- Laboratory tests in Rheumatology

Содержание
- 2. Introduction In rheumatic disease lab test contribute to diagnosis Laboratory investigation should be guided by clinical
- 3. Utility of Lab Tests Aims of lab test: 1. Identification of pathological process in the body
- 4. Diagnostic vs. Evaluative Tests Need to determine which test is appropriate Diagnostic tests accurately distinguish a
- 5. Blood Panel - Hemoglobin Anemia of chronic disease – usually normocytic and normochromic, but sometimes hypochromic
- 6. Blood panel - WBC White blood cells – neutrophils, lymphocytes, eosinophils: Neutrophils are acute phase reactants
- 7. Platelets Thrombocytosis can accompany active phases of autoimmune diseases – RA (APR) Thrombocytopenia – can be
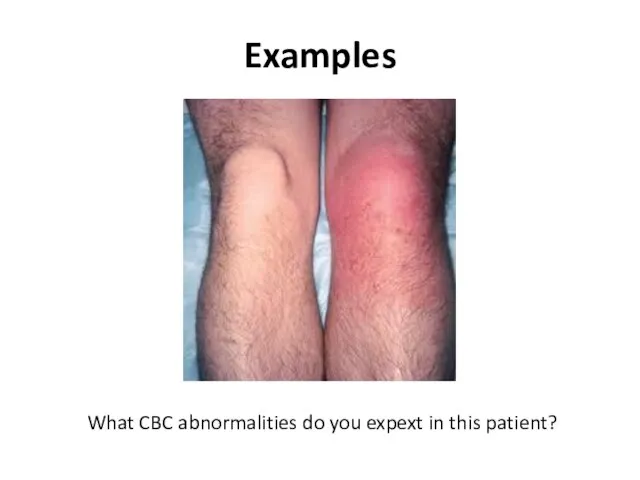
- 8. Examples What CBC abnormalities do you expext in this patient?
- 9. Biochemical testing- liver Synthetic activity (albumin, coagulation factors, Glucose, Bil) Liver enzymes – hepatocellular, cholestatic Should
- 10. Kidney function tests Connective tissue diseases and systemic vasculitides are frequently associated with kidney involvement –
- 11. Uric acid Commonly included in the workup of patients with arthritis Elevated in 90% of patients
- 12. Acute-phase reactants Are not specific for rheumatic disorders AP response occurs in a variety of inflammatory
- 13. Acute phase reactants Produced by hepatocytes upon stimulation by cytokines (IL-1, IL -6, TNF – tumor
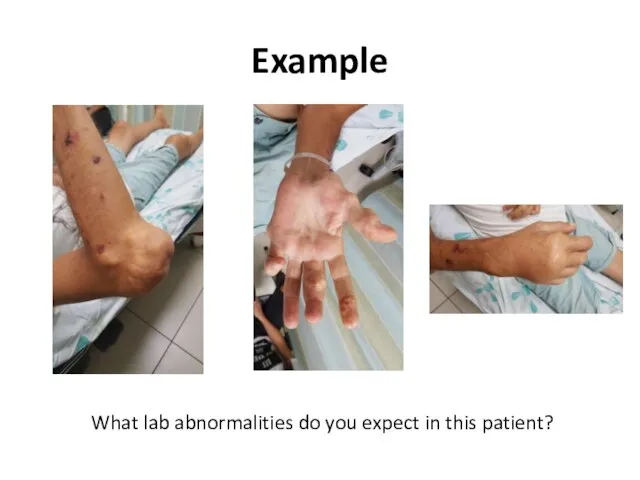
- 14. Example What lab abnormalities do you expect in this patient?
- 15. Example What lab abnormalities do you expect in this patient?
