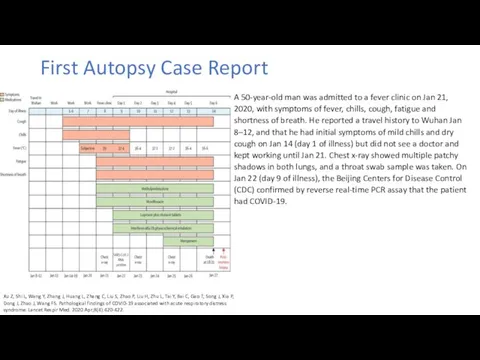
First Autopsy Case Report
Xu Z, Shi L, Wang Y, Zhang J,
First Autopsy Case Report
Xu Z, Shi L, Wang Y, Zhang J,
First Autopsy Case Report
Bilateral diffuse alveolar damage with cellular fibromyxoid exudates.
First Autopsy Case Report
Bilateral diffuse alveolar damage with cellular fibromyxoid exudates.
Macroscopic features
(A)The lungs are heavy, with bilateral interstitial edema and congestion.
Macroscopic features
(A)The lungs are heavy, with bilateral interstitial edema and congestion.
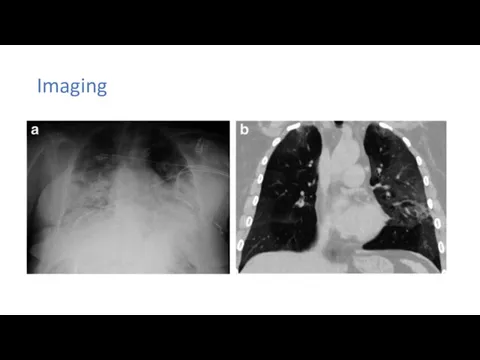
Imaging
Imaging
Etiology
Du, Lanying et al. “The spike protein of SARS-CoV--a target for
Etiology
Du, Lanying et al. “The spike protein of SARS-CoV--a target for
Patogenesis
Patogenesis
SARS-COV-2 inflammatory response
A - Recruited monocytes secretes pro-inflammatory cytokines, inducing pneumocytes
SARS-COV-2 inflammatory response
A - Recruited monocytes secretes pro-inflammatory cytokines, inducing pneumocytes
Diffuse alveolar damage
A - The first or exudative phase constitutes alveolar
Diffuse alveolar damage
A - The first or exudative phase constitutes alveolar
Histology
the exudative phase(10 days of viral infection): hyaline membrane formation (A
Histology
the exudative phase(10 days of viral infection): hyaline membrane formation (A
Histology
Microthombi casting the capillaries of the alveoli (Fibrin stain, original magnification
Histology
Microthombi casting the capillaries of the alveoli (Fibrin stain, original magnification
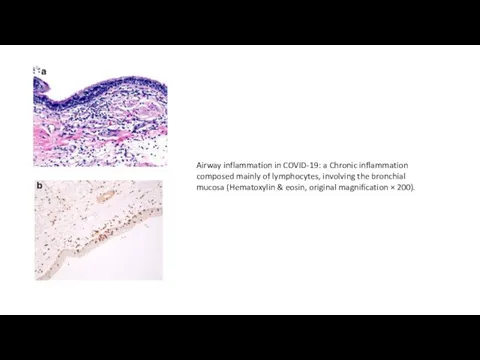
Airway inflammation in COVID-19: a Chronic inflammation composed mainly of lymphocytes, involving
Airway inflammation in COVID-19: a Chronic inflammation composed mainly of lymphocytes, involving

Endothelial cell dysfunction
Post-mortem lung specimen showed thickened lung septa, including a
Endothelial cell dysfunction
Post-mortem lung specimen showed thickened lung septa, including a
Neutrophil extracellular traps
Barnes, B. J., Adrover, J. M et al. (2020).
Neutrophil extracellular traps
Barnes, B. J., Adrover, J. M et al. (2020).
