- General anaesthetics

Содержание
- 2. General anaesthetics (GAs) are drugs which produce reversible loss of all sensation and consciousness. The cardinal
- 3. Mechanism of action of anaesthetics Anaesthetic potency correlates well with lipid solubility. Anaesthetics might dissolve in
- 4. Properties of an ideal anaesthetic A. For the patient: It should be pleasant, nonirritating, should not
- 5. C. For the anaesthetist: Its administration should be easy, controllable. Heart, liver and other organs should
- 6. Stages of general anaesthesia I. Stage of analgesia starts from beginning of anaesthetic inhalation and lasts
- 8. General anaesthesia usually involves the administration of different drugs For premedication, For induction of anaesthesia, and
- 9. CLASSIFICATION Inhalational Gas: Nitrous oxide Volatile liquids: Ether, Halothane, Enflurane, Isoflurane, Desflurane, Sevoflurane Intravenous Fast acting
- 10. Nitrous oxide is not potent enough to use as a sole anaesthetic agent, but it is
- 11. Isoflurane is more soluble in blood than sevoflurane or enflurane and so onset and recovery are
- 12. Propofol is the most widely used intravenous anaesthetic. It induces anaesthesia within 30 s and is
- 13. Ketamine may be given by intramuscular or intravenous injection. It is analgesic in subanaesthetic doses, but
- 14. COMPLICATIONS OF GENERAL ANAESTHESIA A. During anaesthesia Respiratory depression. Cardiac arrhythmias, asystole. Fall in BP. Salivation,
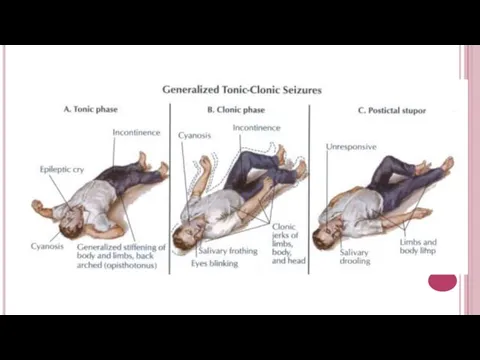
- 15. ANTIEPILEPTIC DRUGS Epilepsy is a chronic disease in which seizures result from the abnormal discharge of
- 17. Absence seizures last about 1/2 min. Momentary loss of consciousness, patient apparently freezes and stares in
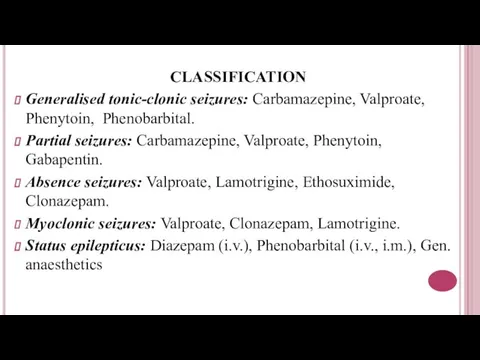
- 18. CLASSIFICATION Generalised tonic-clonic seizures: Carbamazepine, Valproate, Phenytoin, Phenobarbital. Partial seizures: Carbamazepine, Valproate, Phenytoin, Gabapentin. Absence seizures:
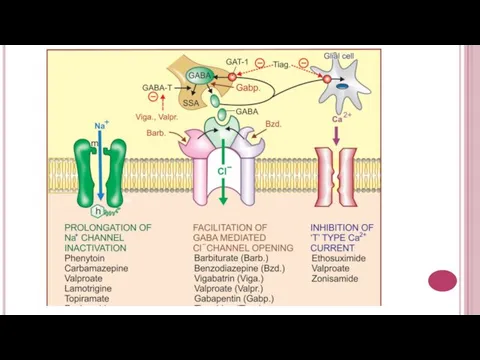
- 19. Carbamazepine, lamotrigine, valproate, phenytoin block neuronal Na+ channels, ↓ axonal conduction. Barbiturates and benzodiazepins ↑inhibitory tone
- 21. Phenytoin. Pharmacokinetics – variable absorption, induction of P450s; Side effects: CNS depression, gingival hyperplasia, osteomalacia (↓
- 22. Valproate can be used for migraines. Inhibits P450s. Side effects: hepatotoxicity, thrombocytopenia, pancretitis, alopecia, teratogenicity (spinal
- 23. Antiparkinsonian Drugs. These are drugs that have a therapeutic effect in parkinsonism. Parkinsonism. It is an
- 26. CLASSIFICATION I. Drugs affecting brain dopaminergic system Dopamine precursor : Levodopa (l-dopa) Peripheral decarboxylase inhibitors :
- 28. Levodopa. Mechanism of action: Levodopa is the immediate precursor of dopamine and is able to penetrate
- 30. The DA agonists can act on striatal DA receptors Bromocriptine is a potent agonist on D2receptors.
- 31. Amantadine has muscarinic blocking actions and probably increases dopamine release. It has modest antiparkinsonian effects in
- 33. Скачать презентацию
General anaesthetics (GAs) are drugs which produce reversible loss of all
General anaesthetics (GAs) are drugs which produce reversible loss of all
Mechanism of action of anaesthetics
Anaesthetic potency correlates well with lipid solubility.
Mechanism of action of anaesthetics
Anaesthetic potency correlates well with lipid solubility.
Properties of an ideal anaesthetic
A. For the patient:
It should be
Properties of an ideal anaesthetic
A. For the patient:
It should be
C. For the anaesthetist:
Its administration should be easy, controllable.
Heart,
C. For the anaesthetist:
Its administration should be easy, controllable.
Heart,
Stages of general anaesthesia
I. Stage of analgesia starts from beginning of
Stages of general anaesthesia
I. Stage of analgesia starts from beginning of

