- Arterial hypertension

Содержание
- 2. Definition Arterial hypertension (WHO, 1999) is a constantly increased systolic (≥140 mmHg) and/or diastolic BP (≥90
- 3. Definition Hypertension is defined as values ≥140 mmHg SBP and/or ≥90 mmHg DBP, based on the
- 4. Why do we take care of arterial hypertension? “Silent killer of XXI century” Major cardiovascular risk
- 5. What do we call “target organs”? CNS (Strokes 7-10 times more frequent!) Heart (MI 4-5 times
- 6. Hypertension in the world 33% of the population in USA, 43-44% in Russia,more than 41,5 million.
- 7. Prevalence of hypertension Overall the prevalence of hypertension appears to be around 30–45% of the general
- 8. Report of World Health Organization In 2020 AD, 2.6 million Indians are predicted to die due
- 9. Hypertension in Nigeria Prevalence of hypertension -28.7%. Hypertension prevalence was comparable in men and women (29.9%
- 10. Hypertension: Predisposing factors Age > 60 years Sex (men and postmenopausal women) Family history of cardiovascular
- 11. Structure of the diagnosis of AH Primary (essential hypertension) or secondary (symptomatic) Degree (according to BP
- 12. Structure of AH 94-95% constitute 5-6% - secondary AH 4-5% Renal parenchimal diseases 1-2% others primary
