- Cardiologic critical care in childhood

Содержание
- 2. Plan of the lecture 1. Acute circulatory dysfunction 2. Syncope 3. Collapse 4. Shock 5. Acute
- 3. Acute circulatory dysfunction Is defined as a pathologic state due to decreased vessel’s smooth muscle tonicity,
- 4. Syncope - Is sudden short-term loss of conscience with muscle tonicity loss due to transient cerebral
- 5. Syncope reasons in children: Vessels neurotic dysregulation : vaso-vagal, orthostatic, sinocarotid, reflectory, hyperventilation syndrome Cardiogenic syncope
- 6. Critical care in syncope Put down in horizontal position with slightly raising legs, loose belts, collar
- 7. Collapse - Life threatening acute vascular insufficiency with acute vessel dystonia, circulatory blood volume decrease, signs
- 8. Reasons of collapse Severe course of acute infectious pathology ( intestine infection, flu, pneumonia, angina, pyelonephritis
- 9. Critical care in collapse Put down to back with throw back head, heat patient, provide air
- 10. SHOCK Acute threatening life pathologic process characterized by progressive tissue perfusion diminishing, subsequent CNS impaired functioning,
- 11. Reasons of shock Decreasing of circulatory volume (hypovolemic shock): due to bleeding, dehydration, burns, etc. Main
- 12. Critical care in shock Put down in horizontal position with slightly raising legs, moisturized oxygen To
- 13. Acute cardiac failure Pathologic condition characterized by cardiac output decreasing due to myocardial pumping function reduction
- 14. Acute cardiac failure (ACF) reasons Shock due to rhythm disorders –bradiarhythmia ( sinus or due to
- 15. ACF reasons: Acute lung and bronchial disorders (pneumonia, atelectasis, hydro- and pneumothorax etc.) Main mechanism of
- 16. ACF clinical presentation: Little cardiac output syndrome (LCOS): arterial hypotonia, and signs of centralized circulation; Congestive
- 17. Acute left ventricular failure Algorithm of critical care Patient position in bed sitting or semisitting Oxygen
- 18. Acute right ventricular failure algorythm of critical care Causative factors eradication (bronchospasm, pneumothorax, foreign body) Oxygen
- 19. Heart rhythm and conductivity disorders Sinus tachy- bradycardia, arrhythmia Sick sinus node Extrasystoles Paroxysmal tachycardia (
- 20. Arrhythmia treatment Pharmacologic medications Reflectory methods Psycho-physical methods Electrical methods Surgical methods
- 21. Antiarrhythmic drugs features Class 1 – membrane stabilizers, block rapid Na channels of cell membrane, retard
- 22. Antiarhythmic drugs features - subclass IВ– medications that shorten repolarization and the whole action potential. Refractory
- 23. Antiarrhythmic drugs features Class II – β-adrenoblockers, limit sympathetic influence on heart. They suppress sinoatrial node
- 24. Sinus tachycardia Clinics. Complaints to heartbeats, heart pain, dyscomfort, HR >10-60% from age norma ECG:shortening or
- 25. Sinus bradycardia Clinics. Weakness,dizziness, head ache, cardiac pains, HR 95-60% from age norma ECG. Intervals РР,
- 26. Sick sinus node syndrome Can be inherited or acquired one ( after myocarditis, cardiomyopathies, amyloidosis, hemochromatosis,,
- 27. Premature contractility Allocation: supraventricular, from AV-node. Left-right-ventricular; functional and organic. Clinics – signs of vegetative dystonia.