- 16. Serologic testing Testing for autoantibodies is frequently used in the diagnoses of rheumatic conditions and sometimes
- 17. Rheumatoid Factor Autoantibodies directed against Fc– chains of IgG molecules Laboratories test only for IgM RF
- 18. Rheumatoid Factor Not specific for Rheumatoid Arthritis The main indication for RF testing – suspicion for
- 19. Antibodies to citrullinated protein and peptide ACPA- antigens Citrullination of proteins (arginine – citrullin) occurs as
- 20. Anti-nuclear Antibodies (ANA) Immunoglobulins directed against structures within the cell ( i.e. DNA, ribonuclear proteins, histones,
- 21. ANA ANAs do not correlate with disease activity Consider using as a screening test in only
- 22. ANA Low titres ( Infections (EBV, CMV, Hepatitis B, bacterial endocarditis, HIV) Drugs (hydralazine, INH, dilantin,
- 23. ANA detection and measurement IIF - the indirect immunofluorescence test is the most widely used assay
- 24. ANA patterns In the homogeneous staining pattern, the entire nucleus is diffusely stained. EX: Antibodies to
- 25. homogenous nucleolar speckled cenromere
- 26. ELISA method Solid phase assays - enzyme-linked immunoabsorbant assays (ELISA) A panel of purified native or
- 27. Advantages and Disadvantages The major advantage of indirect immunofluorescence is the large number of autoantibodies that
- 28. Advantages and Disadvantages The number of autoantigens that are included in solid phase (ELIZA) assays is
- 29. Anti-dsDNA antibodies Antibodies that target DNA Produce homogenous pattern in ANA IIF Positive result for anti-dsDNA
- 30. Anti-histone antibodies Found in 95% of patients with drug-induced lupus syndrome Seen with: Procainamide Quinidine Hydralazine
- 31. Anti-Sm and anti-RNP antibodies “extractable” (ENA) Produce coarse speckled pattern in ANA IIF The nucleoli are
- 32. Anti-Sm and anti-RNP antibodies “extractable” (ENA) Anti-Sm antibodies generally remain positive, even when a patient has
- 33. Anti-Ro (SS-A) and anti-La (SS-B) antibodies (ENAs) Two sets of names assigned by two different groups;
- 34. Anti-Ro (SS-A) and anti-La (SS-B) antibodies Produce fine speckled pattern in ANA IIF with staining of
- 35. Anticentomere and anti-SCL-70 Anticentromere antibodies (ACA) produce a typical pattern in ANA IIF by staining the