- 13. Classification of AH according to the BP level (WHO, 1999) WHO-ISH Guidelines Subcommittee J Hypertens 1999;
- 14. Classification of AH according to stages Stage I: no objective signs of target organs affection Stage
- 15. Assessment of total cardiovascular risk The concept is based on the fact that only a small
- 16. Assessment of total cardiovascular risk Estimation of total CV risk is easy in particular subgroups of
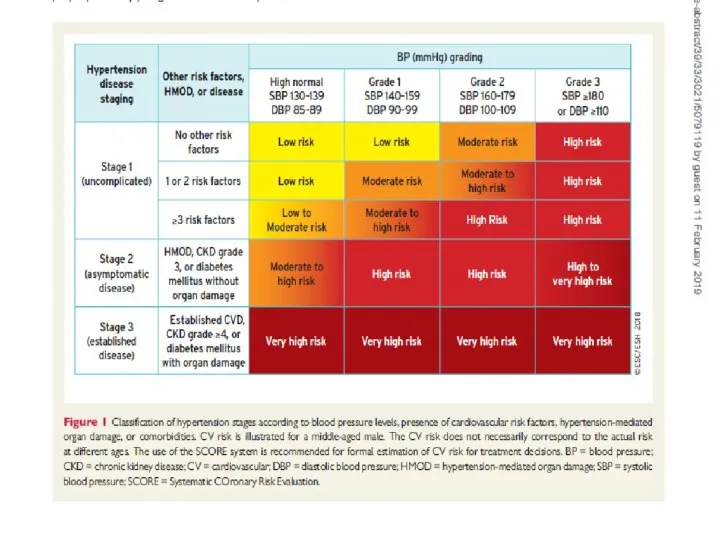
- 17. Assessment of total cardiovascular risk The classification in low, moderate, high and very high risk is
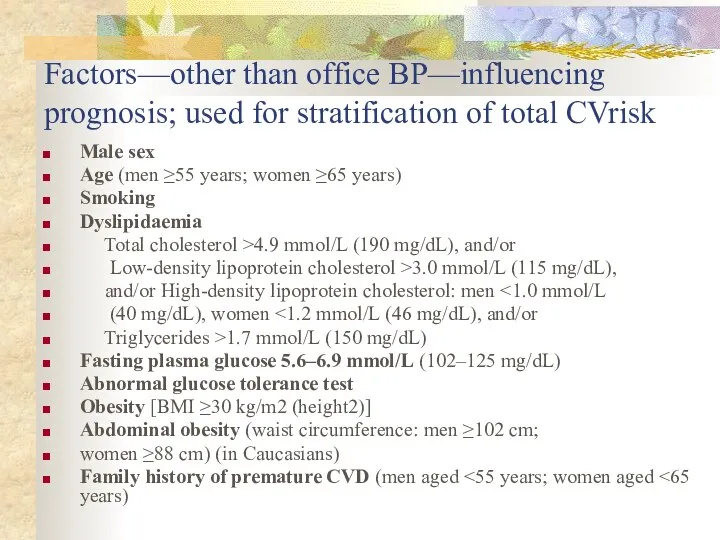
- 18. Factors—other than office BP—influencing prognosis; used for stratification of total CVrisk Male sex Age (men ≥55
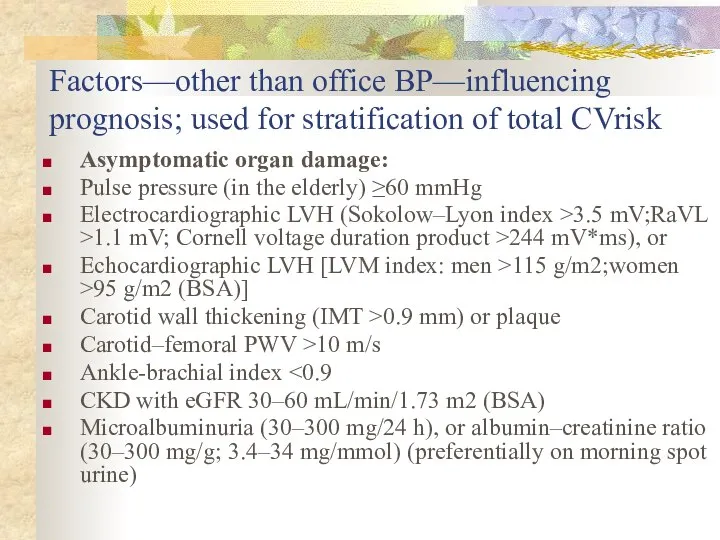
- 19. Factors—other than office BP—influencing prognosis; used for stratification of total CVrisk Asymptomatic organ damage: Pulse pressure
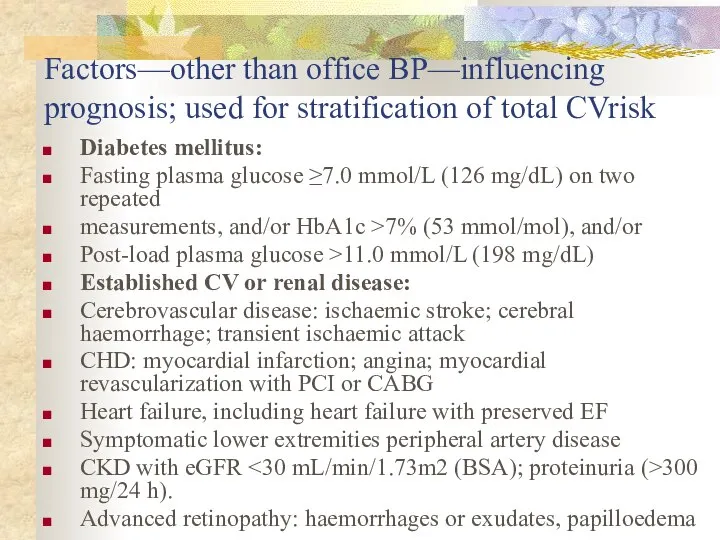
- 20. Factors—other than office BP—influencing prognosis; used for stratification of total CVrisk Diabetes mellitus: Fasting plasma glucose
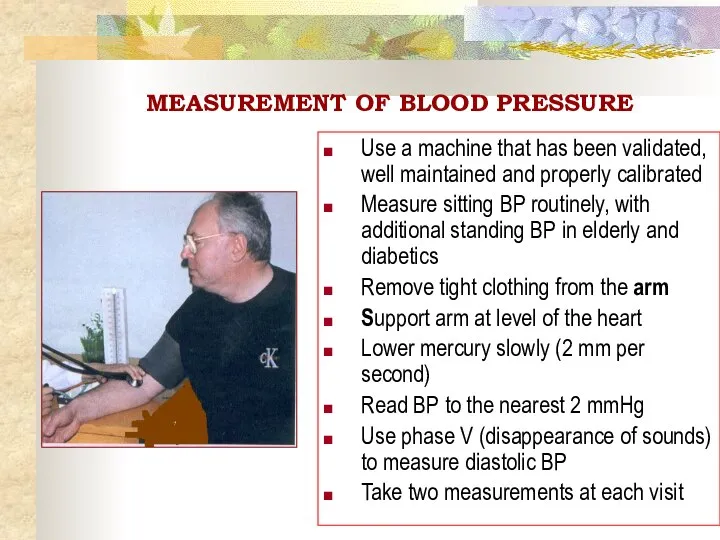
- 22. MEASUREMENT OF BLOOD PRESSURE Use a machine that has been validated, well maintained and properly calibrated
- 23. Types of measurement: Office BP Home BP Daily monitoring of BP!!!