- 28. Supraventricular paroxysmal tachycardia HR 180-220 /min (infants – 250-300/min). Heartbeats, unpleasant sensation or heart , epigastrium
- 29. Treatment Semisitting position, respiratory therapy Mechanical stimulation of nervous vagus: Ashner reflex- pressing by 2 fingers
- 30. Treatment IV 0,25% isoptin (verapamil) sol.without dilution for 20-30 sec in dosages: for neonates 0,3-04 ml,
- 31. Ventricular paroxysmal tachycardia (VPT) Abrupt heartbeating attack, dyspnea, cardialgia Condition is severe with progressive worsening, loss
- 32. VPT treatment Lidocain IV injection 1 mg/kg for 5 min. If it’s ineffective repeat injection 0,5
- 33. Atrium fibrillation treatment Isoptin 0,15mg/kg I V slowly diluted with 10-20ml of 5% glucose Propranolol very
- 34. Anoxic spells- Is paroxysmal attack of dyspnea in child with congenital heart disease with cyanosismore frequently
- 35. Clinical presentation Sudden onset Irritability, moaning, crying with dyspnea and cyanosis Sitting posture-squatting or lateral decubitus
- 36. Emergency care To calm child, put into knee-chest position, give humidified oxygen Morohine or promedol 0,1
- 38. Скачать презентацию
Plan of the lecture
1. Acute circulatory dysfunction
2. Syncope
3. Collapse
4. Shock
Plan of the lecture
1. Acute circulatory dysfunction
2. Syncope
3. Collapse
4. Shock
Acute circulatory dysfunction
Is defined as a pathologic state due to
Acute circulatory dysfunction
Is defined as a pathologic state due to
Syncope -
Is sudden short-term loss of conscience with muscle tonicity
Syncope -
Is sudden short-term loss of conscience with muscle tonicity
Syncope reasons in children:
Vessels neurotic dysregulation : vaso-vagal, orthostatic, sinocarotid, reflectory,
Syncope reasons in children:
Vessels neurotic dysregulation : vaso-vagal, orthostatic, sinocarotid, reflectory,
Critical care in syncope
Put down in horizontal position with slightly raising
Critical care in syncope
Put down in horizontal position with slightly raising
Collapse -
Life threatening acute vascular insufficiency with acute vessel dystonia, circulatory
Collapse -
Life threatening acute vascular insufficiency with acute vessel dystonia, circulatory
Reasons of collapse
Severe course of acute infectious pathology ( intestine infection,
Reasons of collapse
Severe course of acute infectious pathology ( intestine infection,
Critical care in collapse
Put down to back with throw back head,
Critical care in collapse
Put down to back with throw back head,
SHOCK
Acute threatening life pathologic process characterized by progressive tissue perfusion
SHOCK
Acute threatening life pathologic process characterized by progressive tissue perfusion
Reasons of shock
Decreasing of circulatory volume (hypovolemic shock): due to bleeding,
Reasons of shock
Decreasing of circulatory volume (hypovolemic shock): due to bleeding,
Critical care in shock
Put down in horizontal position with slightly raising
Critical care in shock
Put down in horizontal position with slightly raising
Acute cardiac failure
Pathologic condition characterized by cardiac output decreasing due to
Acute cardiac failure
Pathologic condition characterized by cardiac output decreasing due to
Acute cardiac failure (ACF) reasons
Shock due to rhythm disorders –bradiarhythmia (
Acute cardiac failure (ACF) reasons
Shock due to rhythm disorders –bradiarhythmia (
ACF reasons:
Acute lung and bronchial disorders (pneumonia, atelectasis, hydro- and pneumothorax
ACF reasons:
Acute lung and bronchial disorders (pneumonia, atelectasis, hydro- and pneumothorax
ACF clinical presentation:
Little cardiac output syndrome (LCOS): arterial hypotonia, and signs
ACF clinical presentation:
Little cardiac output syndrome (LCOS): arterial hypotonia, and signs
Acute left ventricular failure
Algorithm of critical care
Patient position in bed
Acute left ventricular failure
Algorithm of critical care
Patient position in bed
Acute right ventricular failure
algorythm of critical care
Causative factors eradication (bronchospasm, pneumothorax,
Acute right ventricular failure
algorythm of critical care
Causative factors eradication (bronchospasm, pneumothorax,
Heart rhythm and conductivity disorders
Sinus tachy- bradycardia, arrhythmia
Sick sinus node
Extrasystoles
Paroxysmal tachycardia
Heart rhythm and conductivity disorders
Sinus tachy- bradycardia, arrhythmia
Sick sinus node
Extrasystoles
Paroxysmal tachycardia
Arrhythmia treatment
Pharmacologic medications
Reflectory methods
Psycho-physical methods
Electrical methods
Surgical methods
Arrhythmia treatment
Pharmacologic medications
Reflectory methods
Psycho-physical methods
Electrical methods
Surgical methods
Antiarrhythmic drugs features
Class 1 – membrane stabilizers, block rapid Na channels
Antiarrhythmic drugs features
Class 1 – membrane stabilizers, block rapid Na channels
Antiarhythmic drugs features
- subclass IВ– medications that shorten repolarization and the
Antiarhythmic drugs features
- subclass IВ– medications that shorten repolarization and the
Antiarrhythmic drugs features
Class II – β-adrenoblockers, limit sympathetic influence on heart.
