- Acute and Chronic pyelonephritis

Содержание
- 2. Pyelonephritis is a bacterial infection of the kidneys. Pyelonephritis can be acute or chronic, and it
- 3. Incidence: About 3 to 7 out of 10,000 people. Predisposing factors: Obstruction of the urinary tract
- 4. Grading of VUR
- 5. Causative organisms: Gram negative organism: E.coli (common), Proteus mirabilis, Citrobacter, klebsiella, enterobacter, proteus pseudomonas aeruginosa; Gram
- 6. Pathogenesis The urinary tract can be viewed as an anatomic unit united by a continuous column
- 8. Signs and symptoms Signs and symptoms of a kidney infection might include: Fever Chills Back, side
- 9. Acute pyelonephritis Acute pyelonephritis is an exudative purulent localized inflammation of the renal pelvis (collecting system)
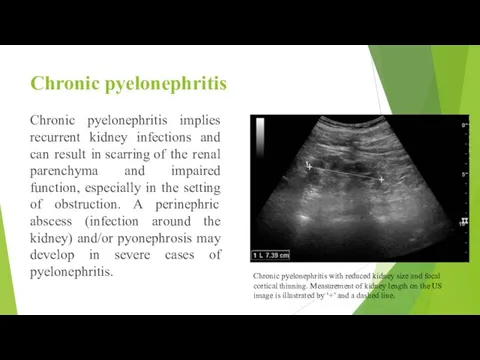
- 10. Chronic pyelonephritis Chronic pyelonephritis implies recurrent kidney infections and can result in scarring of the renal
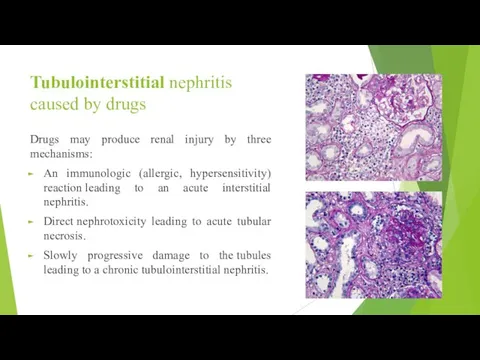
- 12. Tubulointerstitial nephritis caused by drugs Drugs may produce renal injury by three mechanisms: An immunologic (allergic,
- 13. Acute drug induced tubulointerstitial nephritis may be induced by synthetic penicillins (methicillin, ampicillin), sulfonamides, rifampin, diuretics
- 14. Diagnostics Physical examination: - soreness in palpation in the area of the projection of the kidneys;
- 15. Imaging studies If a kidney stone is suspected (e.g. on the basis of characteristic colicky pain
- 16. Purpose of treatment: consists in elimination of infectious and inflammatory process, possible only at restoration of
- 17. Detoxification therapy: plentiful drink; parenteral infusion therapy in the form of solutions of glucose 5-10% and
- 18. The list of basic medicines: 1. Amoxicillin + clavulanic acid, coated tablets 250 mg / 125
- 20. Скачать презентацию
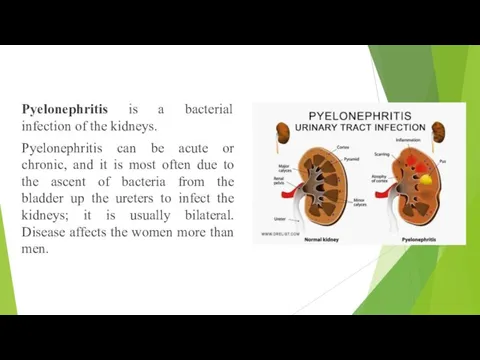
Pyelonephritis is a bacterial infection of the kidneys.
Pyelonephritis can be
Pyelonephritis is a bacterial infection of the kidneys.
Pyelonephritis can be

Incidence:
About 3 to 7 out of 10,000 people.
Predisposing factors:
Obstruction of the
Incidence:
About 3 to 7 out of 10,000 people.
Predisposing factors:
Obstruction of the
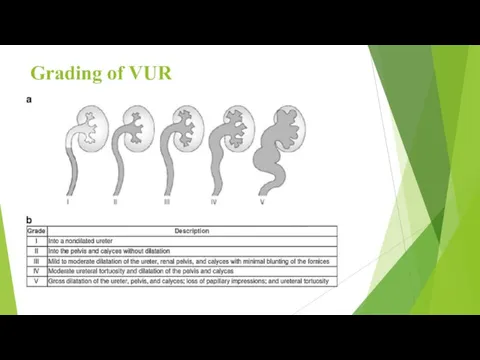
Grading of VUR
Grading of VUR

Causative organisms:
Gram negative organism: E.coli (common), Proteus mirabilis, Citrobacter, klebsiella,
Causative organisms:
Gram negative organism: E.coli (common), Proteus mirabilis, Citrobacter, klebsiella,
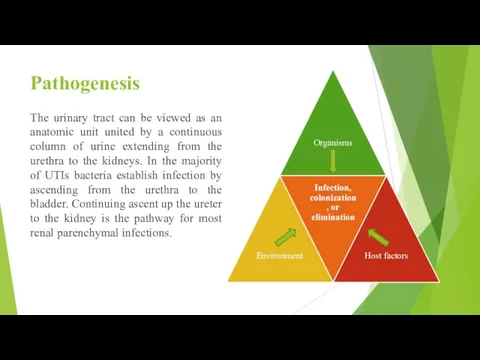
Pathogenesis
The urinary tract can be viewed as an anatomic unit united
Pathogenesis
The urinary tract can be viewed as an anatomic unit united