- 36. Antineutrophil cytoplasmic antibodies - ANCA Subgroup of neutrophil specific antibodies Commonly directed to myeloperoxidase (MPO) -
- 37. ANCA c-ANCA is seen in 90% of GPA (Wegener’s granulomatosis) p-ANCA is associated with microscopic polyangiitis,
- 38. Complement The most frequent clinical parameters used for judging complement activation – C3, C4 C3, C4
- 39. Antiphospholipid antibodies (APLA) Anti-cardiolipin antibodies (ELIZA) IgG – better related to procoagulant activity compared to IgM/IgA
- 40. Examples 24y woman presents with weakness, nausea, ptechia and echymozes
- 41. Laboratory analyses
- 42. Laboratory analyses
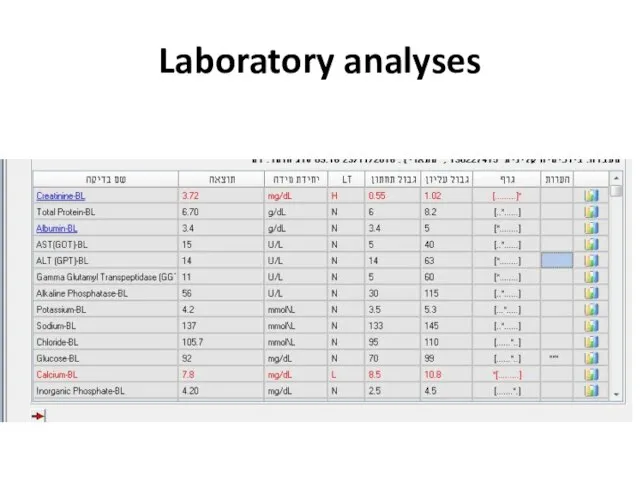
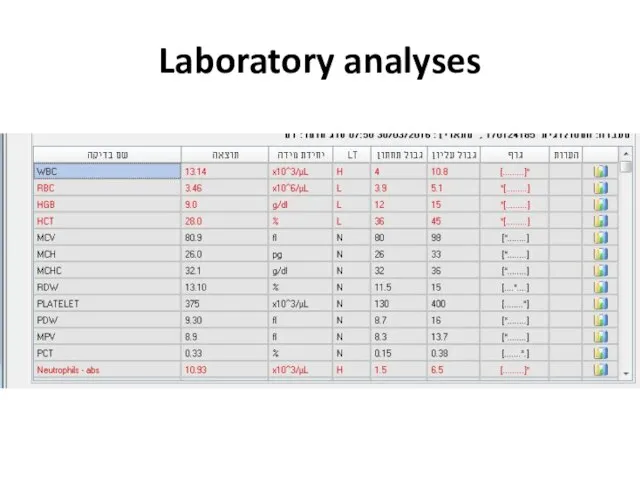
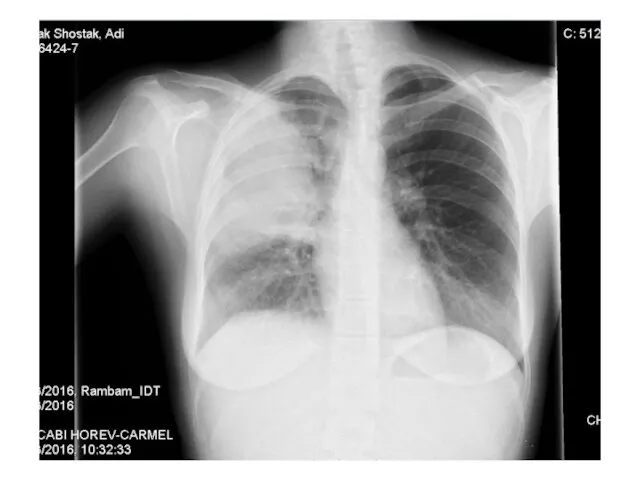
- 45. Examples 28y old woman presents with cough, fever, dyspnea, fatigue
- 46. Laboratory analyses
- 47. Laboratory analyses
- 49. Laboratory analyses
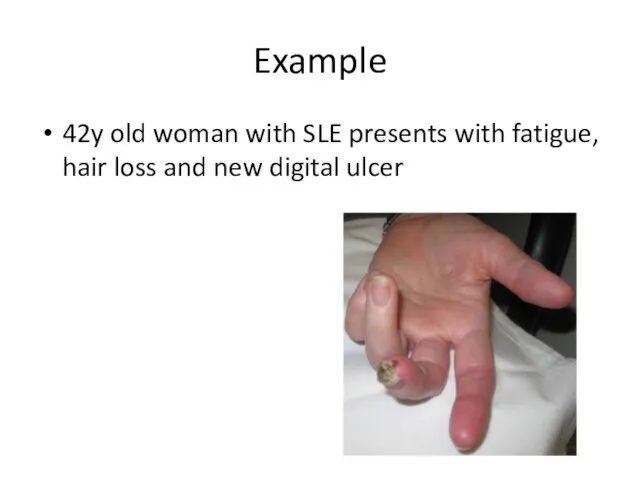
- 50. Example 42y old woman with SLE presents with fatigue, hair loss and new digital ulcer
- 51. Examples
- 53. Examples
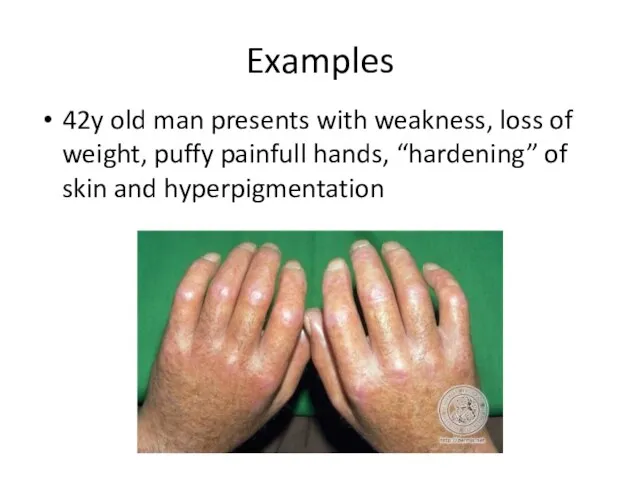
- 54. Examples 42y old man presents with weakness, loss of weight, puffy painfull hands, “hardening” of skin
- 56. Скачать презентацию
Introduction
In rheumatic disease lab test contribute to diagnosis
Laboratory investigation should be
Introduction
In rheumatic disease lab test contribute to diagnosis
Laboratory investigation should be
Utility of Lab Tests
Aims of lab test:
1. Identification of pathological process
Utility of Lab Tests
Aims of lab test:
1. Identification of pathological process
Diagnostic vs. Evaluative Tests
Need to determine which test is appropriate
Diagnostic tests
Diagnostic vs. Evaluative Tests
Need to determine which test is appropriate
Diagnostic tests
Blood Panel - Hemoglobin
Anemia of chronic disease – usually normocytic and
Blood Panel - Hemoglobin
Anemia of chronic disease – usually normocytic and
Blood panel - WBC
White blood cells – neutrophils, lymphocytes, eosinophils:
Neutrophils are
Blood panel - WBC
White blood cells – neutrophils, lymphocytes, eosinophils:
Neutrophils are
Platelets
Thrombocytosis can accompany active phases of autoimmune diseases – RA (APR)
Thrombocytopenia
Platelets
