- Cfu. Department of obs. & gyn. 1

Содержание
- 2. Fetal malpresentation refers to fetal presenting part other than vertex and includes breech, transverse, face, brow,
- 3. • The woman has had more than one pregnancy • There is more than one fetus
- 4. BREECH x Complete (Flexed) Breech Presentation x Footling Breech Presentation x Frank (Extended) Breech Presentation x
- 5. Face Presentation
- 6. Face Presentation Definition It is a cephalic presentation in which the head is completely extended. •
- 7. Aetiology • l.Primary face: a. It is less common. b. It occurs during pregnancy. c. It
- 8. Aetiology • Secondary face: a. It is more common. b. It occurs during labour. c. It
- 9. Positions a. Right mento-posterior (RMP). b. Left mento-posterior (LMP). c. Left mento-anterior (LMA). d. Right mento-anterior
- 10. Positions • The first position (RMP) corresponds to the first normal position (LOA) as the back
- 11. Diagnosis During pregnancy (difficult) * The back is difficult to feel. * The limbs are felt
- 12. Diagnosis * During labour Vaginal examination shows the following identifying features for face: * supra-orbital ridges,
- 13. • Late in labour, the face becomes oedematous (tumefaction) so it can be misdiagnosed as a
- 14. The following points can differentiate in-between: The foetal mouth and malar processes form the apexes of
- 15. Mechanism of Labour • Mento-anterior position • Descent. • Engagement by submento-bregmatic diameter 9.5 cm. •
- 16. Engagement is delayed because: • The biparietal diameter does not pass the plane of pelvic inlet
- 17. Mento-posterior position a. Long anterior rotation 3/8 circle (2/3 of cases): so the head is delivered
- 18. * Direct mento-posterior, unlike direct occipito-posterior, cannot be delivered because: * Delivery should occur by extension
- 19. Management of Labour * Mento-anterior * First stage: as in occipito-posterior. * Second stage: > Spontaneous
- 20. Management of Labour • Mento-posterior • First stage: as mento-anterior. • Second stage:Wait for long anterior
- 21. Management of Labour • Failure of long anterior rotation 3/8 circle or development of foetal or
- 22. Brow Presentation
- 23. Brow Presentation • Definition • It is a cephalic presentation in which the head is midway
- 24. Diagnosis During pregnancy: • It is difficult. • The occiput and sinciput may be felt at
- 25. Diagnosis During labour: • In addition to the previous findings, vaginal examination reveals the following features:
- 26. Mechanism of Labour * Persistent brow: The engagement diameter is the mento-vertical 13.5 cm which is
- 27. Management * Early in the first stage: > Exclude contracted pelvis, if present do caesarean section.
- 28. Management * Early in the first stage:> Exclude contracted pelvis, if present do caesarean section. >The
- 29. Management In the second stage: The case is considered as persistent brow so: > Caesarean section
- 31. Скачать презентацию
Fetal malpresentation refers to fetal presenting part other than vertex and
Fetal malpresentation refers to fetal presenting part other than vertex and
• The woman has had more than one pregnancy
• There is
• The woman has had more than one pregnancy
• There is
BREECH
x Complete (Flexed) Breech Presentation x Footling Breech Presentation x Frank
BREECH
x Complete (Flexed) Breech Presentation x Footling Breech Presentation x Frank

Face Presentation
Face Presentation
Face Presentation
Definition
It is a cephalic presentation in which the head is
Face Presentation
Definition
It is a cephalic presentation in which the head is
Aetiology
• l.Primary face:
a. It is less common.
b. It occurs during pregnancy.
c.
Aetiology
• l.Primary face:
a. It is less common.
b. It occurs during pregnancy.
c.
Aetiology
• Secondary face:
a. It is more common.
b. It occurs during labour.
c.
Aetiology
• Secondary face:
a. It is more common.
b. It occurs during labour.
c.
Positions
a. Right mento-posterior (RMP).
b. Left mento-posterior (LMP).
c. Left mento-anterior (LMA).
d. Right
Positions
a. Right mento-posterior (RMP).
b. Left mento-posterior (LMP).
c. Left mento-anterior (LMA).
d. Right
Positions
• The first position (RMP) corresponds to the first normal position
Positions
• The first position (RMP) corresponds to the first normal position
Diagnosis
During pregnancy (difficult) * The back is difficult to feel.
* The
Diagnosis
During pregnancy (difficult) * The back is difficult to feel.
* The
Diagnosis
* During labour
Vaginal examination shows the following identifying features for face:
*
Diagnosis
* During labour
Vaginal examination shows the following identifying features for face:
*
• Late in labour, the face becomes oedematous (tumefaction) so it
• Late in labour, the face becomes oedematous (tumefaction) so it
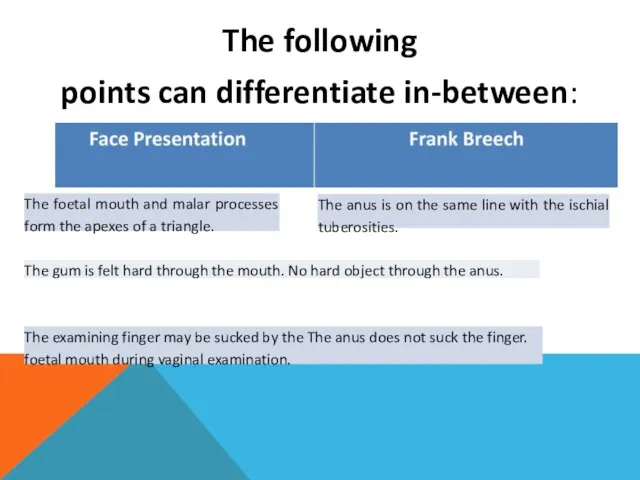
The following
points can differentiate in-between:
The foetal mouth and malar processes form
The following
points can differentiate in-between:
The foetal mouth and malar processes form
Mechanism of Labour
• Mento-anterior position
• Descent.
