- Oncological Emergencies

Содержание
- 2. What is Oncologic Emergency? A clinical condition resulting from a metabolic, neurologic, cardiovascular, hematologic, and/or infectious
- 5. METABOLIC
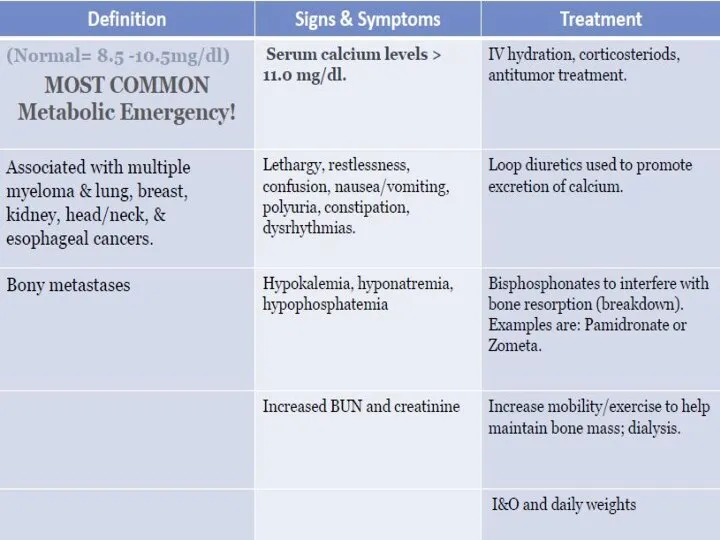
- 6. Hypercalcemia of Malignancy. Major Mechanisms: Local osteolytic hypercalcemia Osteoclastic bone resorbing cytokines In Extensive bone metastases
- 8. Symptoms GI : Nausea, vomiting, Anorexia,Constipation Renal Polyuria due to interference with ADH- Diabetes insipidus-like syndrome,
- 9. Lab Total calcium & albumin or ionized calcium Medical emergency above 10.5 mg/dL Phosphorus Creatinine, urea
- 13. Cиндром неадекватной секреции антидиуретического гормона (SIADH)
- 15. Osmotic Demyelination Syndrome Recall that during chronic hyponatremia, osmolytes are shifted out of brain cells to
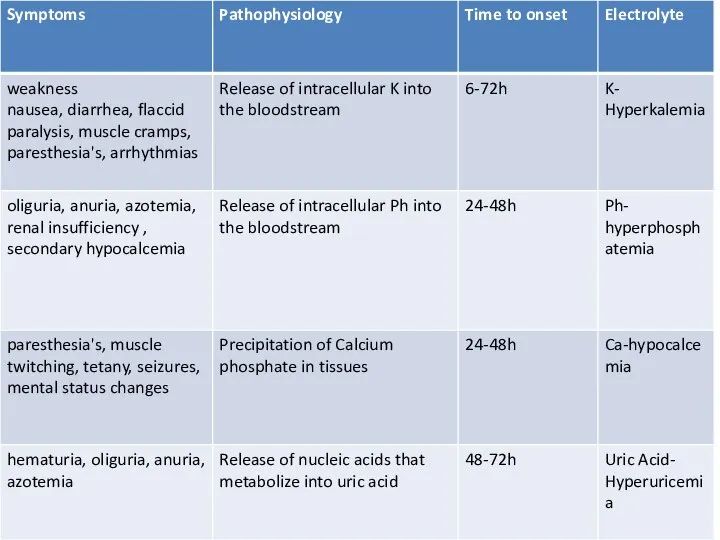
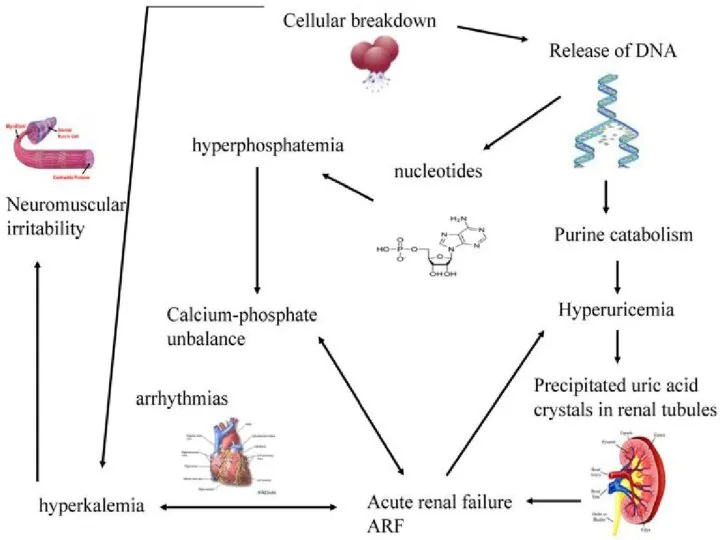
- 18. Acute Tumor Lysis Syndrome Usually starts 6-72 h from initiation of chemo or radiotherapy Due to
- 19. Etiologic Factors Large Tumor burden High growth fraction High pre treatment serum LDH or Uric Acid
- 22. Treatment Best treatment – prevention Hydration – 3L\24h, better started 24-48 h before treatment initiation Stop
- 23. Stop the chemotherapy Aggressive IV hydration / diuresis CaCl2, NaHCO3, glucose / insulin, kayexalate for hyperkalemia
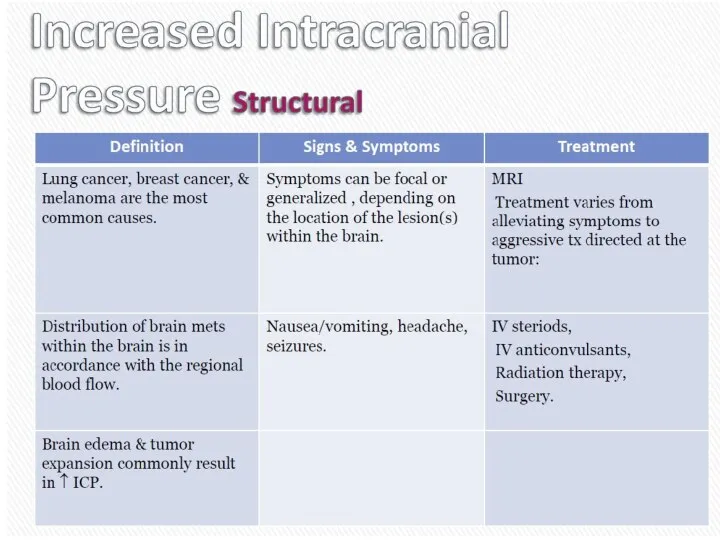
- 27. STRUCTURAL: Neurologic emergencies
- 28. Spinal Cord Compression
- 29. What is malignant spinal cord compression? Occurs when cancer cells grow in/near to spine and press
- 30. Most commonly seen in Breast Lung Prostate Lymphoma Myeloma About 10% of patients with cancer overall
- 31. Method of spread 85%From vertebral body or pedicle 10% Through intervertebral foramina (from paravertebral nodes or
- 32. Location Thoracic spine 60-70% Lumbosacral spine 20-30% Cervical and sacral spine less then 10% each
- 34. First Symptoms Pain 95% Weakness 5% Ataxia 1% Sensory loss 1% RED FLAGS…..