Thrombocytosis can accompany active phases of autoimmune diseases – RA (APR)
Thrombocytopenia
Examples
What CBC abnormalities do you expext in this patient?
Examples
What CBC abnormalities do you expext in this patient?
Biochemical testing- liver
Synthetic activity (albumin, coagulation factors, Glucose, Bil)
Liver
Biochemical testing- liver
Synthetic activity (albumin, coagulation factors, Glucose, Bil)
Liver
Kidney function tests
Connective tissue diseases and systemic vasculitides are frequently associated
Kidney function tests
Connective tissue diseases and systemic vasculitides are frequently associated
Uric acid
Commonly included in the workup of patients with arthritis
Elevated in
Uric acid
Commonly included in the workup of patients with arthritis
Elevated in
Acute-phase reactants
Are not specific for rheumatic disorders
AP response occurs in
Acute-phase reactants
Are not specific for rheumatic disorders
AP response occurs in
Acute phase reactants
Produced by hepatocytes upon stimulation by cytokines (IL-1, IL
Acute phase reactants
Produced by hepatocytes upon stimulation by cytokines (IL-1, IL
Example
What lab abnormalities do you expect in this patient?
Example
What lab abnormalities do you expect in this patient?
Example
What lab abnormalities do you expect in this patient?
Example
What lab abnormalities do you expect in this patient?
Serologic testing
Testing for autoantibodies is frequently used in the diagnoses of
Serologic testing
Testing for autoantibodies is frequently used in the diagnoses of
Rheumatoid Factor
Autoantibodies directed against Fc– chains of IgG molecules
Laboratories test only
Rheumatoid Factor
Autoantibodies directed against Fc– chains of IgG molecules
Laboratories test only
Rheumatoid Factor
Not specific for Rheumatoid Arthritis
The main indication for RF testing
Rheumatoid Factor
Not specific for Rheumatoid Arthritis
The main indication for RF testing
Antibodies to citrullinated protein and peptide ACPA- antigens
Citrullination of proteins (arginine
Antibodies to citrullinated protein and peptide ACPA- antigens
Citrullination of proteins (arginine
Anti-nuclear Antibodies (ANA)
Immunoglobulins directed against structures within the cell ( i.e.
Anti-nuclear Antibodies (ANA)
Immunoglobulins directed against structures within the cell ( i.e.