General anaesthesia usually involves the administration of different drugs
For premedication,
For induction
General anaesthesia usually involves the administration of different drugs
For premedication,
For induction
CLASSIFICATION
Inhalational
Gas: Nitrous oxide
Volatile liquids: Ether, Halothane, Enflurane, Isoflurane, Desflurane, Sevoflurane
Intravenous
Fast
CLASSIFICATION
Inhalational
Gas: Nitrous oxide
Volatile liquids: Ether, Halothane, Enflurane, Isoflurane, Desflurane, Sevoflurane
Intravenous
Fast
Nitrous oxide is not potent enough to use as a sole
Nitrous oxide is not potent enough to use as a sole

Isoflurane is more soluble in blood than sevoflurane or enflurane and
Isoflurane is more soluble in blood than sevoflurane or enflurane and
Propofol is the most widely used intravenous anaesthetic. It induces anaesthesia
Propofol is the most widely used intravenous anaesthetic. It induces anaesthesia
Ketamine may be given by intramuscular or intravenous injection. It is
Ketamine may be given by intramuscular or intravenous injection. It is
COMPLICATIONS OF GENERAL ANAESTHESIA
A. During anaesthesia
Respiratory depression. Cardiac arrhythmias,
COMPLICATIONS OF GENERAL ANAESTHESIA
A. During anaesthesia
Respiratory depression. Cardiac arrhythmias,
ANTIEPILEPTIC DRUGS
Epilepsy is a chronic disease in which seizures result from
ANTIEPILEPTIC DRUGS
Epilepsy is a chronic disease in which seizures result from
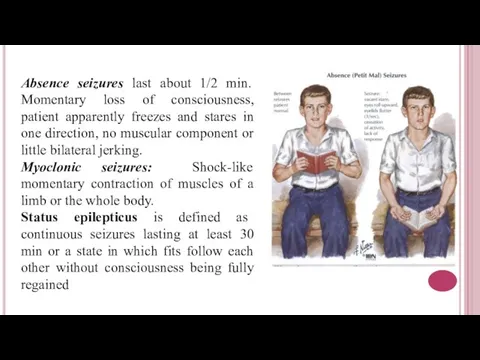
Absence seizures last about 1/2 min. Momentary loss of consciousness, patient
Absence seizures last about 1/2 min. Momentary loss of consciousness, patient
CLASSIFICATION
Generalised tonic-clonic seizures: Carbamazepine, Valproate, Phenytoin, Phenobarbital.
Partial seizures: Carbamazepine, Valproate, Phenytoin,
CLASSIFICATION
Generalised tonic-clonic seizures: Carbamazepine, Valproate, Phenytoin, Phenobarbital.
Partial seizures: Carbamazepine, Valproate, Phenytoin,
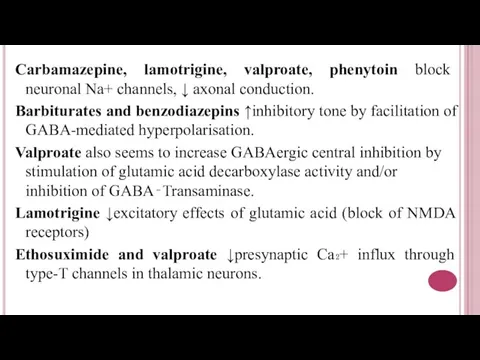
Carbamazepine, lamotrigine, valproate, phenytoin block neuronal Na+ channels, ↓ axonal conduction.
Carbamazepine, lamotrigine, valproate, phenytoin block neuronal Na+ channels, ↓ axonal conduction.
Phenytoin. Pharmacokinetics – variable absorption, induction of P450s;
Side effects: CNS
Phenytoin. Pharmacokinetics – variable absorption, induction of P450s;
Side effects: CNS
Valproate can be used for migraines. Inhibits P450s. Side effects: hepatotoxicity,
Valproate can be used for migraines. Inhibits P450s. Side effects: hepatotoxicity,
Antiparkinsonian Drugs.
These are drugs that have a therapeutic effect in
Antiparkinsonian Drugs.
These are drugs that have a therapeutic effect in