- 24. ‘White coat‘ hypertension? Up to 13-15% of apparent hypertension in the clinic may 'normal BP' when
- 25. Classification of secondary AH 1. Renal: Renal parenchymal, Renovascular Anephric 2. Endocrinological: Cushing`s syndrome and disease
- 26. Classification of secondary AH 3. Neurogenic: - In increased intracranial pressure (tumors, inflammatory diseases) Hypotalamic syndrome
- 27. Classification of secondary AH 5. Pharmacological (iatrogenic) Corticosteroids Excessive thyroxine Oral contraceptives, containing oestrogens Sympatomimetics (for
- 28. Routine tests • Haemoglobin and/or haematocrit. • Fasting plasma glucose. • Serum total cholesterol, low-density lipoprotein
- 29. Obligatory investigation to detect the secondary hypertension • Chest radiograph: to detect cardiomegaly, heart failure, coarctation
- 30. Life style modifications Lose weight, if overweight Limit alcohol intake Increase physical activity Reduce salt intake
- 31. Principles of treatment 1. Etiological: elimination of causes 2. Non-pharmacological treatment: weight reduction, stop alcogol and
- 32. Treatment strategies 1) Treatment is permanent and continuous 2) Begin treatment with a minimal dose and
- 33. Angiotensin II inhibitors ACE-inhibitors Diuretics Ca-blockers or + Top-priority combinations of AHT
- 34. Renal parenchymal AH: chronic glomerulonephritis, pyelonephritis, polycystic renal disease, diabetic nephropathy, congenital diseases of kidneys, vasculitis
- 35. Diagnostics of renal parenchymal diseases urinary syndrome (proteinuria, leucocyturia, hematuria, cylindruria, bacteriuria), testing of the renal
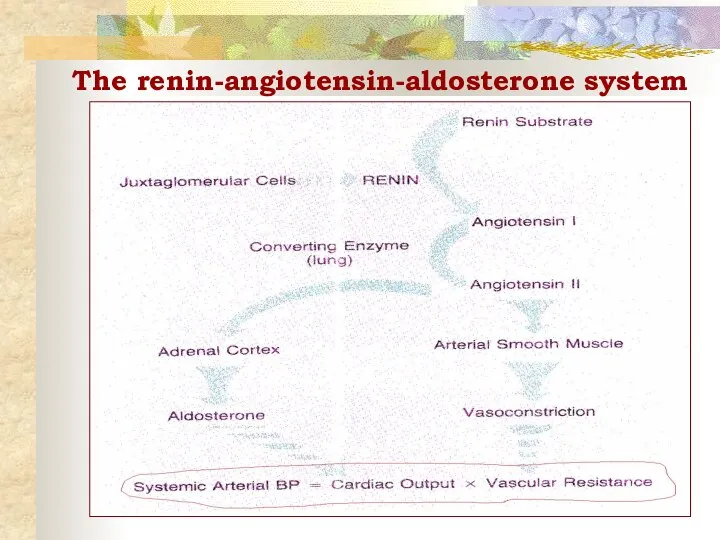
- 36. The renin-angiotensin-aldosterone system
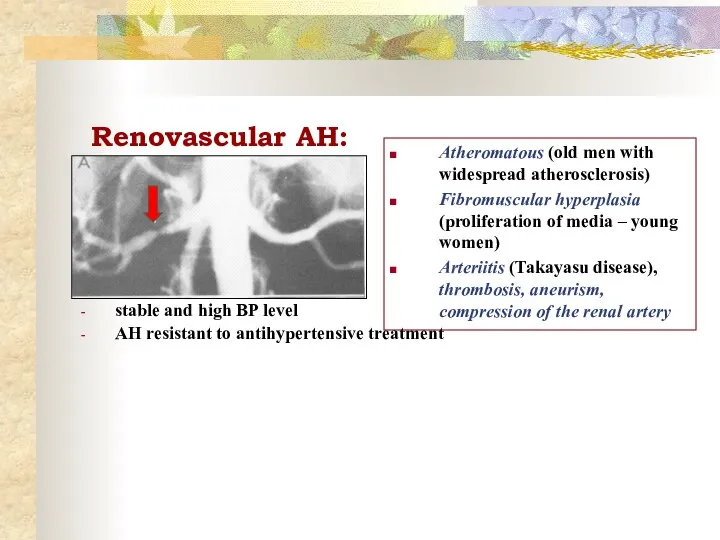
- 37. Renovascular AH: stable and high BP level AH resistant to antihypertensive treatment Atheromatous (old men with
- 38. Diagnostics and treatment of renovascular desease Auscultation: murmur in the paraumbilical region Renal arteriogram Doppler-echocardiography of
- 39. Pheochromacytoma Rare tumor of chromaffin cells (adrenal medulla of the kidneys or the sympathetic ganglia in
- 40. Diagnostics and treatment of Pheochromacytoma Diagnosis: Elevated urinary excretion of vanillylmandelic acid (VMA) and metanephrine Hyperglycemia,