ANA
ANAs do not correlate with disease activity
Consider using as a screening
ANA
ANAs do not correlate with disease activity
Consider using as a screening
ANA
Low titres (<= 1:160) found in:
Infections (EBV, CMV, Hepatitis B,
ANA
Low titres (<= 1:160) found in:
Infections (EBV, CMV, Hepatitis B,
ANA detection and measurement
IIF - the indirect immunofluorescence test is the
ANA detection and measurement
IIF - the indirect immunofluorescence test is the
ANA patterns
In the homogeneous staining pattern, the entire nucleus is diffusely
ANA patterns
In the homogeneous staining pattern, the entire nucleus is diffusely
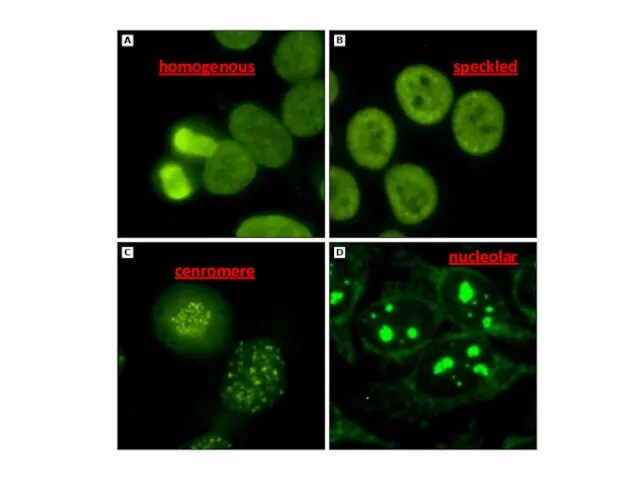
homogenous
nucleolar
speckled
cenromere
homogenous
nucleolar
speckled
cenromere
ELISA method
Solid phase assays - enzyme-linked immunoabsorbant assays (ELISA)
A panel of
ELISA method
Solid phase assays - enzyme-linked immunoabsorbant assays (ELISA)
A panel of
Advantages and Disadvantages
The major advantage of indirect immunofluorescence is the large
Advantages and Disadvantages
The major advantage of indirect immunofluorescence is the large
Advantages and Disadvantages
The number of autoantigens that are included in solid
Advantages and Disadvantages
The number of autoantigens that are included in solid
Anti-dsDNA antibodies
Antibodies that target DNA
Produce homogenous pattern in ANA IIF
Positive
Anti-dsDNA antibodies
Antibodies that target DNA
Produce homogenous pattern in ANA IIF
Positive
Anti-histone antibodies
Found in 95% of patients with drug-induced lupus syndrome
Seen with:
Procainamide
Quinidine
Hydralazine
Phenytoin
Anti-histone antibodies
Found in 95% of patients with drug-induced lupus syndrome
Seen with:
Procainamide
Quinidine
Hydralazine
Phenytoin
Anti-Sm and anti-RNP antibodies
“extractable” (ENA)
Produce coarse speckled pattern in ANA IIF
The
Anti-Sm and anti-RNP antibodies
“extractable” (ENA)
Produce coarse speckled pattern in ANA IIF
The
Anti-Sm and anti-RNP antibodies
“extractable” (ENA)
Anti-Sm antibodies generally remain positive, even when
Anti-Sm and anti-RNP antibodies
“extractable” (ENA)
Anti-Sm antibodies generally remain positive, even when
Anti-Ro (SS-A) and anti-La (SS-B) antibodies
(ENAs)
Two sets of names assigned by
Anti-Ro (SS-A) and anti-La (SS-B) antibodies
(ENAs)