• Engagement by submento-bregmatic diameter 9.5
Mechanism of Labour
• Mento-anterior position
• Descent.
• Engagement by submento-bregmatic diameter 9.5
Engagement is delayed because:
• The biparietal diameter does not pass the
Engagement is delayed because:
• The biparietal diameter does not pass the
Mento-posterior position
a. Long anterior rotation 3/8 circle (2/3 of cases): so
Mento-posterior position
a. Long anterior rotation 3/8 circle (2/3 of cases): so
* Direct mento-posterior, unlike direct occipito-posterior, cannot be delivered because:
* Delivery
* Direct mento-posterior, unlike direct occipito-posterior, cannot be delivered because:
* Delivery
Management of Labour
* Mento-anterior
* First stage: as in occipito-posterior.
* Second stage:
>
Management of Labour
* Mento-anterior
* First stage: as in occipito-posterior.
* Second stage:
>
Management of Labour
• Mento-posterior
• First stage: as mento-anterior.
• Second stage:Wait for
Management of Labour
• Mento-posterior
• First stage: as mento-anterior.
• Second stage:Wait for
Management of Labour
• Failure of long anterior rotation 3/8 circle or
Management of Labour
• Failure of long anterior rotation 3/8 circle or
Brow Presentation
Brow Presentation
Brow Presentation
• Definition
• It is a cephalic presentation in which the
Brow Presentation
• Definition
• It is a cephalic presentation in which the
Diagnosis
During pregnancy:
• It is difficult.
• The occiput and sinciput may be
Diagnosis
During pregnancy:
• It is difficult.
• The occiput and sinciput may be
Diagnosis
During labour:
• In addition to the previous findings, vaginal examination reveals
Diagnosis
During labour:
• In addition to the previous findings, vaginal examination reveals
Mechanism of Labour
* Persistent brow:
The engagement diameter is the mento-vertical 13.5
Mechanism of Labour
* Persistent brow:
The engagement diameter is the mento-vertical 13.5
Management
* Early in the first stage:
> Exclude contracted pelvis, if present
Management
* Early in the first stage:
> Exclude contracted pelvis, if present
Management
* Early in the first stage:> Exclude contracted pelvis, if present
Management
* Early in the first stage:> Exclude contracted pelvis, if present
Management
In the second stage: The case is considered as persistent brow
Management
In the second stage: The case is considered as persistent brow
 20170218_muzyka_2_klass_krossvord
20170218_muzyka_2_klass_krossvord IBM-совместимые Macintosh
IBM-совместимые Macintosh Требования к устройству мостового полотна искусственных дорожных сооружений
Требования к устройству мостового полотна искусственных дорожных сооружений Маф для детских площадок из современных
Маф для детских площадок из современных Деревянное профилированное домостроение
Деревянное профилированное домостроение Религиозность
Религиозность Технология вытягивания тяг от руки
Технология вытягивания тяг от руки На внимание и память жалуются все, на рассудок – никто
На внимание и память жалуются все, на рассудок – никто 20130117_mezhdunaodnoei_gumanitarnoe_pravo
20130117_mezhdunaodnoei_gumanitarnoe_pravo Доклад ректора 2021 - уменьшенный размер (2)
Доклад ректора 2021 - уменьшенный размер (2) Преподобный Сергий Радонежский
Преподобный Сергий Радонежский 20180103_bashkirskie_muzykalnye_instrumenty
20180103_bashkirskie_muzykalnye_instrumenty Презентация
Презентация Игра Всезнайки
Игра Всезнайки Смысл жизни
Смысл жизни Текущий ремонт подъездов
Текущий ремонт подъездов Технология заготовительного производства
Технология заготовительного производства Группа Звездочка
Группа Звездочка Примеры современных зданий
Примеры современных зданий 제3과 일상생활. Корейский язык
제3과 일상생활. Корейский язык Схема включения асинхронного двигателя с короткозамкнутым ротором с нереверсивным включением
Схема включения асинхронного двигателя с короткозамкнутым ротором с нереверсивным включением 2011 - год лесов (ООН)
2011 - год лесов (ООН) S7 Airlines является участником глобального авиационного альянса oneworld
S7 Airlines является участником глобального авиационного альянса oneworld Свайные работы. Изготовление свай
Свайные работы. Изготовление свай история зоологии
история зоологии Hidden Images
Hidden Images Презентация бережливого проекта Оптимизация процесса Выдачи справки об обучении
Презентация бережливого проекта Оптимизация процесса Выдачи справки об обучении Городской конкурсе экологических презентаций Мой дом-планета Земля номинация Мой эксперимент
Городской конкурсе экологических презентаций Мой дом-планета Земля номинация Мой эксперимент