- 35. First Red Flag: Pain Usually first and most common symptom (80-90%) Usually precedes other neurologic symptoms
- 36. Second Red Flag: Motor Weakness: 60-85% At or above conus medularis Extensors of the upper extremities
- 37. Third Red Flag: Bladder & Bowel Function Loss is late finding Problems passing urine may include
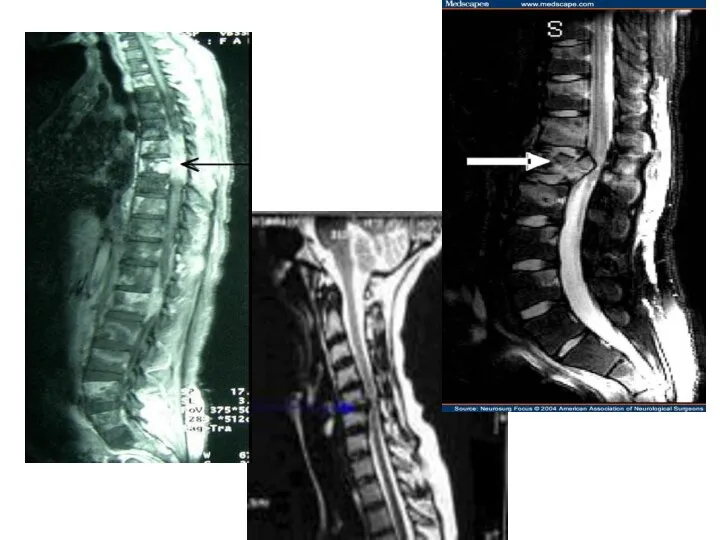
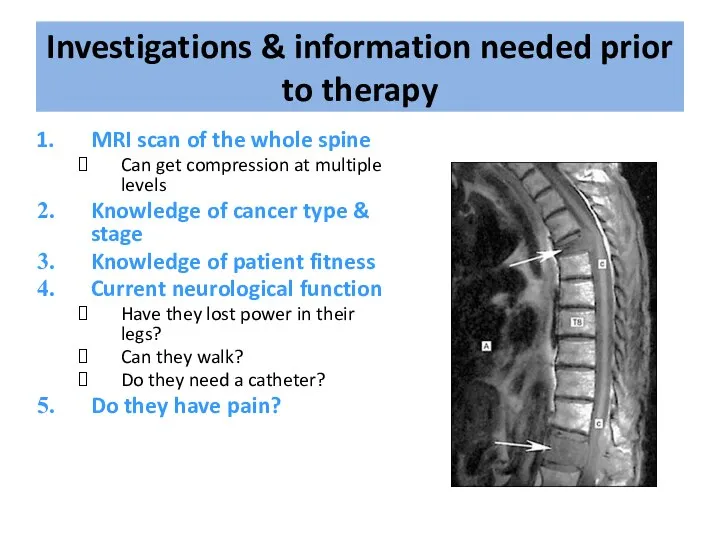
- 38. Investigations & information needed prior to therapy MRI scan of the whole spine Can get compression
- 39. Treatment options include: Immobilisation Steroids & gastric protection Analgesia Surgery – decompression & stabilisation of the
- 40. Indications for Surgery • Unknown primary tumour • Relapse post RT • Progression while on RT
- 41. Surgery
- 45. Improvement in surgery + RT Days remained ambulatory (126 vs. 35) Percent that regained ambulation after
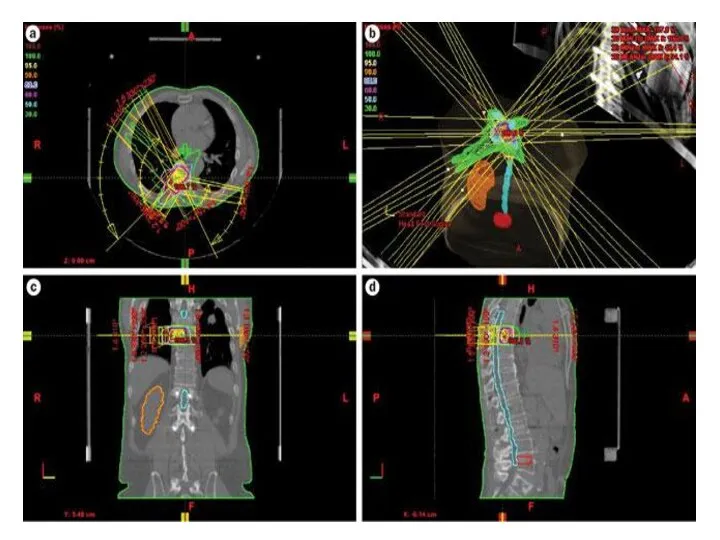
- 46. Radiation Therapy
- 48. Prognosis Median survival with MSCC is 6 months Ambulatory patients with radiosensitive tumours have the best
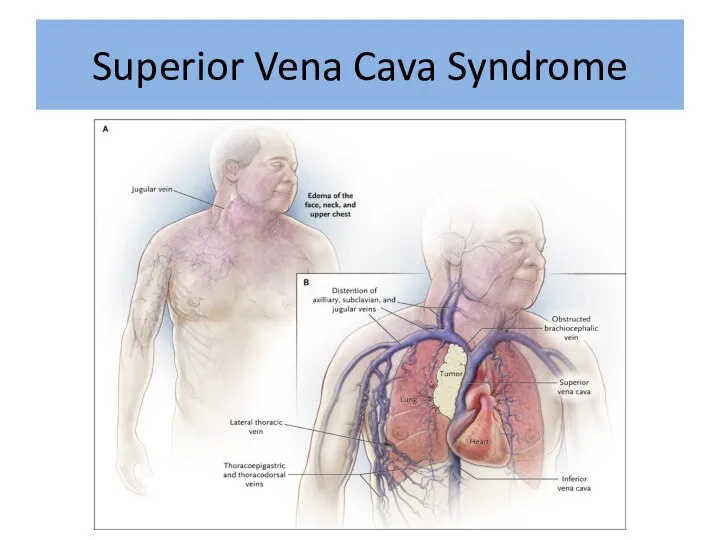
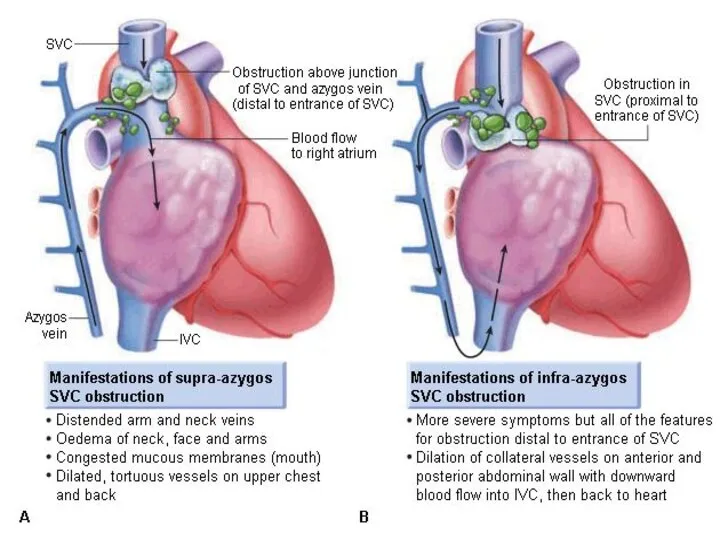