CLASSIFICATION
I. Drugs affecting brain dopaminergic system
Dopamine precursor : Levodopa (l-dopa)
Peripheral
CLASSIFICATION
I. Drugs affecting brain dopaminergic system
Dopamine precursor : Levodopa (l-dopa)
Peripheral

Levodopa. Mechanism of action: Levodopa is the immediate precursor of dopamine
Levodopa. Mechanism of action: Levodopa is the immediate precursor of dopamine

The DA agonists can act on striatal DA receptors
Bromocriptine
The DA agonists can act on striatal DA receptors
Bromocriptine
Amantadine has muscarinic blocking actions and probably increases dopamine release. It
Amantadine has muscarinic blocking actions and probably increases dopamine release. It
 Проектирование подстанции 110/10 кВ в г. Пермь
Проектирование подстанции 110/10 кВ в г. Пермь Зачем искусство
Зачем искусство Сварочные выпрямители и их эксплуатация
Сварочные выпрямители и их эксплуатация Встречные забои
Встречные забои Проектирование и организация работы отделения по ремонту роликовых подшипников
Проектирование и организация работы отделения по ремонту роликовых подшипников Связующие для неводных окрасочных составов. Тема № 4. Растительные масла
Связующие для неводных окрасочных составов. Тема № 4. Растительные масла Выпуск 2008 представляет
Выпуск 2008 представляет История Обществознание
История Обществознание 20120225_nabokov_poseshchenie_muzeya
20120225_nabokov_poseshchenie_muzeya игра Собери фрукты
игра Собери фрукты Критическая и максимально применяемая частоты. Методы исследования ионосферы
Критическая и максимально применяемая частоты. Методы исследования ионосферы Победа ковалась в тылу
Победа ковалась в тылу Технология и организация высокотехнологичного производства
Технология и организация высокотехнологичного производства 20120305_velikiy_dar_tvorchestva
20120305_velikiy_dar_tvorchestva Пламенный Серафим
Пламенный Серафим Приемы работы_2017
Приемы работы_2017 Event DJ AndRave pres-2
Event DJ AndRave pres-2 Технология возведения работ нулевого цикла
Технология возведения работ нулевого цикла Автоматическое регулирование расхода природного газа в двухванном сталеплавильном агрегате ДСПА-32
Автоматическое регулирование расхода природного газа в двухванном сталеплавильном агрегате ДСПА-32 Производство хлебобулочных изделий
Производство хлебобулочных изделий Алгоритмы и исполнители
Алгоритмы и исполнители Волшебный мир коми сказок
Волшебный мир коми сказок Маленькие истории о больших музыкантах
Маленькие истории о больших музыкантах Тварина - живий організм
Тварина - живий організм ПрезентацияБайкалЮгповерпоинт (1)
ПрезентацияБайкалЮгповерпоинт (1) Когда музыка не нуждается в словах
Когда музыка не нуждается в словах Термическая обработка металлов и сплавов
Термическая обработка металлов и сплавов Основы производственных процессов. Офсетные печатные формы
Основы производственных процессов. Офсетные печатные формы