- Face presentation

Содержание
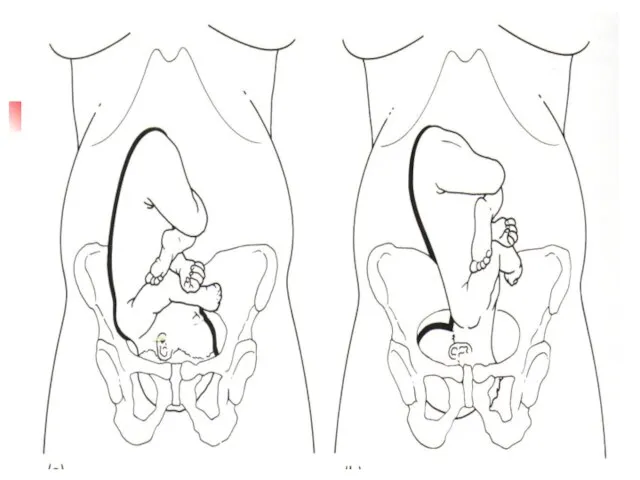
- 2. Definition Head hyper extended, with face as presenting part
- 3. Epidemiology Incidence: 0.1 to 0.2% of singleton deliveries
- 4. Pathophysiology Face presentation is an extended attitude Results in largest head diameter: Occipitomental Increases diameter 3
- 6. Causes Polyhydramnios Multiple pregnancy Multiparity,lax uterus Contracted pelvis
- 7. Cont. Anencephaly Loops of cord around the neck Tumours in front of neck, cystic hygroma, goitre
- 8. Diagnosis During pregnancy High head Head protuberance on the same side as the back USG In
- 10. Labour in face presentation Prolonged labour Early ROM Perineal & vaginal tears May end in obstructed
- 11. Management Do not attempt to convert face presentation to vertex Never apply vacuum extractor to face
- 12. Management No active intervention Wait for the spontaneous rotation and delivery Epidural analgesia If prolonged second
- 13. Cont. If persistant mentotransverse: rotation manually or with Kielland forceps In persistant mentoposterior: C.Section
- 14. Brow Presentation
- 15. Epidemiology Incidence: 0.02% of singleton deliveries Brow is an area between the orbital ridges and anterior
- 18. Diagnosis Never made during pregnancy In labour High head Frontal suture & anterior fontanelle on one
- 19. Pathophysiology Results in largest head diameter: Occipitomental (mentovertical )13.5cms
- 20. Management Cesarean section required in most cases Brow presentation rarely can deliver vaginally unless: spontaneously converts
- 22. Скачать презентацию
Definition
Head hyper extended, with face as presenting part
Definition
Head hyper extended, with face as presenting part
Epidemiology
Incidence: 0.1 to 0.2% of singleton deliveries
Epidemiology
Incidence: 0.1 to 0.2% of singleton deliveries
Pathophysiology
Face presentation is an extended attitude
Results in largest head diameter:
Pathophysiology
Face presentation is an extended attitude
Results in largest head diameter:
Causes
Polyhydramnios
Multiple pregnancy
Multiparity,lax uterus
Contracted pelvis
Causes
Polyhydramnios
Multiple pregnancy
Multiparity,lax uterus
Contracted pelvis
Cont.
Anencephaly
Loops of cord around the neck
Tumours in front of neck, cystic
Cont.
Anencephaly
Loops of cord around the neck
Tumours in front of neck, cystic
Diagnosis
During pregnancy
High head
Head protuberance on the same side as the
Diagnosis
During pregnancy
High head
Head protuberance on the same side as the
Labour in face presentation
Prolonged labour
Early ROM
Perineal & vaginal tears
May end in
Labour in face presentation
Prolonged labour
Early ROM
Perineal & vaginal tears
May end in
Management
Do not attempt to convert face presentation to vertex
Never apply
Management
Do not attempt to convert face presentation to vertex
Never apply
Management
No active intervention
Wait for the spontaneous rotation and delivery
Epidural analgesia
If prolonged
Management
No active intervention
Wait for the spontaneous rotation and delivery
Epidural analgesia
If prolonged
Cont.
If persistant mentotransverse:
rotation manually or with Kielland forceps
In persistant mentoposterior:
Cont.