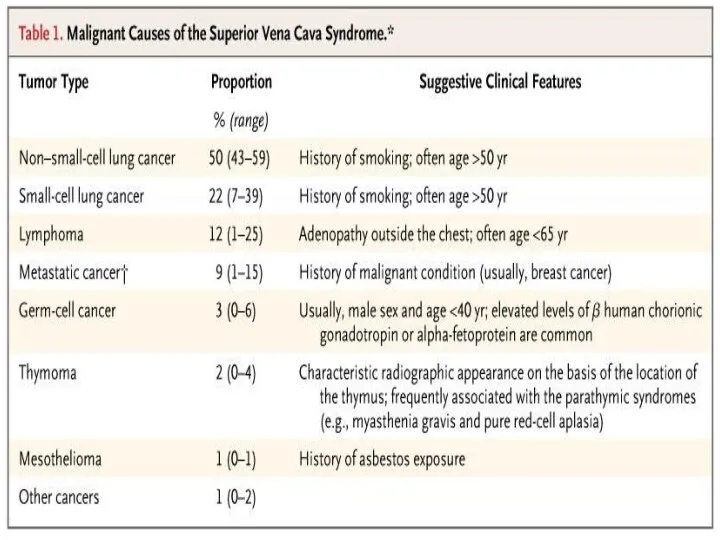
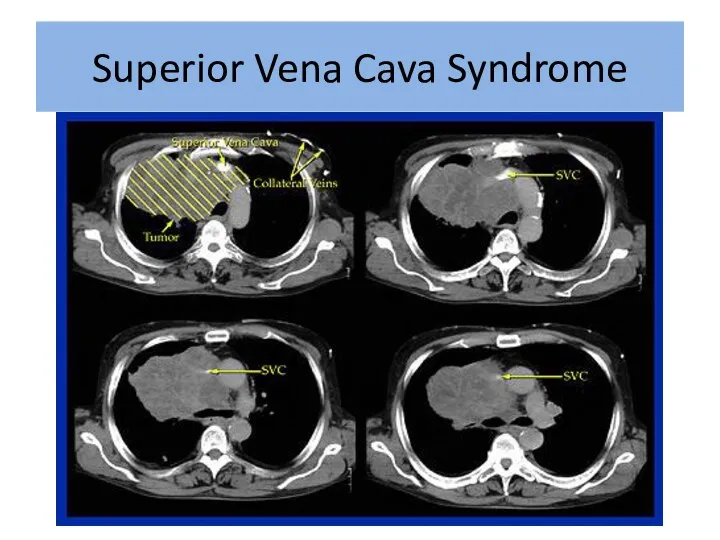
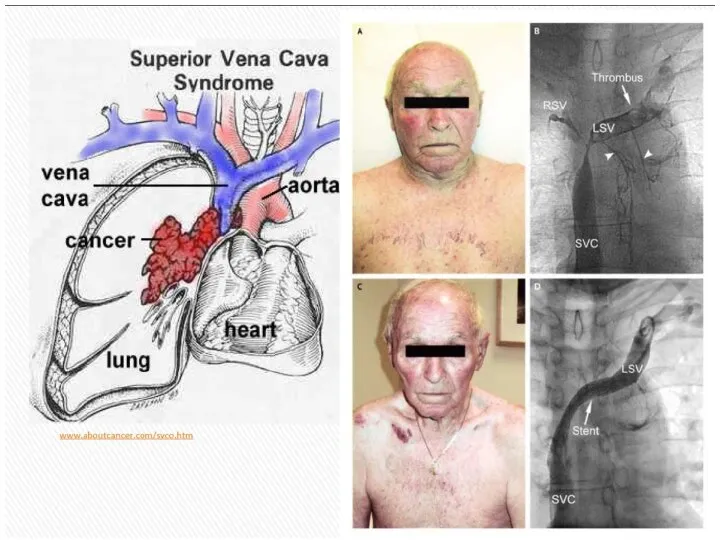
- 49. Superior Vena Cava Syndrome
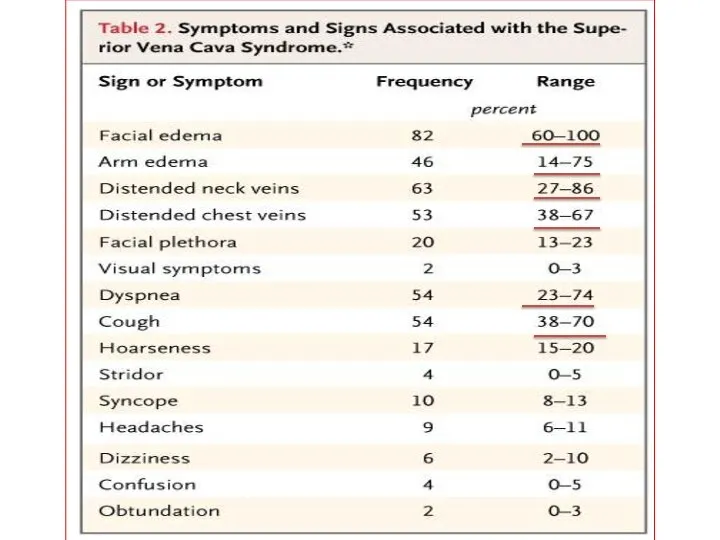
- 51. Superior Vena Cava Syndrome
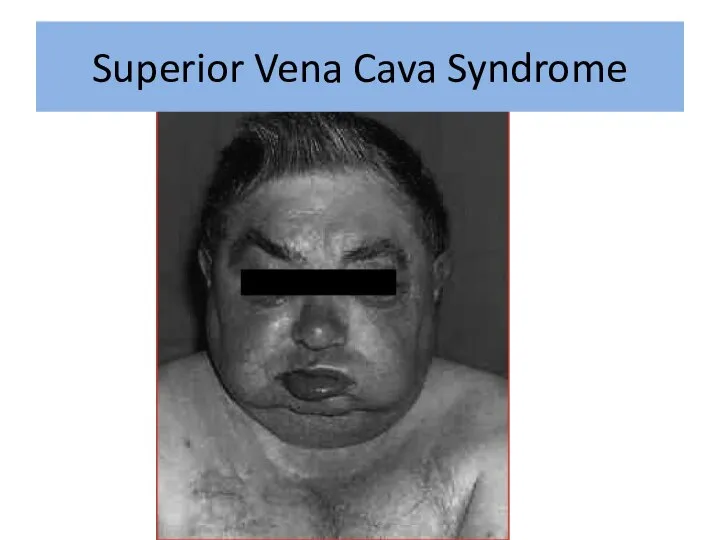
- 52. Superior Vena Cava Syndrome
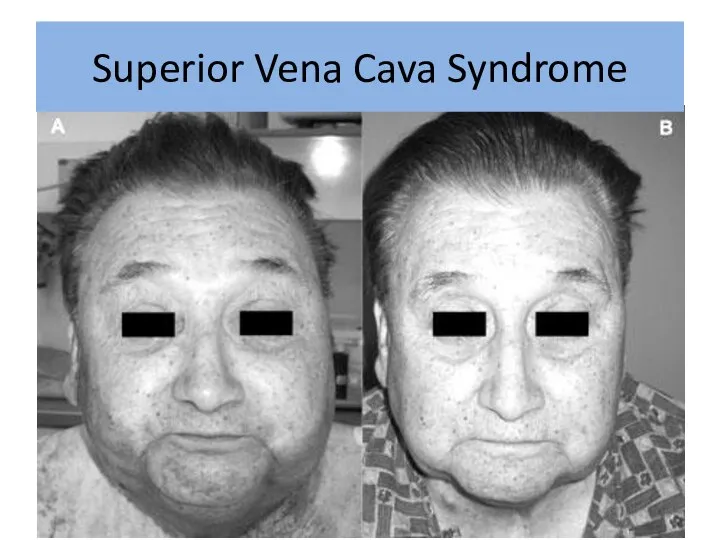
- 54. Superior Vena Cava Syndrome
- 57. In rare cases can be disease presentation No time for pathology Urgent treatment without tissue diagnosis
- 58. Exeption: Treatment Sensitive Tumors NHLs, germ cells, and limited-stage small cell lung cancers usually respond to
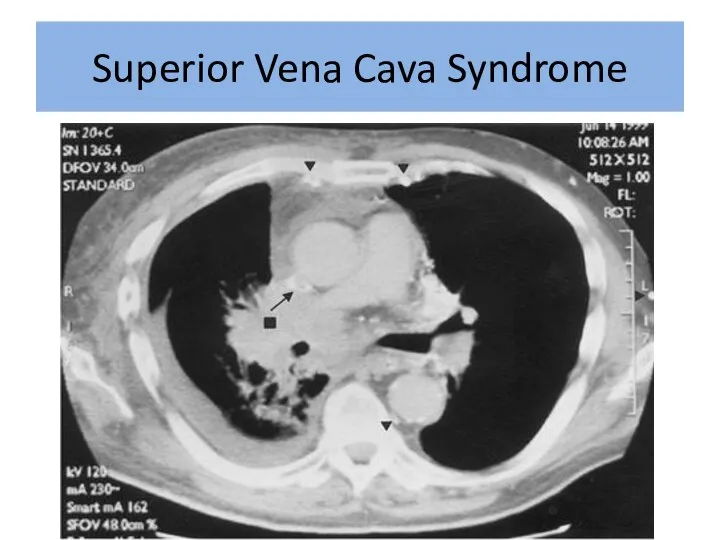
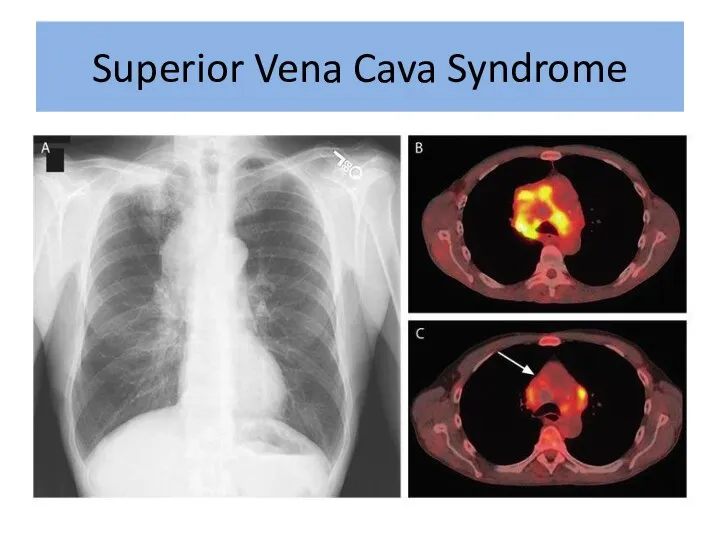
- 59. Superior Vena Cava Syndrome
- 60. Superior Vena Cava Syndrome
- 61. Superior Vena Cava Syndrome
- 62. Treatment Options Radiation therapy Chemotherapy Intraluminal Stent +supportive care
- 63. Supportive Care: Rest Head elevation Oxygen Diuretics Anticoagulation Steroids Avoid high volume fluid infusion through upper
- 64. Intraluminal Stents Endovascular placement under fluoroscopy Patients who have recurrent disease in previously irradiated fields Tumors