Antiarrhythmic drugs features
Class II – β-adrenoblockers, limit sympathetic influence on heart.
Sinus tachycardia
Clinics. Complaints to heartbeats, heart pain, dyscomfort, HR >10-60% from
Sinus tachycardia
Clinics. Complaints to heartbeats, heart pain, dyscomfort, HR >10-60% from
Sinus bradycardia
Clinics. Weakness,dizziness, head ache, cardiac pains, HR 95-60% from age
Sinus bradycardia
Clinics. Weakness,dizziness, head ache, cardiac pains, HR 95-60% from age
Sick sinus node syndrome
Can be inherited or acquired one ( after
Sick sinus node syndrome
Can be inherited or acquired one ( after
Premature contractility
Allocation: supraventricular, from AV-node. Left-right-ventricular; functional and organic.
Clinics – signs
Premature contractility
Allocation: supraventricular, from AV-node. Left-right-ventricular; functional and organic.
Clinics – signs
Supraventricular paroxysmal tachycardia
HR 180-220 /min (infants – 250-300/min).
Heartbeats, unpleasant sensation
Supraventricular paroxysmal tachycardia
HR 180-220 /min (infants – 250-300/min).
Heartbeats, unpleasant sensation
Treatment
Semisitting position, respiratory therapy
Mechanical stimulation of nervous vagus: Ashner reflex- pressing
Treatment
Semisitting position, respiratory therapy
Mechanical stimulation of nervous vagus: Ashner reflex- pressing
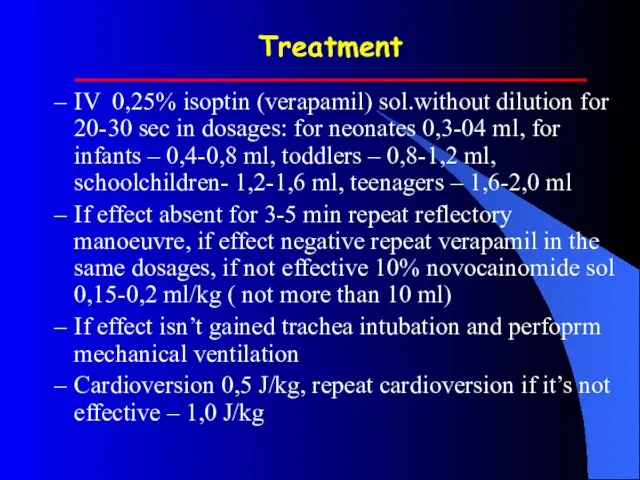
Treatment
IV 0,25% isoptin (verapamil) sol.without dilution for 20-30 sec in dosages:
Treatment
IV 0,25% isoptin (verapamil) sol.without dilution for 20-30 sec in dosages:
Ventricular paroxysmal tachycardia (VPT)
Abrupt heartbeating attack, dyspnea, cardialgia
Condition is severe with
Ventricular paroxysmal tachycardia (VPT)
Abrupt heartbeating attack, dyspnea, cardialgia
Condition is severe with
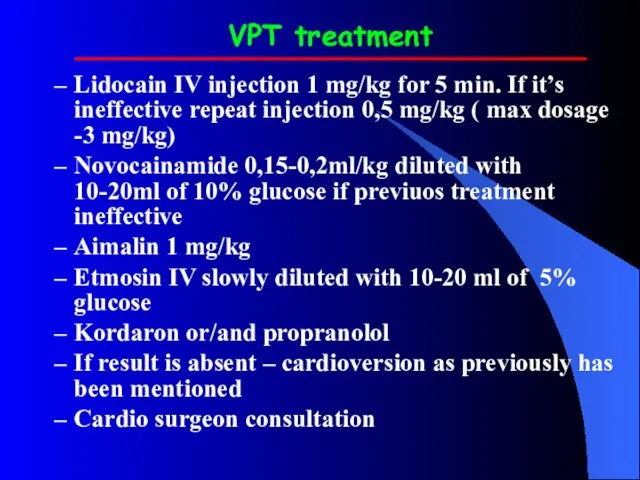
VPT treatment
Lidocain IV injection 1 mg/kg for 5 min. If it’s
VPT treatment
Lidocain IV injection 1 mg/kg for 5 min. If it’s
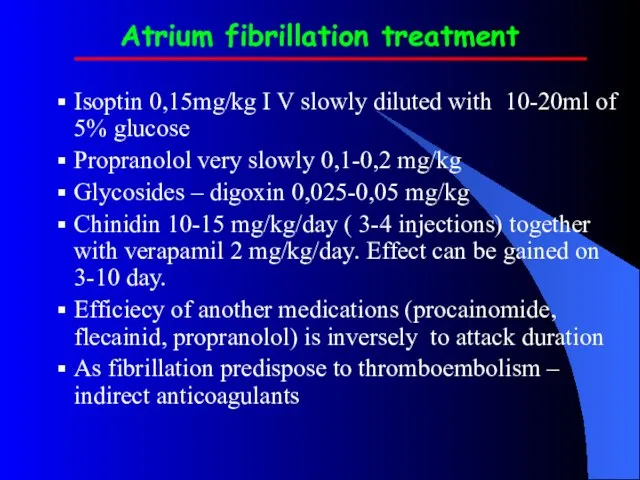
Atrium fibrillation treatment
Isoptin 0,15mg/kg I V slowly diluted with 10-20ml of
Atrium fibrillation treatment
Isoptin 0,15mg/kg I V slowly diluted with 10-20ml of
Anoxic spells-
Is paroxysmal attack of dyspnea in child with congenital
Anoxic spells-
Is paroxysmal attack of dyspnea in child with congenital
Clinical presentation
Sudden onset
Irritability, moaning, crying with dyspnea and cyanosis
Sitting posture-squatting or
Clinical presentation
Sudden onset
Irritability, moaning, crying with dyspnea and cyanosis
