- Influenza

Содержание
- 2. INFLUENZA is an acute infectious disease which occurs in epidemics and is caused by a virus,
- 3. Influenza takes the leading position in the human pathology. The main thing is that besides relatively
- 4. History The first documented pandemic of influenza (retrospectively - influenza type A virus) occurred in 1889.
- 5. History In 1890 M.I. Afanasiev and in 1892 the German doctor R. Pfeiffer isolated small bacilli
- 6. Etiology The family Orthomyxoviridae comprises: influenza A, B, C. Influenza A viruses can infect a variety
- 7. Etiology The virions are spherical 80-120 nm in diameter. They have a nucleocapsid comprising RNA, RNA-polymerase.
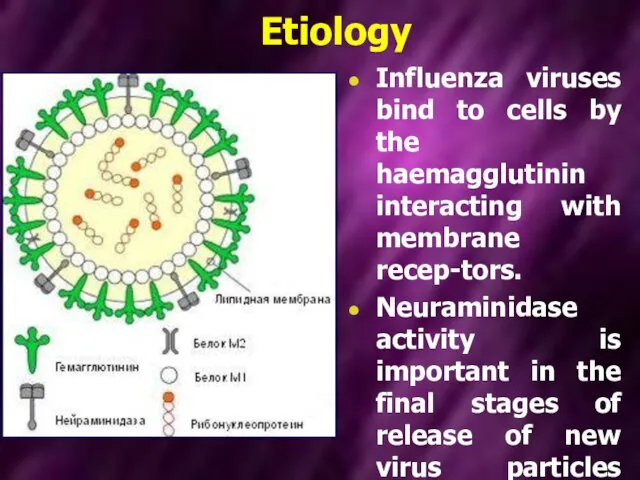
- 8. Etiology Influenza viruses bind to cells by the haemagglutinin interacting with membrane recep-tors. Neuraminidase activity is
- 9. One of the most prominent features of the influenza viruses is their ability to change antigenically
- 10. Nomenclature. The World Health Organization system of nomenclature includes: the host of origin; geographical origin, strain
- 11. A / Scotland / 42/89 (H3N2)
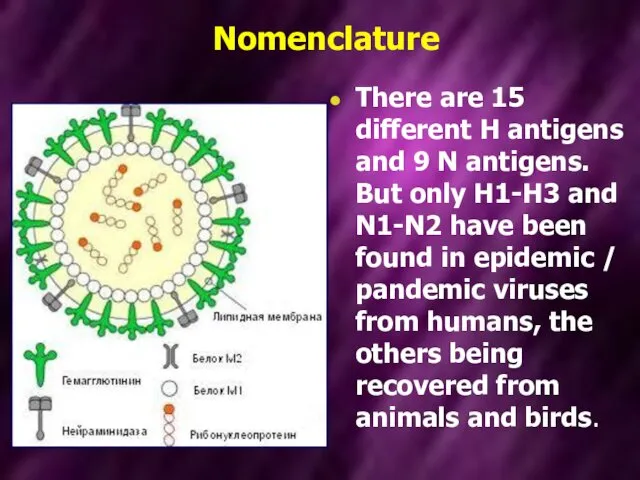
- 12. Nomenclature There are 15 different H antigens and 9 N antigens. But only H1-H3 and N1-N2
- 13. Nomenclature However, in 1997 an outbreak, with high case mortality, occurred in humans in Hong Kong;
- 14. Physical characteristics The influenza viruses withstands slow drying at room temperature on articles such as blankets
- 15. Physical characteristics Exposure to heat for 30 min at 56°C is sufficient to inactivate most strains.