- 66. Endovascular stenting and angioplasty Superior vena cava syndrome
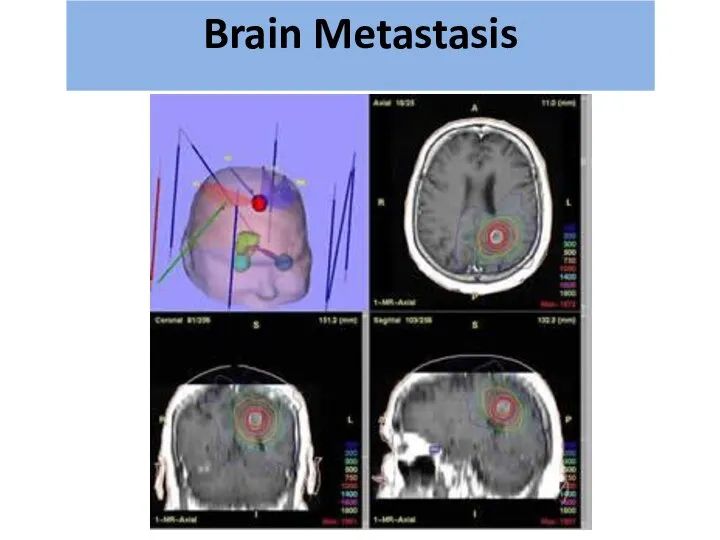
- 70. Most Common type of CNS malignancy 20-40% of cancer patients will develop brain mets Most common
- 71. Recursive Partitioning Analysis - RPA גרורות מוחיות Brain Metastasis
- 72. גרורות מוחיות Brain Metastasis
- 73. Diagnosis: CT with and without contrast MRI – modality of choice for small lesions including leptomeningial
- 74. גרורות מוחיות Brain Metastasis
- 75. גרורות מוחיות Brain Metastasis
- 76. גרורות מוחיות Brain Metastasis
- 77. Treatment: Steroids – Dexamethasone 16mg*2 Anticonvulsant Surgery? Radiation therapy גרורות מוחיות Brain Metastasis
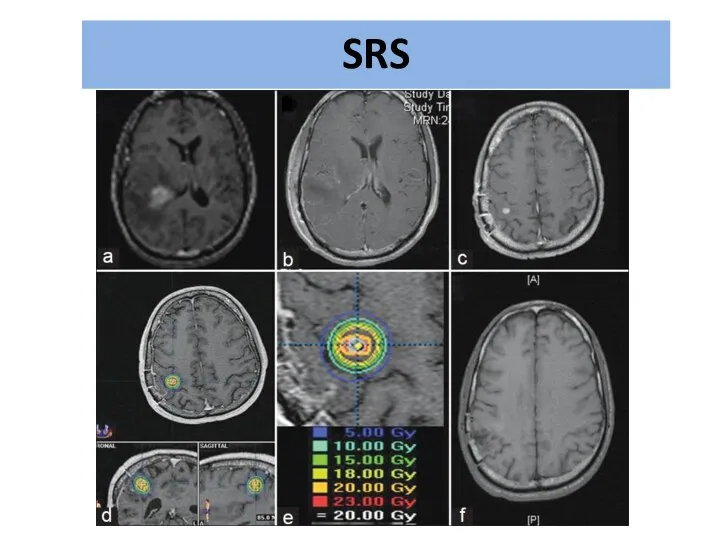
- 78. Radiation therapy WBRT=Whole Brain RT SRS=Stereotactic Radio Surgery גרורות מוחיות Brain Metastasis
- 79. גרורות מוחיות German Helmet Brain Metastasis
- 80. גרורות מוחיות Brain Metastasis
- 81. גרורות מוחיות Brain Metastasis
- 82. SRS
- 83. גרורות מוחיות Brain Metastasis
- 85. Скачать презентацию
What is Oncologic Emergency?
A clinical condition resulting from a metabolic, neurologic,