Two sets of names assigned by
Anti-Ro (SS-A) and anti-La (SS-B) antibodies
Produce fine speckled pattern in ANA
Anti-Ro (SS-A) and anti-La (SS-B) antibodies
Produce fine speckled pattern in ANA
Anticentomere and anti-SCL-70
Anticentromere antibodies (ACA) produce a typical pattern in ANA
Anticentomere and anti-SCL-70
Anticentromere antibodies (ACA) produce a typical pattern in ANA
Antineutrophil cytoplasmic antibodies - ANCA
Subgroup of neutrophil specific antibodies
Commonly directed to
Antineutrophil cytoplasmic antibodies - ANCA
Subgroup of neutrophil specific antibodies
Commonly directed to
ANCA
c-ANCA is seen in 90% of GPA (Wegener’s granulomatosis)
p-ANCA is associated
ANCA
c-ANCA is seen in 90% of GPA (Wegener’s granulomatosis)
p-ANCA is associated
Complement
The most frequent clinical parameters used for judging complement activation –
Complement
The most frequent clinical parameters used for judging complement activation –
Antiphospholipid antibodies (APLA)
Anti-cardiolipin antibodies (ELIZA)
IgG – better related to procoagulant activity
Antiphospholipid antibodies (APLA)
Anti-cardiolipin antibodies (ELIZA)
IgG – better related to procoagulant activity
Examples
24y woman presents with weakness, nausea, ptechia and echymozes
Examples
24y woman presents with weakness, nausea, ptechia and echymozes
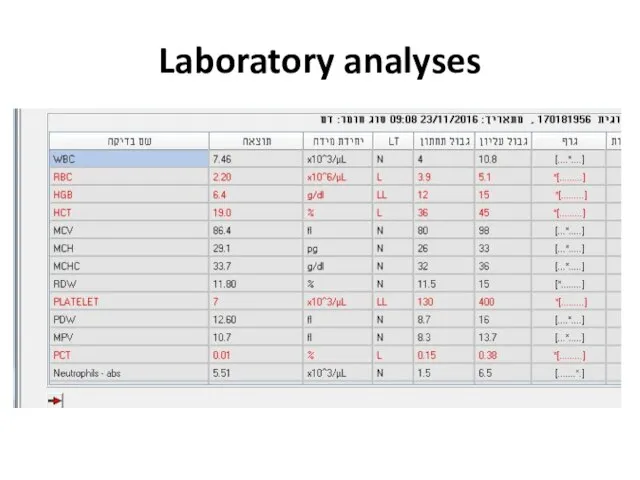
Laboratory analyses
Laboratory analyses
Laboratory analyses
Laboratory analyses



Examples
28y old woman presents with cough, fever, dyspnea, fatigue
Examples
28y old woman presents with cough, fever, dyspnea, fatigue
Laboratory analyses
Laboratory analyses

Laboratory analyses
Laboratory analyses
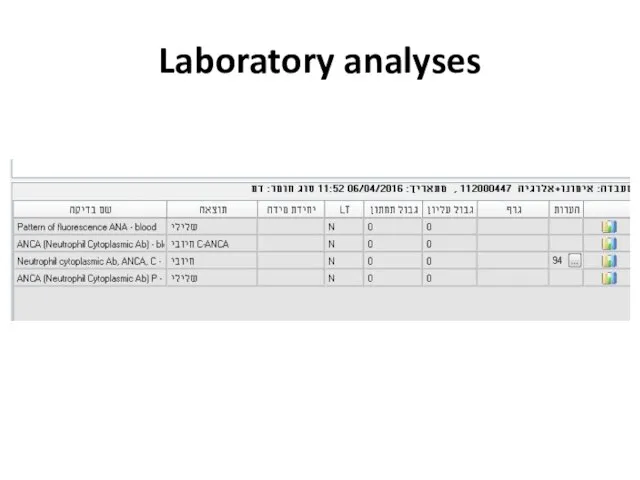
Laboratory analyses
Laboratory analyses
Example
42y old woman with SLE presents with fatigue, hair loss and
Example
42y old woman with SLE presents with fatigue, hair loss and
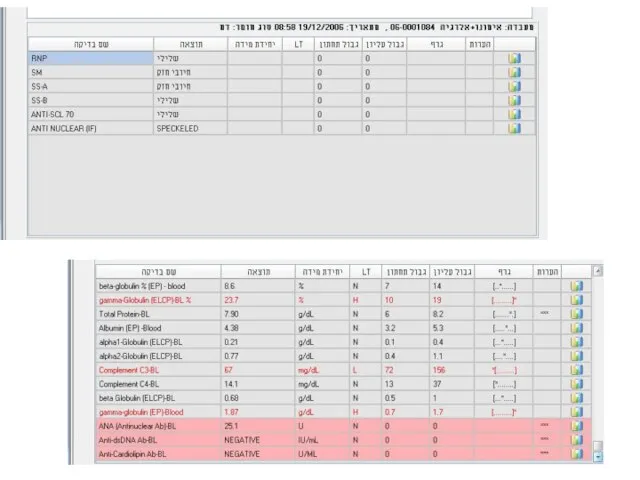
Examples
Examples

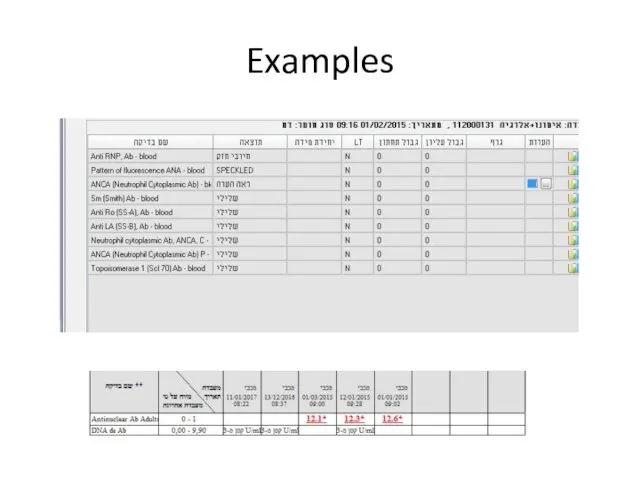
Examples
Examples
Examples
42y old man presents with weakness, loss of weight, puffy painfull
Examples
42y old man presents with weakness, loss of weight, puffy painfull
 Кожа. Заболевания кожи
Кожа. Заболевания кожи Хирургическая операция
Хирургическая операция Профилактика психических заболеваний
Профилактика психических заболеваний Неклеточные формы жизни. Вирусы