- 16. Epidemiology Epidemics, which must have been caused by influenza viruses, have been described for over 2000
- 17. Epidemiology In 1933 Christopher Andrewes and others isolated influenza A virus. Continued isolation studies and analysis
- 18. Epidemiology The mayor pandemics are associated with antigenic shifts – when the viral H or N,
- 19. Epidemiology Until 1977, when H1N1 reappeared, it was the rule that when a “new” virus appeared,
- 20. Epidemiology Influenza B viruses do not undergo antigenic shift as there is no animal reservoir and,
- 21. Epidemiology A sick person is the only source of the disease. The virus quickly multiplies in
- 22. Epidemiology The influenza infection is spread with the help of small particle aerosol dispersion. The mechanism
- 23. Epidemiology The viable influenza virus can live and be infectious in the air for 2 -3
- 24. Epidemiology The speed of influenza spreading depends on the speed of people moving on the territory.
- 25. Pathogenesis Pathogencity of influenza viruses is multifactirial and may involve viral, host and environment factors. After
- 26. Pathogenesis The virus multiplication cycle lasts 7-10 hours. Every virion which penetrated a cell gives birth
- 27. Pathogenesis The cell, in which virus reproduces, produces and secretes interferon. This interferon gets into the
- 28. Pathogenesis The cells affected by a virus are rejected and the products of their decomposition are
- 29. Pathogenesis When the process spreads in the lung tissue, there are signs of general edema with
- 30. Pathogenesis Under these conditions the influenza virus easily penetrates the blood and virusemia develops. However, virusemia
- 31. Pathogenesis Besides, it is a fact that even in the mild cases of the disease there
- 32. Pathogenesis The earliest response is the synthesis and release of interferons from the infected cells: these
- 33. Clinical features. In classic influenza A: The incubation period is short, 2 days, but it may
- 34. Clinical features The incubation period at influenza in short: from several hours to 2 days. Its
- 35. Clinical features The first symptoms are chilliness, high temperature, headaches, dizziness, a syncope condition, malaise, pains
- 36. Clinical features The main physical finding is pyrexia, which rises rapidly to a peak of 38-41°C
- 37. Clinical features Adynamia, malaise can be considerable and are manifested since the first day of the
- 38. Clinical features of influenza
- 39. Clinical features Many patients have both upper and lower respiratory tract infection, ofen with a troublesome,
- 40. Clinical features The affection of the upper respiratory tracts is accompanied with hyperemia and swelling of
- 41. Clinical features During fauces examination hyperemia of the tonsils, uvula palatina and posterior wall of the
- 42. Clinical features Diverse changes in the cardiovascular system have been described. The pulse very often corresponds
- 43. Clinical features There are various affections of the nervous system during the influenza infection. The functional
- 44. Clinical features. In classic influenza B: Symptoms closely resemble those associated with influenza A infection, consisting
- 45. Clinical features. In classic influenza C: Clinically, influenza C causes an afebrile upper respiratory tract infection
- 46. Complications of influenza: Primary influenza pneumonia may occur, especially in young adults during an outbreak, and
- 47. The changes in the hemogram are manifested as leukopenia or normocytosis. If there are no complications
- 48. Laboratory diagnosis The virusological methods of diagnostics are used to isolate and identify the influenza virus.
- 49. Laboratory diagnosis The serological diagnostics of influenza ensures an accurate determination of etiology by revealing the
- 50. Laboratory diagnosis The immunefluorescent method is recommended as one of the reliable means of quick deciphering
- 51. immune fluorescent method The essence of the immune fluorescent method is in specific reactions of antigen-antibody
- 52. Treatment During the epidemics 10-25% of the adult population fall ill with influenza, 1-2% of them
- 53. Treatment Even in case of a moderate severe influenza form together with an unfavorable premorbid condition
- 54. Treatment Oral amantadine hydrochloride was introduced in the early 1980s, followed later by a derivative, rimantadine.
- 55. Treatment The usage of rimantadinum is quite effective especially during the first days of the disease.