What is Oncologic Emergency?
A clinical condition resulting from a metabolic, neurologic,
METABOLIC
METABOLIC
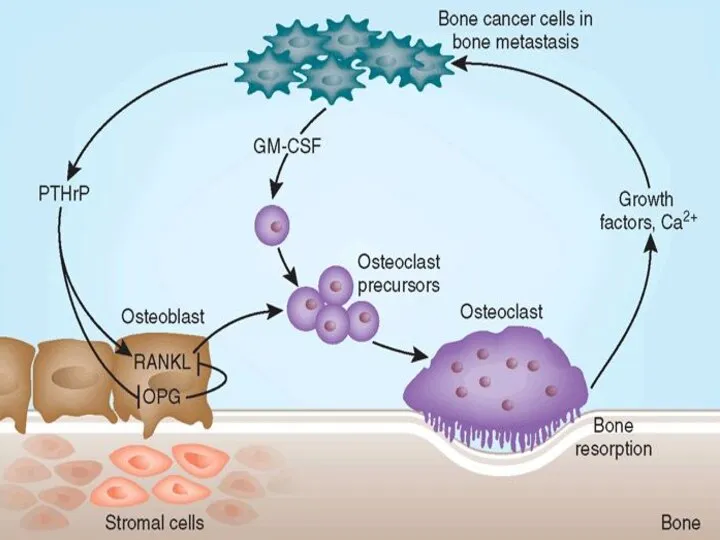
Hypercalcemia of Malignancy.
Major Mechanisms:
Local osteolytic hypercalcemia
Osteoclastic bone resorbing cytokines
In Extensive bone
Hypercalcemia of Malignancy.
Major Mechanisms:
Local osteolytic hypercalcemia
Osteoclastic bone resorbing cytokines
In Extensive bone
Symptoms
GI :
Nausea, vomiting, Anorexia,Constipation
Renal
Polyuria due to interference with ADH- Diabetes
Symptoms
GI :
Nausea, vomiting, Anorexia,Constipation
Renal
Polyuria due to interference with ADH- Diabetes
Lab
Total calcium & albumin or ionized calcium
Medical emergency above 10.5 mg/dL
Phosphorus
Creatinine,
Lab
Total calcium & albumin or ionized calcium
Medical emergency above 10.5 mg/dL
Phosphorus
Creatinine,
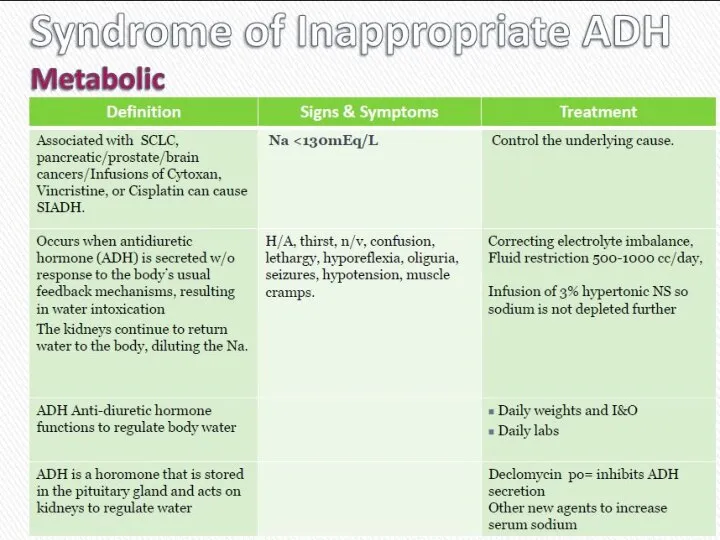
Cиндром неадекватной секреции антидиуретического гормона
(SIADH)
Cиндром неадекватной секреции антидиуретического гормона
(SIADH)

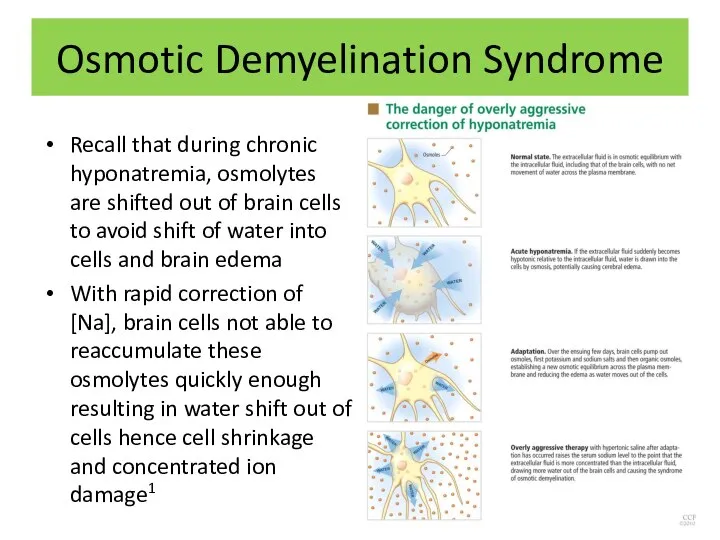
Osmotic Demyelination Syndrome
Recall that during chronic hyponatremia, osmolytes are shifted out