If persistant mentotransverse:
rotation manually or with Kielland forceps
In persistant mentoposterior:
Brow Presentation
Brow Presentation
Epidemiology
Incidence: 0.02% of singleton deliveries
Brow is an area between the
Epidemiology
Incidence: 0.02% of singleton deliveries
Brow is an area between the

Diagnosis
Never made during pregnancy
In labour
High head
Frontal suture & anterior fontanelle on
Diagnosis
Never made during pregnancy
In labour
High head
Frontal suture & anterior fontanelle on
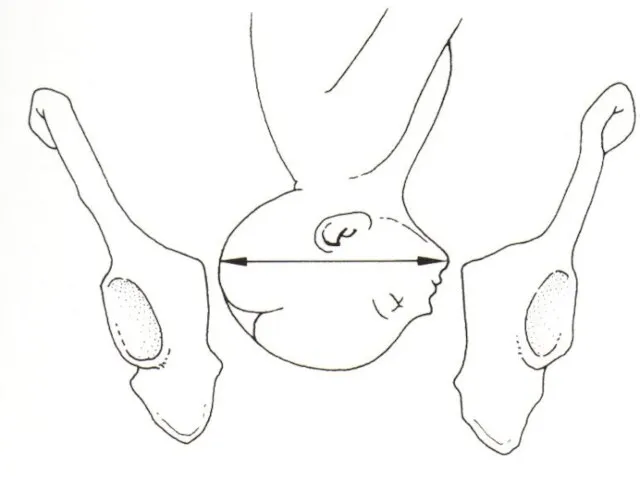
Pathophysiology
Results in largest head diameter: Occipitomental (mentovertical )13.5cms
Pathophysiology
Results in largest head diameter: Occipitomental (mentovertical )13.5cms
Management
Cesarean section required in most cases
Brow presentation rarely can deliver
Management
Cesarean section required in most cases
Brow presentation rarely can deliver
 Такая удивительная жидкость
Такая удивительная жидкость Технические требования, предъявляемые к печатным платам
Технические требования, предъявляемые к печатным платам Пещера Шове
Пещера Шове Развивающие игры для детей и их родителей
Развивающие игры для детей и их родителей Совершенствование работы станции Р при взаимодействии с железнодорожными путями необщего пользования
Совершенствование работы станции Р при взаимодействии с железнодорожными путями необщего пользования Акулы и их разновидности
Акулы и их разновидности Муниципальный центр поддержки ТОС и ОИ: опыт Пермского края
Муниципальный центр поддержки ТОС и ОИ: опыт Пермского края Сказка добрых дел
Сказка добрых дел Повышение эффективности деятельности местных органов власти по территориальному планированию (на примере Управы района Коньково)
Повышение эффективности деятельности местных органов власти по территориальному планированию (на примере Управы района Коньково) СОВЕТЫ
СОВЕТЫ Профессия Учитель
Профессия Учитель Дикие растения нашего края
Дикие растения нашего края объявление
объявление Выбор материалов по их декоративно-художественным свойствам
Выбор материалов по их декоративно-художественным свойствам Сессия БНБ с элементами ТМП по скважине № 58, Волостновского месторождения. ПАО РОСНЕФТЬ
Сессия БНБ с элементами ТМП по скважине № 58, Волостновского месторождения. ПАО РОСНЕФТЬ Агробизнес. Предприятие с большой площадкой для реализации разных сельскохозяйственных проектов
Агробизнес. Предприятие с большой площадкой для реализации разных сельскохозяйственных проектов Отчет по ПДП
Отчет по ПДП Металлы и сплавы
Металлы и сплавы Снятие мерок
Снятие мерок Жизнь в творчестве
Жизнь в творчестве Вечнозаветная псалтирь - святорусская редакция (псалом 61)
Вечнозаветная псалтирь - святорусская редакция (псалом 61) Высотное строительство в условиях плотной городской застройки
Высотное строительство в условиях плотной городской застройки Технологии строительного производства. (Лекция 1)
Технологии строительного производства. (Лекция 1) Результати участi студентiв в Всеукраiнських олiмпiадах
Результати участi студентiв в Всеукраiнських олiмпiадах Земли Уинской очарование
Земли Уинской очарование Теплопередача при установившихся условиях. Сопротивление теплопередаче. Расчёт температуры в ограждении
Теплопередача при установившихся условиях. Сопротивление теплопередаче. Расчёт температуры в ограждении Если любят, то переживают и заботятся. (На примере поэзии Н.С.Гумилёва)
Если любят, то переживают и заботятся. (На примере поэзии Н.С.Гумилёва) 1&1 Versatel
1&1 Versatel