Неклеточные формы жизни. Вирусы Острая кишечная непроходимость
Острая кишечная непроходимость Асқорыту мүшелерінің рентгенанатомиясы
Асқорыту мүшелерінің рентгенанатомиясы Компьютерные полиграфные системы. Психологические и психофизиологические основы применения полиграфных устройств
Компьютерные полиграфные системы. Психологические и психофизиологические основы применения полиграфных устройств Инородные тела верхних дыхательных путей
Инородные тела верхних дыхательных путей Колесо баланса
Колесо баланса Рахит. Основные причины дефицита фосфатов и солей кальция у детей раннего возраста
Рахит. Основные причины дефицита фосфатов и солей кальция у детей раннего возраста Предпринимательская и приносящая доходы деятельность. Правовые и организационные основы оказания платных медицинских услуг
Предпринимательская и приносящая доходы деятельность. Правовые и организационные основы оказания платных медицинских услуг Профилактика постинъекционных осложнений
Профилактика постинъекционных осложнений Воспаление. Причины воспаления
Воспаление. Причины воспаления Аутоиммунные заболевания печени
Аутоиммунные заболевания печени Травматология детского возраста
Травматология детского возраста Анаэробная инфекция
Анаэробная инфекция Симпатическая гиперактивация при артериальной гипертнезии. Роль бета-блокаторов в лечении пациентов с артериальной гипертензий
Симпатическая гиперактивация при артериальной гипертнезии. Роль бета-блокаторов в лечении пациентов с артериальной гипертензий Орган зрения
Орган зрения Вещества, влияющие на центральную нервную систему
Вещества, влияющие на центральную нервную систему Коарктация аорты
Коарктация аорты Диагностика расслаивающей аневризмы аорты
Диагностика расслаивающей аневризмы аорты Кинетопластиды. Види паразитичных джгутиконосцев
Кинетопластиды. Види паразитичных джгутиконосцев Очищение от паразитов. Действенные методы
Очищение от паразитов. Действенные методы Оспа обезьян
Оспа обезьян Остеосинтез - операции на костях
Остеосинтез - операции на костях Сердечно-сосудистая система. Органы кроветворения и иммунной системы
Сердечно-сосудистая система. Органы кроветворения и иммунной системы Бүйрек және зәр биохимиясы
Бүйрек және зәр биохимиясы Талмажәне талма кезінде алғашқы көмек
Талмажәне талма кезінде алғашқы көмек