Osmotic Demyelination Syndrome
Recall that during chronic hyponatremia, osmolytes are shifted out
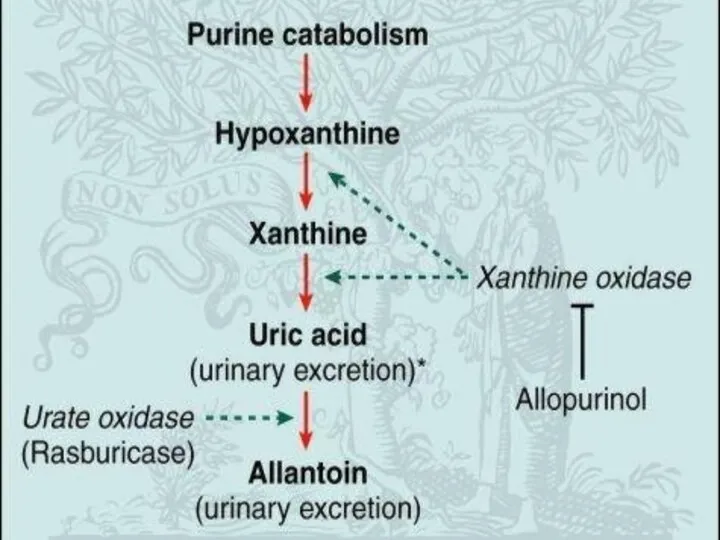
Acute Tumor Lysis Syndrome
Usually starts 6-72 h from initiation of chemo
Acute Tumor Lysis Syndrome
Usually starts 6-72 h from initiation of chemo
Etiologic Factors
Large Tumor burden
High growth fraction
High pre treatment serum LDH
Etiologic Factors
Large Tumor burden
High growth fraction
High pre treatment serum LDH
Treatment
Best treatment – prevention
Hydration – 3L\24h, better started 24-48 h
Treatment
Best treatment – prevention
Hydration – 3L\24h, better started 24-48 h
Stop the chemotherapy
Aggressive IV hydration / diuresis
CaCl2, NaHCO3, glucose / insulin,
Stop the chemotherapy
Aggressive IV hydration / diuresis
CaCl2, NaHCO3, glucose / insulin,
STRUCTURAL:
Neurologic emergencies
STRUCTURAL:
Neurologic emergencies
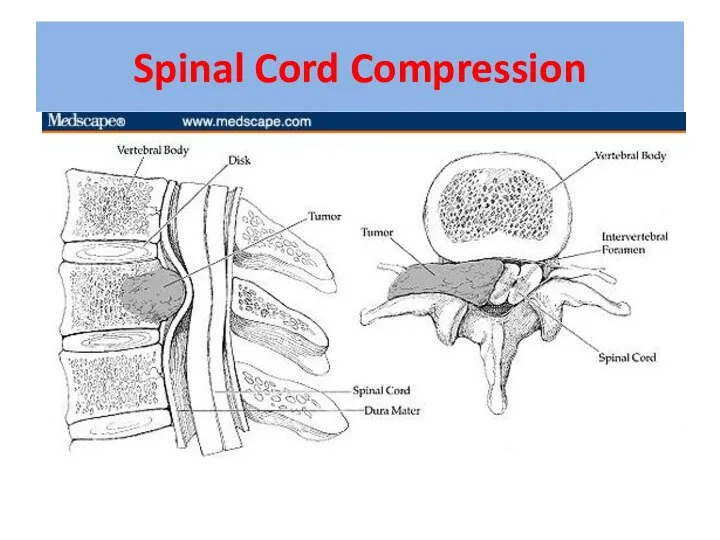
Spinal Cord Compression
Spinal Cord Compression
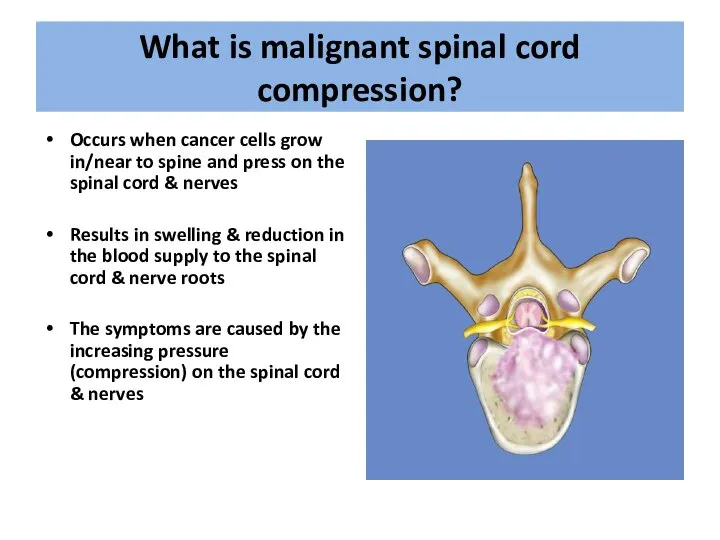
What is malignant spinal cord compression?
Occurs when cancer cells grow in/near
What is malignant spinal cord compression?