Sitting posture-squatting or
Emergency care
To calm child, put into knee-chest position, give humidified oxygen
Morohine
Emergency care
To calm child, put into knee-chest position, give humidified oxygen
Morohine
 Санитарно-гигиенические требования к организации питания в организациях для детей-сирот
Санитарно-гигиенические требования к организации питания в организациях для детей-сирот Основные варианты задержки психического развития
Основные варианты задержки психического развития Функции участкового педиатра
Функции участкового педиатра Типичная форма (ангинозный)
Типичная форма (ангинозный) Тест по теме: Эндокринная система
Тест по теме: Эндокринная система Тест на определение темперамента
Тест на определение темперамента Информация по компании Интертич для ТОО Болашак Атырау
Информация по компании Интертич для ТОО Болашак Атырау Психология семейных отношений
Психология семейных отношений Практика графологического исследования
Практика графологического исследования Основные факторы, влияющие на уровень материнской смертности
Основные факторы, влияющие на уровень материнской смертности Алгоритм при обнаружении очаговых образований в легких
Алгоритм при обнаружении очаговых образований в легких Crimea state medical academy named
Crimea state medical academy named Патологическая физиология пищеварения
Патологическая физиология пищеварения Мед.катастроф Лекция №8 СДС
Мед.катастроф Лекция №8 СДС Презентация по медицине Сахарный диабет»
Презентация по медицине Сахарный диабет»  Витамин K
Витамин K Urok_zdorovya_v_3V_red
Urok_zdorovya_v_3V_red Оценка тяжести состояния пациентов с острым панкреатитом
Оценка тяжести состояния пациентов с острым панкреатитом Болезни губ и языка у детей
Болезни губ и языка у детей Введение в неонатологию. Организация медицинской помощи новорожденным детям
Введение в неонатологию. Организация медицинской помощи новорожденным детям Патофизиология клетки. Гипоксия
Патофизиология клетки. Гипоксия Гастростомия
Гастростомия Трихофития
Трихофития Ультразвуковая ангиология. Некоторые особенности диагностики и лечения ХНМК
Ультразвуковая ангиология. Некоторые особенности диагностики и лечения ХНМК Акушерский перитонит
Акушерский перитонит Лекция №4. Патология реактивности нарушения иммунной системы, аллергия
Лекция №4. Патология реактивности нарушения иммунной системы, аллергия Проблема создания единых представлений об условиях труда
Проблема создания единых представлений об условиях труда Перитонит
Перитонит