Signs and symptoms
Signs and symptoms of a kidney infection might include:
Fever
Chills
Back,
Signs and symptoms
Signs and symptoms of a kidney infection might include:
Fever
Chills
Back,
Acute pyelonephritis
Acute pyelonephritis is an exudative purulent localized inflammation of the renal
Acute pyelonephritis
Acute pyelonephritis is an exudative purulent localized inflammation of the renal
Chronic pyelonephritis
Chronic pyelonephritis implies recurrent kidney infections and can result in scarring of
Chronic pyelonephritis
Chronic pyelonephritis implies recurrent kidney infections and can result in scarring of

Tubulointerstitial nephritis caused by drugs
Drugs may produce renal injury by three
Tubulointerstitial nephritis caused by drugs
Drugs may produce renal injury by three
Acute drug induced tubulointerstitial nephritis may be induced by synthetic penicillins
Acute drug induced tubulointerstitial nephritis may be induced by synthetic penicillins

Diagnostics
Physical examination:
- soreness in palpation in the area of the projection
Diagnostics
Physical examination:
- soreness in palpation in the area of the projection

Imaging studies
If a kidney stone is suspected (e.g. on the basis
Imaging studies
If a kidney stone is suspected (e.g. on the basis
Purpose of treatment: consists in elimination of infectious and inflammatory process,
Purpose of treatment: consists in elimination of infectious and inflammatory process,

Detoxification therapy:
plentiful drink;
parenteral infusion therapy in the form of solutions of
Detoxification therapy:
plentiful drink;
parenteral infusion therapy in the form of solutions of
The list of basic medicines:
1. Amoxicillin + clavulanic acid, coated tablets
The list of basic medicines:
1. Amoxicillin + clavulanic acid, coated tablets
 Курс Родить легко
Курс Родить легко Челюстно-лицевая ортопедия. Цель, задачи. Классификация переломов челюстей. Причины и механизм смещения отломков. (Тема 3)
Челюстно-лицевая ортопедия. Цель, задачи. Классификация переломов челюстей. Причины и механизм смещения отломков. (Тема 3) Болезни новорождённых
Болезни новорождённых Суррогатное материнство
Суррогатное материнство Переноска, транспортировка раненых и пострадавших
Переноска, транспортировка раненых и пострадавших Анафилактический шок. Неотложная помощь, интенсивная терапия
Анафилактический шок. Неотложная помощь, интенсивная терапия Системная красная волчанка
Системная красная волчанка Ишемическая болезнь сердца
Ишемическая болезнь сердца Техническое обеспечение современной анестезии
Техническое обеспечение современной анестезии Внебольничная пневмония
Внебольничная пневмония Бронзовая болезнь или Болезнь Аддисона
Бронзовая болезнь или Болезнь Аддисона Информация для медицинских и фармацевтических работников CP-266252
Информация для медицинских и фармацевтических работников CP-266252 Ауыз қуысының шырышты қабатының созылмалы аурулары. Ортопедиялық емдеу тәсілдер
Ауыз қуысының шырышты қабатының созылмалы аурулары. Ортопедиялық емдеу тәсілдер Деформирующий остеоартроз. Причины, симптомы, диагностика и лечение
Деформирующий остеоартроз. Причины, симптомы, диагностика и лечение Гигиена зубов и полости рта. Гигиена тела и кожи
Гигиена зубов и полости рта. Гигиена тела и кожи Психология или психиатрия?
Психология или психиатрия? ЕГИСЗ. Федеральный регистр лиц, больных туберкулезом. Правила учета сведений для расчета основных показателей
ЕГИСЗ. Федеральный регистр лиц, больных туберкулезом. Правила учета сведений для расчета основных показателей Zacházení s lékařskými předpisy
Zacházení s lékařskými předpisy Нормативно-правовые основы профессиональной деятельности младшего медицинского персонала
Нормативно-правовые основы профессиональной деятельности младшего медицинского персонала Типы темперамента
Типы темперамента Лекарственные средства, влияющие на адренергические синапсы
Лекарственные средства, влияющие на адренергические синапсы Гуморальный иммунитет. Иммуноглобулины. Роль антител. Реакция антиген-антитело. (Лекция 12)
Гуморальный иммунитет. Иммуноглобулины. Роль антител. Реакция антиген-антитело. (Лекция 12) Предмет, задачи, особенности анатомии, физиологии, гигиены как науки. Основные закономерности роста и развития организма
Предмет, задачи, особенности анатомии, физиологии, гигиены как науки. Основные закономерности роста и развития организма Взаимосвязь различных факторов риска с патологией ЦНС у детей первого года жизни
Взаимосвязь различных факторов риска с патологией ЦНС у детей первого года жизни Гемотрансфузионный шок
Гемотрансфузионный шок Иммунотропные, противоаллергические и противовоспалительные средства
Иммунотропные, противоаллергические и противовоспалительные средства Нақты қылмыстар себептерінің әлеуметтік және биологиялық факторлары Әлеуметтік және биологиялық факторлардың ара қатынасы
Нақты қылмыстар себептерінің әлеуметтік және биологиялық факторлары Әлеуметтік және биологиялық факторлардың ара қатынасы Педагогічна цінність використання ігор на практичних заняттях
Педагогічна цінність використання ігор на практичних заняттях