- 41. Primary hypеraldosteronism (Conn`s syndrome) Adenoma of the adrenal, or adrenal hyperplasia Oversecretion of aldosterone ↑ excretion
- 42. Diagnostics and treatment of Conn`s syndrome Diagnosis: Hypokaliemia ( ↓ Renin, ↑ Aldosterone in plasma Identification
- 43. Cushing`s disease & Cushing`s syndrome Cushing`s disease is a primary tumor of the anterior pituitary gland
- 44. Cushing`s syndrome “Moon-like” face Purple striae
- 45. Diagnostics and treatment of Cushing`s disease Diagnosis: ↑ ACTH and Cortisol level in the blood Visualization
- 46. Hyperthyroidism (Graves disease) TSH receptor antibodies → stimulation of thyroid gland → influence of T3 and
- 47. Acromegaly Pituitary adenoma → hypersecretion of growth hormone → Na+ retention → bony overgrowth, hypertension Clinical
- 48. Cardiovascular (hemodynamic) AH: 1. Atherosclerosis of the aorta (↑ regidity of aorta) - elderly and senile
- 49. Cardiovascular (hemodynamic) AH: 3. Coarctation of the aorta (congenital defect) - hyperemia of a face and
- 50. Neurogenic AH Traumas of a skull, meningitis, encephalitis, cerebral atherosclerosis, tumors Severe headaches, dizziness, epilepsy Signs
- 52. Скачать презентацию
Definition
Arterial hypertension (WHO, 1999) is a constantly increased systolic (≥140 mmHg)
Definition
Arterial hypertension (WHO, 1999) is a constantly increased systolic (≥140 mmHg)
Definition
Hypertension is defined as values ≥140 mmHg SBP and/or ≥90
Definition
Hypertension is defined as values ≥140 mmHg SBP and/or ≥90
Why do we take care of arterial hypertension?
“Silent killer of XXI
Why do we take care of arterial hypertension?
“Silent killer of XXI
What do we call “target organs”?
CNS (Strokes 7-10 times more frequent!)
What do we call “target organs”?
CNS (Strokes 7-10 times more frequent!)
Hypertension in the world
33% of the population in USA,
43-44% in
Hypertension in the world
33% of the population in USA,
43-44% in
Prevalence of hypertension
Overall the prevalence of hypertension appears to be around
Prevalence of hypertension
Overall the prevalence of hypertension appears to be around
Report of World Health Organization
In 2020 AD, 2.6 million Indians
Report of World Health Organization
In 2020 AD, 2.6 million Indians
Hypertension in Nigeria
Prevalence of hypertension -28.7%.
Hypertension prevalence was comparable in
Hypertension in Nigeria
Prevalence of hypertension -28.7%.