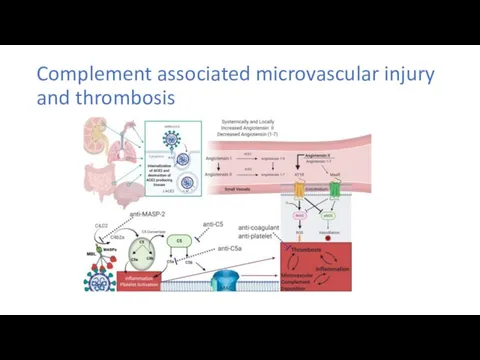
Complement associated microvascular injury and thrombosis
Complement associated microvascular injury and thrombosis
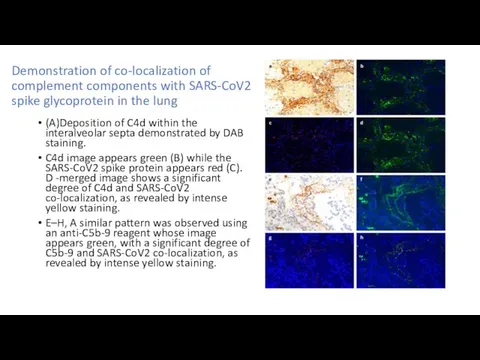
Demonstration of co-localization of complement components with SARS-CoV2 spike glycoprotein in
Demonstration of co-localization of complement components with SARS-CoV2 spike glycoprotein in
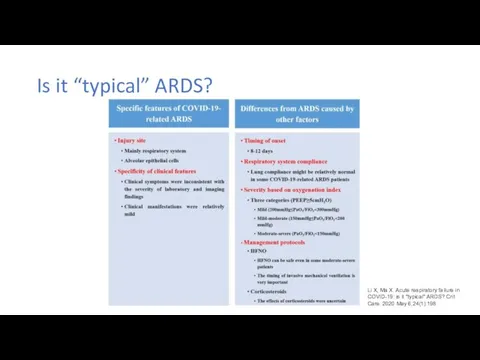
Is it “typical” ARDS?
Li X, Ma X. Acute respiratory failure in
Is it “typical” ARDS?
Li X, Ma X. Acute respiratory failure in
 Методика проведения искусственного дыхания
Методика проведения искусственного дыхания Введение в патофизиологию
Введение в патофизиологию Қозу
Қозу Острая почечная недостаточность
Острая почечная недостаточность Репродуктивное здоровье
Репродуктивное здоровье Доброкачественные и злокачественные опухоли почек
Доброкачественные и злокачественные опухоли почек Фарингоспрей заботиться о горле
Фарингоспрей заботиться о горле Клиническая генетика
Клиническая генетика Дифференциальная диагностика симптомов портальной гипертензии
Дифференциальная диагностика симптомов портальной гипертензии Дерматологические аспекты ВИЧ-инфекции
Дерматологические аспекты ВИЧ-инфекции Антимикробные лекарстенные средства
Антимикробные лекарстенные средства Внематочная беременность – новый взгляд
Внематочная беременность – новый взгляд Созылмалы аурулармен балаларды диспансерлік бақылаудың принциптері
Созылмалы аурулармен балаларды диспансерлік бақылаудың принциптері Холера. Этиология. Эпидемиология. Механизм заражения холерой
Холера. Этиология. Эпидемиология. Механизм заражения холерой БЛХ. Гипоталамо-гипофизарные заболевания
БЛХ. Гипоталамо-гипофизарные заболевания Виды и типы ортодонтических аппаратов и основы ортодонтического лечения
Виды и типы ортодонтических аппаратов и основы ортодонтического лечения Вирус иммунодефицита человека
Вирус иммунодефицита человека Особенности психики детей дошкольного возраста
Особенности психики детей дошкольного возраста Артериальная гипертензия
Артериальная гипертензия Производные аминоалкилбензолов. (Тема 3)
Производные аминоалкилбензолов. (Тема 3) Основы эндоурологии. Основные инструменты в эндоурологии
Основы эндоурологии. Основные инструменты в эндоурологии Новый способ восстановления непрерывности пищеварительного тракта после гастрэктомии
Новый способ восстановления непрерывности пищеварительного тракта после гастрэктомии Сүйек буын аурулары зақымданғанда визуалды диагностика
Сүйек буын аурулары зақымданғанда визуалды диагностика Применение различных средств индивидуальной защиты у больных и контактных covid-19
Применение различных средств индивидуальной защиты у больных и контактных covid-19 Контроль диабета при беременности
Контроль диабета при беременности Методы мозгового штурма
Методы мозгового штурма Нейропсихологические синдромы поражения теменной области головного мозга
Нейропсихологические синдромы поражения теменной области головного мозга Оформление медицинской документации
Оформление медицинской документации