- 56. "Rimantadinum" appoints under the circuit: 1-st day - on 100 mg (2 tablets) 3 times; 2-nd
- 57. More recently neuraminidase inhibitor Oseltamivir. Oseltamivir uses influenza A, B and H5N1 infections. It can reduce
- 58. There is fast elimination of intoxication and noticeable improvement of the patients’ general condition observed when
- 59. Such preparations as 5-20% albumin solution, native or dried plasma 150-200 ml, haemodesum 200 ml, rheopolyglucinum
- 61. Скачать презентацию
INFLUENZA
is an acute infectious disease which occurs in epidemics and
INFLUENZA
is an acute infectious disease which occurs in epidemics and
Influenza takes the leading position in the human pathology.
The
Influenza takes the leading position in the human pathology.
The
History
The first documented pandemic of influenza (retrospectively - influenza type A
History
The first documented pandemic of influenza (retrospectively - influenza type A
History
In 1890 M.I. Afanasiev and in 1892 the German doctor R.
History
In 1890 M.I. Afanasiev and in 1892 the German doctor R.
Etiology
The family Orthomyxoviridae comprises: influenza A, B, C.
Influenza A
Etiology
The family Orthomyxoviridae comprises: influenza A, B, C.
Influenza A
Etiology
The virions are spherical 80-120 nm in diameter. They have a
Etiology
The virions are spherical 80-120 nm in diameter. They have a
Etiology
Influenza viruses bind to cells by the haemagglutinin interacting with membrane
Etiology
Influenza viruses bind to cells by the haemagglutinin interacting with membrane
One of the most prominent features of the influenza viruses is
One of the most prominent features of the influenza viruses is
Nomenclature. The World Health Organization system of nomenclature includes:
the host
Nomenclature. The World Health Organization system of nomenclature includes:
the host

A / Scotland / 42/89 (H3N2)
A / Scotland / 42/89 (H3N2)
Nomenclature
There are 15 different H antigens and 9 N antigens. But
Nomenclature
There are 15 different H antigens and 9 N antigens. But
Nomenclature
However, in 1997 an outbreak, with high case mortality, occurred in
Nomenclature
However, in 1997 an outbreak, with high case mortality, occurred in
Physical characteristics
The influenza viruses withstands slow drying at room temperature on
Physical characteristics
The influenza viruses withstands slow drying at room temperature on
Physical characteristics
Exposure to heat for 30 min at 56°C is sufficient
Physical characteristics
Exposure to heat for 30 min at 56°C is sufficient
Epidemiology
Epidemics, which must have been caused by influenza viruses, have been
Epidemiology
Epidemics, which must have been caused by influenza viruses, have been
Epidemiology
In 1933 Christopher Andrewes and others isolated influenza A virus. Continued
Epidemiology
In 1933 Christopher Andrewes and others isolated influenza A virus. Continued
Epidemiology
The mayor pandemics are associated with antigenic shifts – when the
Epidemiology
The mayor pandemics are associated with antigenic shifts – when the
Epidemiology
Until 1977, when H1N1 reappeared, it was the rule that when
Epidemiology
Until 1977, when H1N1 reappeared, it was the rule that when
Epidemiology
Influenza B viruses do not undergo antigenic shift as there is
Epidemiology
Influenza B viruses do not undergo antigenic shift as there is
Epidemiology
A sick person is the only source of the disease. The
Epidemiology
A sick person is the only source of the disease. The
Epidemiology
The influenza infection is spread with the help of small particle
Epidemiology
The influenza infection is spread with the help of small particle
Epidemiology
The viable influenza virus can live and be infectious in the
Epidemiology
The viable influenza virus can live and be infectious in the
Epidemiology
The speed of influenza spreading depends on the speed of people
Epidemiology
The speed of influenza spreading depends on the speed of people
Pathogenesis
Pathogencity of influenza viruses is multifactirial and may involve viral, host
Pathogenesis
Pathogencity of influenza viruses is multifactirial and may involve viral, host
Pathogenesis
The virus multiplication cycle lasts 7-10 hours. Every virion which penetrated
Pathogenesis
The virus multiplication cycle lasts 7-10 hours. Every virion which penetrated
Pathogenesis
The cell, in which virus reproduces, produces and secretes interferon. This
Pathogenesis
The cell, in which virus reproduces, produces and secretes interferon. This
Pathogenesis
The cells affected by a virus are rejected and the products
Pathogenesis
The cells affected by a virus are rejected and the products
Pathogenesis
When the process spreads in the lung tissue, there are signs
Pathogenesis
When the process spreads in the lung tissue, there are signs
Pathogenesis
Under these conditions the influenza virus easily penetrates the blood and
Pathogenesis
Under these conditions the influenza virus easily penetrates the blood and
Pathogenesis
Besides, it is a fact that even in the mild cases
Pathogenesis
Besides, it is a fact that even in the mild cases
Pathogenesis
The earliest response is the synthesis and release of interferons from
Pathogenesis
The earliest response is the synthesis and release of interferons from
Clinical features.