Hypertension prevalence was comparable in
Hypertension: Predisposing factors
Age > 60 years
Sex (men and postmenopausal women)
Family history
Hypertension: Predisposing factors
Age > 60 years
Sex (men and postmenopausal women)
Family history
Structure of the diagnosis of AH
Primary (essential hypertension) or secondary
Structure of the diagnosis of AH
Primary (essential hypertension) or secondary
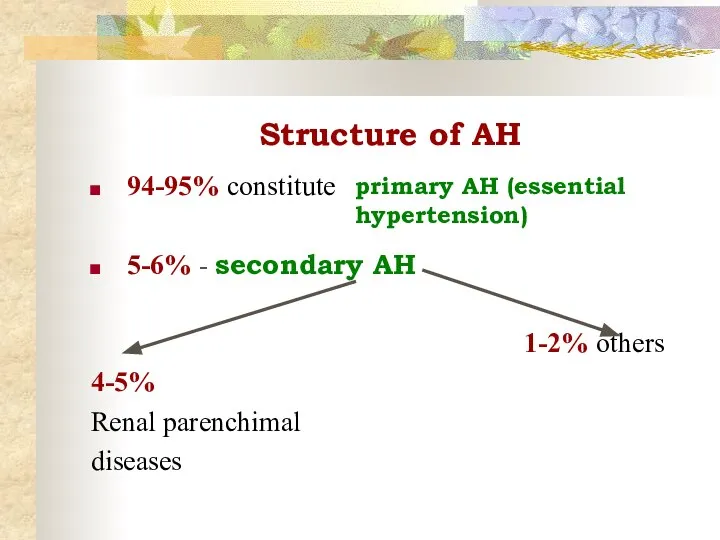
Structure of AH
94-95% constitute
5-6% - secondary AH
4-5%
Renal parenchimal
diseases
1-2% others
primary
Structure of AH
94-95% constitute
5-6% - secondary AH
4-5%
Renal parenchimal
diseases
1-2% others
primary
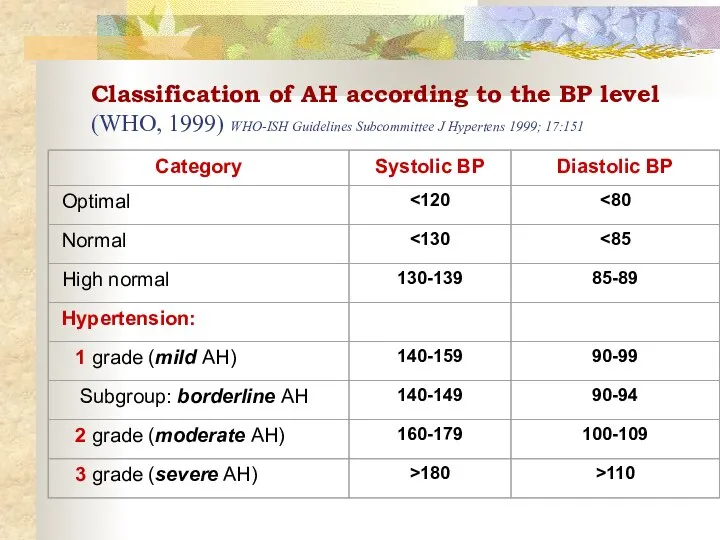
Classification of AH according to the BP level (WHO, 1999) WHO-ISH
Classification of AH according to the BP level (WHO, 1999) WHO-ISH
Classification of AH according to stages
Stage I: no objective signs of
Classification of AH according to stages
Stage I: no objective signs of
Assessment of total cardiovascular risk
The concept is based on the fact
Assessment of total cardiovascular risk
The concept is based on the fact
Assessment of total cardiovascular risk
Estimation of total CV risk is easy
Assessment of total cardiovascular risk
Estimation of total CV risk is easy
Assessment of total cardiovascular risk
The classification in low, moderate, high and
Assessment of total cardiovascular risk
The classification in low, moderate, high and
Factors—other than office BP—influencing
prognosis; used for stratification of total CVrisk
Male sex
Age
Factors—other than office BP—influencing
prognosis; used for stratification of total CVrisk
Male sex
Age
Factors—other than office BP—influencing
prognosis; used for stratification of total CVrisk
Asymptomatic organ
Factors—other than office BP—influencing
prognosis; used for stratification of total CVrisk
Asymptomatic organ
Factors—other than office BP—influencing
prognosis; used for stratification of total CVrisk
Diabetes mellitus:
Fasting
Factors—other than office BP—influencing
prognosis; used for stratification of total CVrisk
Diabetes mellitus:
Fasting
MEASUREMENT OF BLOOD PRESSURE
Use a machine that has been validated, well
MEASUREMENT OF BLOOD PRESSURE
Use a machine that has been validated, well
Types of measurement:
Office BP
Home BP
Daily monitoring of BP!!!
Types of measurement:
Office BP
Home BP
Daily monitoring of BP!!!
‘White coat‘ hypertension?
Up to 13-15% of apparent hypertension in the clinic
‘White coat‘ hypertension?