Occurs when cancer cells grow in/near
Most commonly seen in
Breast
Lung
Prostate
Lymphoma
Myeloma
About 10% of patients with cancer overall
What types
Most commonly seen in
Breast
Lung
Prostate
Lymphoma
Myeloma
About 10% of patients with cancer overall
What types
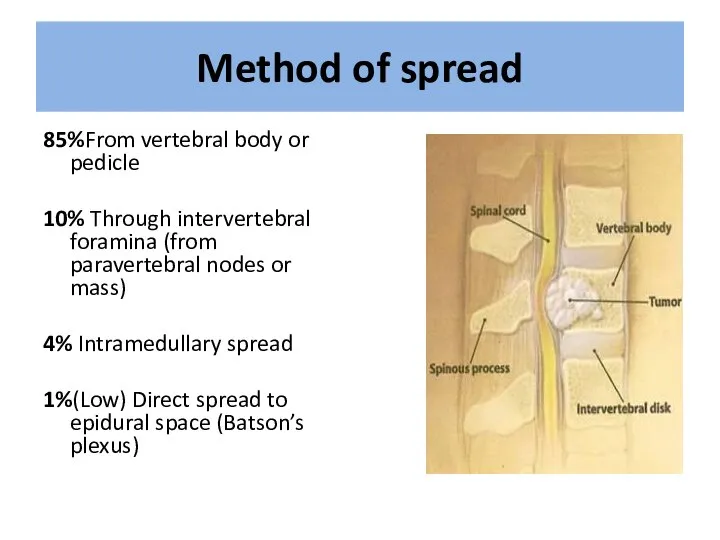
Method of spread
85%From vertebral body or pedicle
10% Through intervertebral foramina (from
Method of spread
85%From vertebral body or pedicle
10% Through intervertebral foramina (from
Location
Thoracic spine 60-70%
Lumbosacral spine 20-30%
Cervical and sacral spine less then 10%
Location
Thoracic spine 60-70%
Lumbosacral spine 20-30%
Cervical and sacral spine less then 10%
First Symptoms
Pain 95%
Weakness 5%
Ataxia 1%
Sensory loss 1%
RED FLAGS…..
First Symptoms
Pain 95%
Weakness 5%
Ataxia 1%
Sensory loss 1%
RED FLAGS…..
First Red Flag: Pain
Usually first and most common symptom
(80-90%)
Usually precedes
First Red Flag: Pain
Usually first and most common symptom
(80-90%)
Usually precedes
Second Red Flag: Motor
Weakness: 60-85%
At or above conus medularis
Extensors of the
Second Red Flag: Motor
Weakness: 60-85%
At or above conus medularis
Extensors of the
Third Red Flag: Bladder & Bowel Function
Loss is late finding
Problems passing
Third Red Flag: Bladder & Bowel Function
Loss is late finding
Problems passing
Investigations & information needed prior to therapy
MRI scan of the whole
Investigations & information needed prior to therapy
MRI scan of the whole
Treatment options include:
Immobilisation
Steroids & gastric protection
Analgesia
Surgery – decompression &
Treatment options include:
Immobilisation
Steroids & gastric protection
Analgesia
Surgery – decompression &
Indications for Surgery
• Unknown primary tumour
• Relapse post RT
• Progression while
Indications for Surgery
• Unknown primary tumour
• Relapse post RT
• Progression while
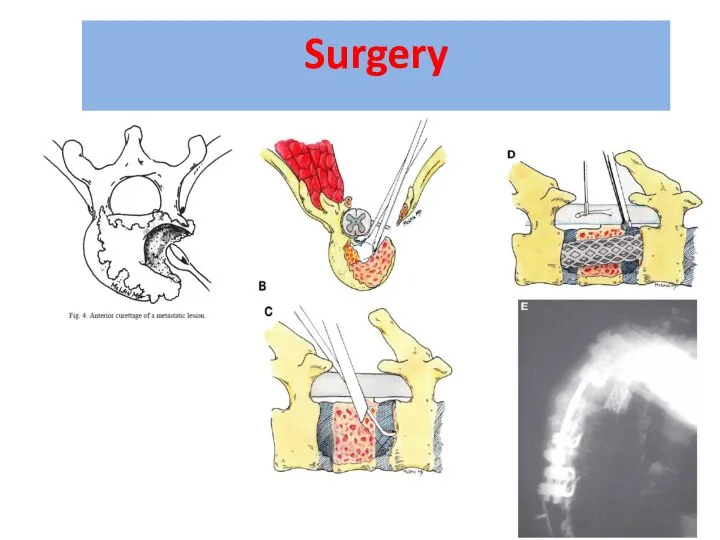
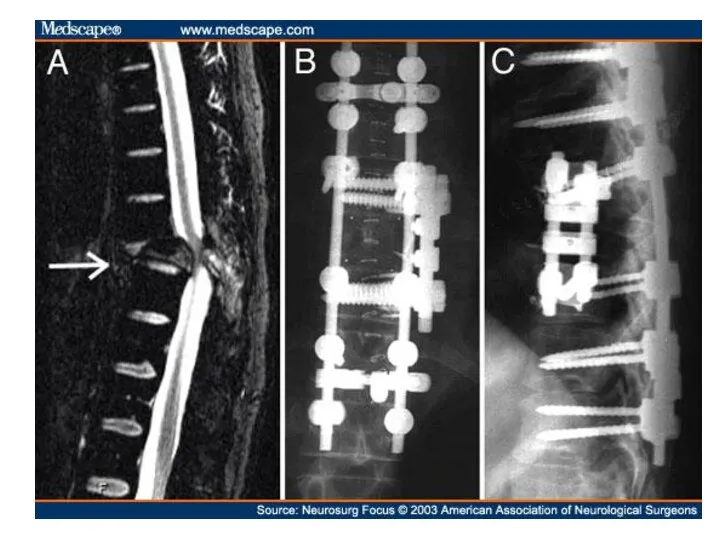
Surgery
Surgery


Improvement in surgery + RT
Days remained ambulatory (126 vs. 35)
Percent that
Improvement in surgery + RT