In classic influenza A:
The incubation period is short, 2 days,
Clinical features.
In classic influenza A:
The incubation period is short, 2 days,
Clinical features
The incubation period at influenza in short: from several hours
Clinical features
The incubation period at influenza in short: from several hours
Clinical features
The first symptoms are chilliness, high temperature, headaches, dizziness, a
Clinical features
The first symptoms are chilliness, high temperature, headaches, dizziness, a
Clinical features
The main physical finding is pyrexia, which rises rapidly to
Clinical features
The main physical finding is pyrexia, which rises rapidly to
Clinical features
Adynamia, malaise can be considerable and are manifested since the
Clinical features
Adynamia, malaise can be considerable and are manifested since the

Clinical features of influenza
Clinical features of influenza
Clinical features
Many patients have both upper and lower respiratory tract infection,
Clinical features
Many patients have both upper and lower respiratory tract infection,
Clinical features
The affection of the upper respiratory tracts is accompanied with
Clinical features
The affection of the upper respiratory tracts is accompanied with
Clinical features
During fauces examination hyperemia of the tonsils, uvula palatina and
Clinical features
During fauces examination hyperemia of the tonsils, uvula palatina and
Clinical features
Diverse changes in the cardiovascular system have been described. The
Clinical features
Diverse changes in the cardiovascular system have been described. The
Clinical features
There are various affections of the nervous system during the
Clinical features
There are various affections of the nervous system during the
Clinical features.
In classic influenza B:
Symptoms closely resemble those associated with influenza
Clinical features.
In classic influenza B:
Symptoms closely resemble those associated with influenza
Clinical features.
In classic influenza C:
Clinically, influenza C causes an afebrile
Clinical features.
In classic influenza C:
Clinically, influenza C causes an afebrile
Complications of influenza:
Primary influenza pneumonia may occur, especially in young adults
Complications of influenza:
Primary influenza pneumonia may occur, especially in young adults
The changes in the hemogram
are manifested as leukopenia or normocytosis.
If
The changes in the hemogram
are manifested as leukopenia or normocytosis.