Up to 13-15% of apparent hypertension in the clinic
Classification of secondary AH
1. Renal:
Renal parenchymal,
Renovascular
Anephric
2. Endocrinological:
Cushing`s syndrome and disease
Primary aldosteronism
Pheochromacytoma
Primary
Classification of secondary AH
1. Renal:
Renal parenchymal,
Renovascular
Anephric
2. Endocrinological:
Cushing`s syndrome and disease
Primary aldosteronism
Pheochromacytoma
Primary
Classification of secondary AH
3. Neurogenic:
- In increased intracranial pressure (tumors,
Classification of secondary AH
3. Neurogenic:
- In increased intracranial pressure (tumors,
Classification of secondary AH
5. Pharmacological (iatrogenic)
Corticosteroids
Excessive thyroxine
Oral contraceptives, containing oestrogens
Sympatomimetics (for
Classification of secondary AH
5. Pharmacological (iatrogenic)
Corticosteroids
Excessive thyroxine
Oral contraceptives, containing oestrogens
Sympatomimetics (for
Routine tests
• Haemoglobin and/or haematocrit.
• Fasting plasma glucose.
• Serum total
Routine tests
• Haemoglobin and/or haematocrit.
• Fasting plasma glucose.
• Serum total
Obligatory investigation to detect the secondary hypertension
• Chest radiograph: to detect
Obligatory investigation to detect the secondary hypertension
• Chest radiograph: to detect
Life style modifications
Lose weight, if overweight
Limit alcohol intake
Increase physical activity
Reduce salt
Life style modifications
Lose weight, if overweight
Limit alcohol intake
Increase physical activity
Reduce salt
Principles of treatment
1. Etiological: elimination of causes
2. Non-pharmacological treatment: weight reduction,
Principles of treatment
1. Etiological: elimination of causes
2. Non-pharmacological treatment: weight reduction,
Treatment strategies
1) Treatment is permanent and continuous
2) Begin treatment with a
Treatment strategies
1) Treatment is permanent and continuous 2) Begin treatment with a
Angiotensin II
inhibitors
ACE-inhibitors
Diuretics
Ca-blockers
or
+
Top-priority combinations of AHT
Angiotensin II
inhibitors
ACE-inhibitors
Diuretics
Ca-blockers
or
+
Top-priority combinations of AHT
Renal parenchymal AH:
chronic glomerulonephritis,
pyelonephritis,
polycystic renal disease,
diabetic nephropathy,
congenital
Renal parenchymal AH:
chronic glomerulonephritis,
pyelonephritis,
polycystic renal disease,
diabetic nephropathy,
congenital
Diagnostics of renal parenchymal diseases
urinary syndrome (proteinuria, leucocyturia, hematuria, cylindruria, bacteriuria),
testing
Diagnostics of renal parenchymal diseases
urinary syndrome (proteinuria, leucocyturia, hematuria, cylindruria, bacteriuria),
testing
The renin-angiotensin-aldosterone system
The renin-angiotensin-aldosterone system
Renovascular AH:
stable and high BP level
AH resistant to antihypertensive treatment
Atheromatous (old
Renovascular AH:
stable and high BP level
AH resistant to antihypertensive treatment
Atheromatous (old
Diagnostics and treatment of renovascular desease
Auscultation: murmur in the paraumbilical region
Diagnostics and treatment of renovascular desease
Auscultation: murmur in the paraumbilical region
Pheochromacytoma
Rare tumor of chromaffin cells (adrenal medulla of the kidneys or
Pheochromacytoma
Rare tumor of chromaffin cells (adrenal medulla of the kidneys or
Diagnostics and treatment
of Pheochromacytoma
Diagnosis:
Elevated urinary excretion of vanillylmandelic acid
Diagnostics and treatment
of Pheochromacytoma
Diagnosis:
Elevated urinary excretion of vanillylmandelic acid
Primary hypеraldosteronism (Conn`s syndrome)
Adenoma of the adrenal, or adrenal hyperplasia
Oversecretion of
Primary hypеraldosteronism (Conn`s syndrome)
Adenoma of the adrenal, or adrenal hyperplasia
Oversecretion of
Diagnostics and treatment of Conn`s syndrome
Diagnosis:
Hypokaliemia (<3,5 μmol/l), ↑ Na+
Diagnostics and treatment of Conn`s syndrome
Diagnosis:
Hypokaliemia (<3,5 μmol/l), ↑ Na+
Cushing`s disease & Cushing`s syndrome
Cushing`s disease is a primary
Cushing`s disease & Cushing`s syndrome
Cushing`s disease is a primary
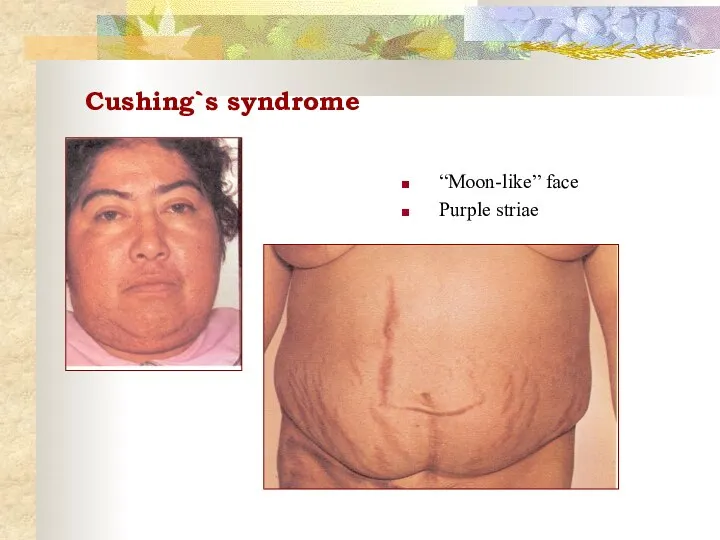
Cushing`s syndrome
“Moon-like” face
Purple striae
Cushing`s syndrome
“Moon-like” face
Purple striae
Diagnostics and treatment of Cushing`s disease
Diagnosis:
↑ ACTH and Cortisol level
Diagnostics and treatment of Cushing`s disease
Diagnosis:
↑ ACTH and Cortisol level
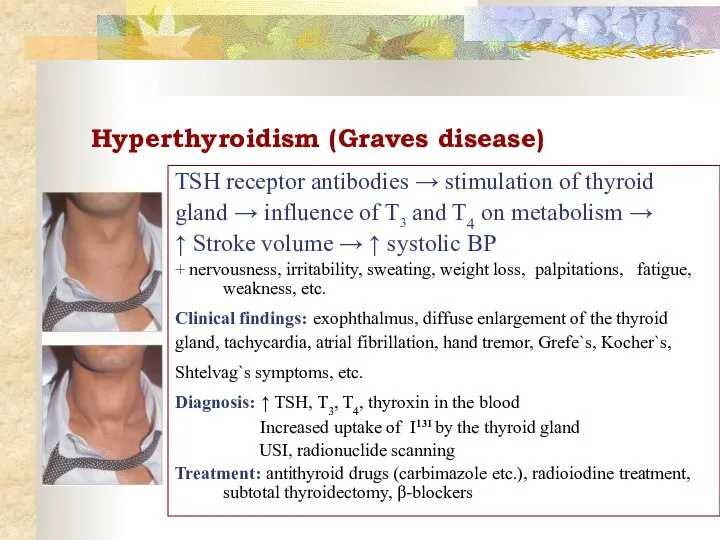
Hyperthyroidism (Graves disease)
TSH receptor antibodies → stimulation of thyroid
gland →
Hyperthyroidism (Graves disease)
TSH receptor antibodies → stimulation of thyroid
gland →
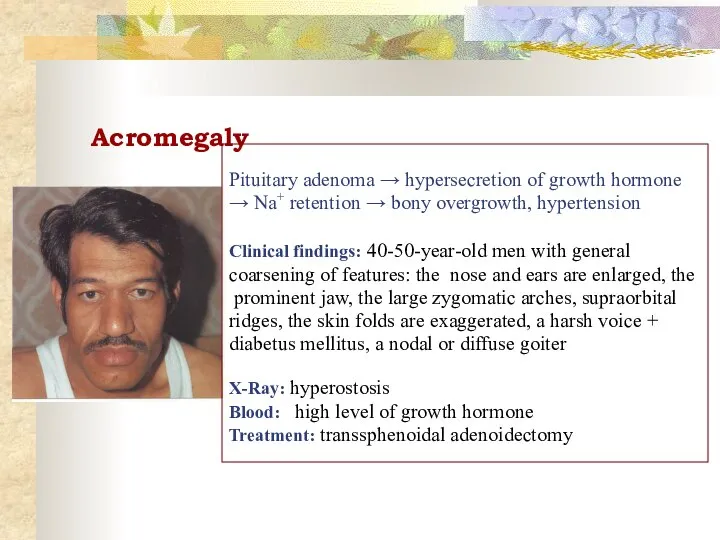
Acromegaly
Pituitary adenoma → hypersecretion of growth hormone
→ Na+ retention
Acromegaly
Pituitary adenoma → hypersecretion of growth hormone
→ Na+ retention
Cardiovascular (hemodynamic) AH:
1. Atherosclerosis of the aorta (↑ regidity of aorta)
-
Cardiovascular (hemodynamic) AH:
1. Atherosclerosis of the aorta (↑ regidity of aorta)
-
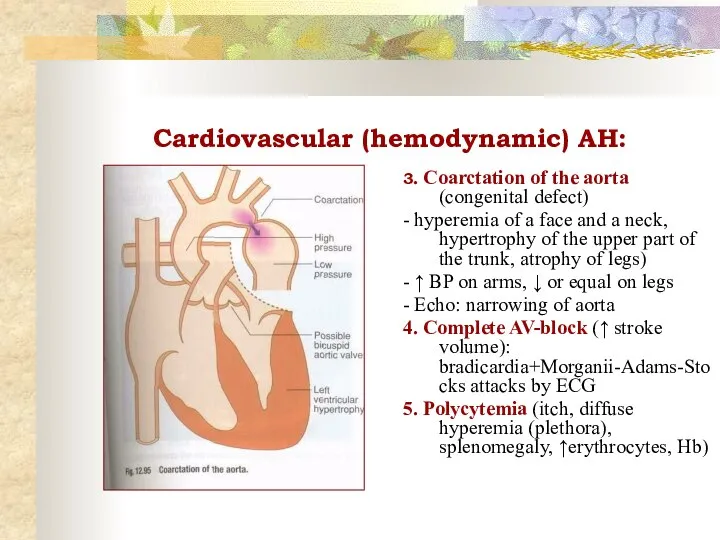
Cardiovascular (hemodynamic) AH:
3. Coarctation of the aorta (congenital defect)
- hyperemia of
Cardiovascular (hemodynamic) AH:
3. Coarctation of the aorta (congenital defect)
- hyperemia of
Neurogenic AH
Traumas of a skull, meningitis, encephalitis, cerebral atherosclerosis, tumors
Severe headaches,
Neurogenic AH
Traumas of a skull, meningitis, encephalitis, cerebral atherosclerosis, tumors
Severe headaches,
 Healthy lifestyle
Healthy lifestyle домашние часы _ by Artem Morozov
домашние часы _ by Artem Morozov Процесс прохождения клиента (нарушения рабочего листа). Злоупотребления при сдаче а/м по системе Трейд-ин
Процесс прохождения клиента (нарушения рабочего листа). Злоупотребления при сдаче а/м по системе Трейд-ин Випускова робота Особливості застосування дощувальної техніки на чорноземних грунтах Горностаївського району
Випускова робота Особливості застосування дощувальної техніки на чорноземних грунтах Горностаївського району Чайные сервиз
Чайные сервиз Гимнастика для глаз
Гимнастика для глаз 3D телевидение
3D телевидение Село родное в объективе
Село родное в объективе Электрические схемы
Электрические схемы La tour Еiffel
La tour Еiffel Anketa_Knigi_stilya_2
Anketa_Knigi_stilya_2 Тренажёр Личные местоимения 3 класс
Тренажёр Личные местоимения 3 класс Уфа. Фото-кастинг
Уфа. Фото-кастинг 20120514_trafalgar
20120514_trafalgar Stagioni nel cinema
Stagioni nel cinema Lesson_1_Этапы_процесса_разработки
Lesson_1_Этапы_процесса_разработки Що читають знаменитості
Що читають знаменитості Нитинол
Нитинол South Korea
South Korea Изготовление крышек центрального отверстия автомобильных дисков с применением аддитивных технологий
Изготовление крышек центрального отверстия автомобильных дисков с применением аддитивных технологий блоксхема1
блоксхема1 Расчет основания фундамента на несущую способность
Расчет основания фундамента на несущую способность Производство. Выполняемые работы и услуги
Производство. Выполняемые работы и услуги Дороги которые мы выбираем
Дороги которые мы выбираем pREZENT-1
pREZENT-1 Материалы применяемые в машино и приборостроении
Материалы применяемые в машино и приборостроении BAE Systems, Inc. Sectors at a Glance
BAE Systems, Inc. Sectors at a Glance Көліктік моторлардың қалдық газдарының уыттылығын төмендетудің негізгі әдістері
Көліктік моторлардың қалдық газдарының уыттылығын төмендетудің негізгі әдістері