If
Laboratory diagnosis
The virusological methods of diagnostics are used to isolate
Laboratory diagnosis
The virusological methods of diagnostics are used to isolate
Laboratory diagnosis
The serological diagnostics of influenza ensures an accurate determination of
Laboratory diagnosis
The serological diagnostics of influenza ensures an accurate determination of
Laboratory diagnosis
The immunefluorescent method is recommended as one of the reliable
Laboratory diagnosis
The immunefluorescent method is recommended as one of the reliable
immune fluorescent method
The essence of the immune fluorescent method is in
immune fluorescent method
The essence of the immune fluorescent method is in
Treatment
During the epidemics 10-25% of the adult population fall ill
Treatment
During the epidemics 10-25% of the adult population fall ill
Treatment
Even in case of a moderate severe influenza form together with
Treatment
Even in case of a moderate severe influenza form together with
Treatment
Oral amantadine hydrochloride was introduced in the early 1980s, followed later
Treatment
Oral amantadine hydrochloride was introduced in the early 1980s, followed later
Treatment
The usage of rimantadinum is quite effective especially during the first
Treatment
The usage of rimantadinum is quite effective especially during the first
"Rimantadinum" appoints under the circuit:
1-st day - on 100 mg (2
"Rimantadinum" appoints under the circuit:
1-st day - on 100 mg (2
More recently neuraminidase inhibitor Oseltamivir. Oseltamivir uses influenza A, B and
More recently neuraminidase inhibitor Oseltamivir. Oseltamivir uses influenza A, B and
There is fast elimination of intoxication and noticeable improvement of the
There is fast elimination of intoxication and noticeable improvement of the
Such preparations as 5-20% albumin solution, native or dried plasma 150-200
Such preparations as 5-20% albumin solution, native or dried plasma 150-200
 Антисептика: механическая, физическая, химическая, биологическая
Антисептика: механическая, физическая, химическая, биологическая Мікози (грибкові ураження шкіри)
Мікози (грибкові ураження шкіри) Schistosomiasis (bilharziasis)
Schistosomiasis (bilharziasis) Аллергодиагностика in vitro
Аллергодиагностика in vitro Психология личности
Психология личности Как получить/продлить инвалидность
Как получить/продлить инвалидность Бас-сүйек ми жарақаты және күйіктер
Бас-сүйек ми жарақаты және күйіктер Преждевременная отслойка нормально расположенной плаценты
Преждевременная отслойка нормально расположенной плаценты Каротидный синус
Каротидный синус ҚТМ мүшелерінің жасқа сай анатомиялық ерекшеліктері
ҚТМ мүшелерінің жасқа сай анатомиялық ерекшеліктері Криоконсервировация и хранение половых клеток, тканей репродуктивных органов и эмбрионов
Криоконсервировация и хранение половых клеток, тканей репродуктивных органов и эмбрионов Захворювання новонароджених дітей. Захворювання шкіри, пупкової ранки, сепсис
Захворювання новонароджених дітей. Захворювання шкіри, пупкової ранки, сепсис Наследственные свойства крови
Наследственные свойства крови Болезни костно-мышечной системы и соединительной ткани
Болезни костно-мышечной системы и соединительной ткани Возрастная психология и педагогика. От нуля до 3-х лет. Занятие 3
Возрастная психология и педагогика. От нуля до 3-х лет. Занятие 3 Физиологический эффект спортивного массажа
Физиологический эффект спортивного массажа Средства, влияющие на систему крови
Средства, влияющие на систему крови Сахарный диабет. Практическое занятие
Сахарный диабет. Практическое занятие Соул коллаж (Soul Collage), автор Сиена Фрост
Соул коллаж (Soul Collage), автор Сиена Фрост Легочное сердце
Легочное сердце Ожоги и ожоговая болезнь
Ожоги и ожоговая болезнь Болезнь Крона
Болезнь Крона Когнитивті қабілеттің дамуы
Когнитивті қабілеттің дамуы Сравнительный анализ основных характеристик препаратов: Простатилен, Витапрост, Простакор, Уропрост, Сампрост
Сравнительный анализ основных характеристик препаратов: Простатилен, Витапрост, Простакор, Уропрост, Сампрост Жеке микроэлементтердің алмасуы
Жеке микроэлементтердің алмасуы Основы массажа
Основы массажа Клеточный метаболизм при раке
Клеточный метаболизм при раке Жүрек гликозидтері (грекше glykys – тəтті) - өсімдік текті азотсыз қосылыстар, декомпенсацияланған миокардқа кардиотоникалық
Жүрек гликозидтері (грекше glykys – тəтті) - өсімдік текті азотсыз қосылыстар, декомпенсацияланған миокардқа кардиотоникалық