Days remained ambulatory (126 vs. 35)
Percent that
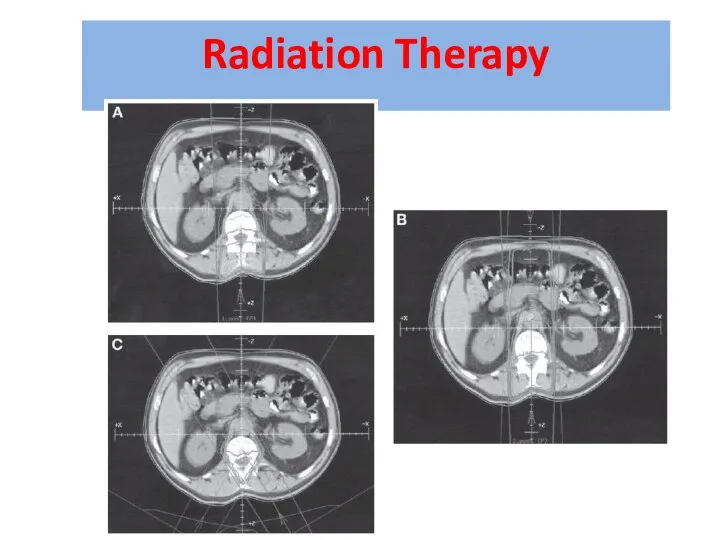
Radiation Therapy
Radiation Therapy
Prognosis
Median survival with MSCC is 6 months
Ambulatory patients with radiosensitive tumours
Prognosis
Median survival with MSCC is 6 months
Ambulatory patients with radiosensitive tumours
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome


Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
In rare cases can be disease presentation
No time for pathology
Urgent
In rare cases can be disease presentation
No time for pathology
Urgent
Exeption: Treatment Sensitive Tumors
NHLs, germ cells, and limited-stage small cell lung
Exeption: Treatment Sensitive Tumors
NHLs, germ cells, and limited-stage small cell lung
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Superior Vena Cava Syndrome
Treatment Options
Radiation therapy
Chemotherapy
Intraluminal Stent
+supportive care
Treatment Options
Radiation therapy
Chemotherapy
Intraluminal Stent
+supportive care
Supportive Care:
Rest
Head elevation
Oxygen
Diuretics
Anticoagulation
Steroids
Avoid high volume fluid infusion through upper
Supportive Care:
Rest
Head elevation
Oxygen
Diuretics
Anticoagulation
Steroids
Avoid high volume fluid infusion through upper
Intraluminal Stents
Endovascular placement under fluoroscopy
Patients who have recurrent disease in previously
Intraluminal Stents
Endovascular placement under fluoroscopy
Patients who have recurrent disease in previously
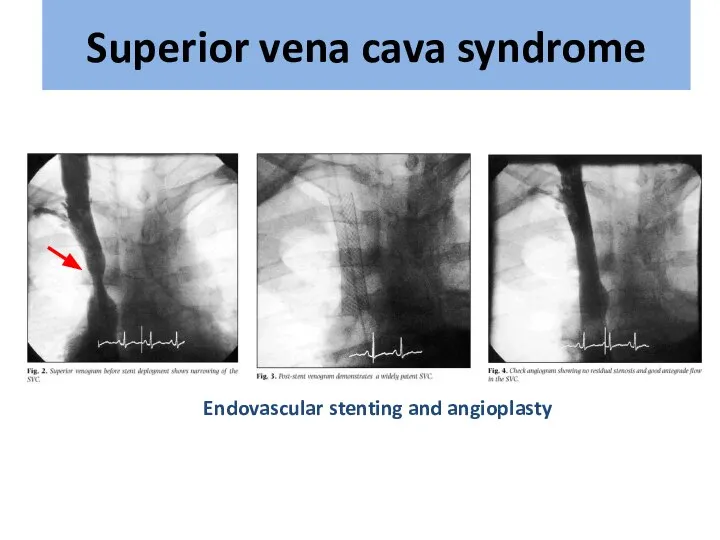
Endovascular stenting and angioplasty
Superior vena cava syndrome
Endovascular stenting and angioplasty
Superior vena cava syndrome
Most Common type of CNS malignancy
20-40% of cancer patients will develop
Most Common type of CNS malignancy
20-40% of cancer patients will develop
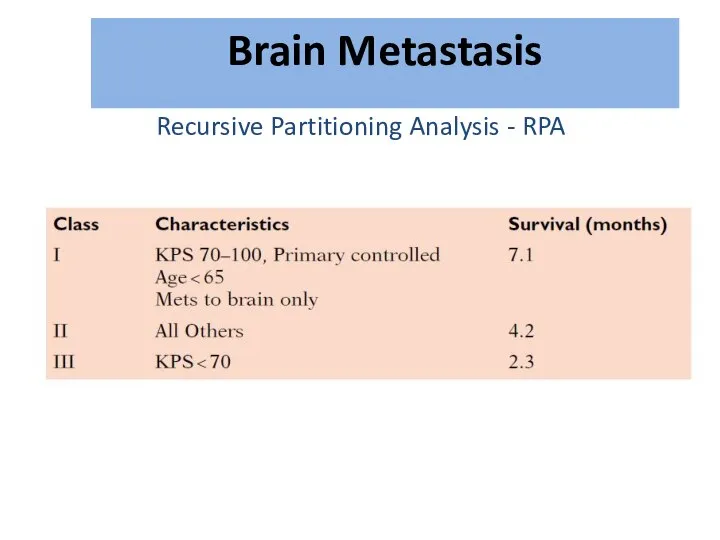
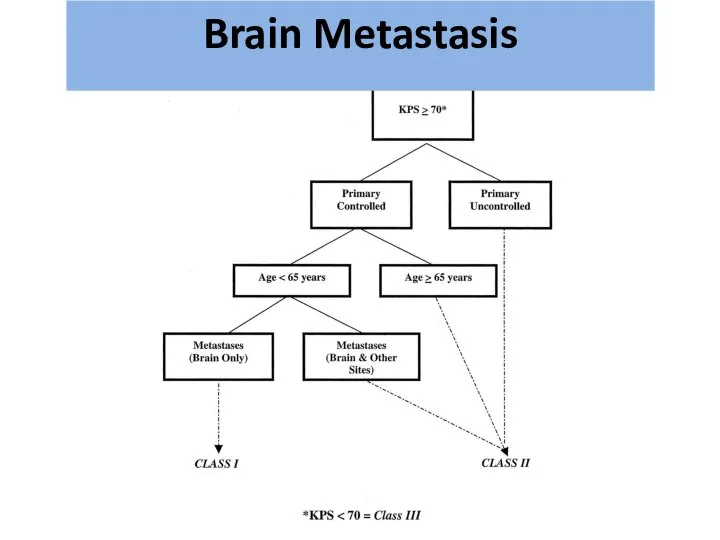
Recursive Partitioning Analysis - RPA
גרורות מוחיות
Brain Metastasis
Recursive Partitioning Analysis - RPA
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
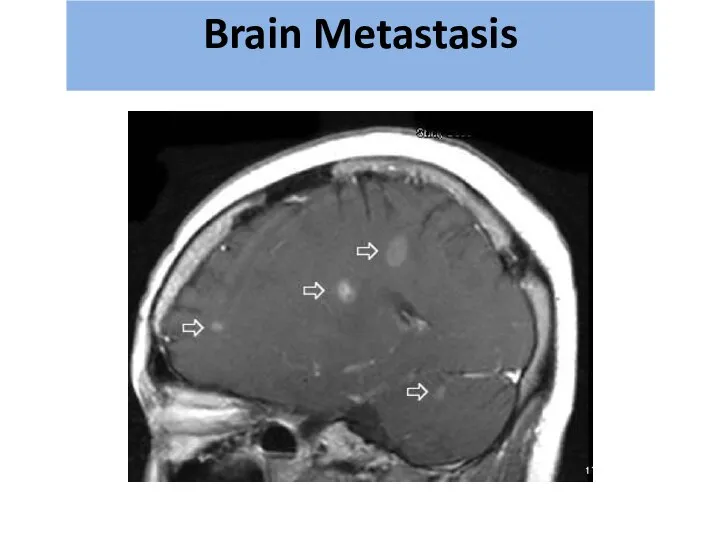
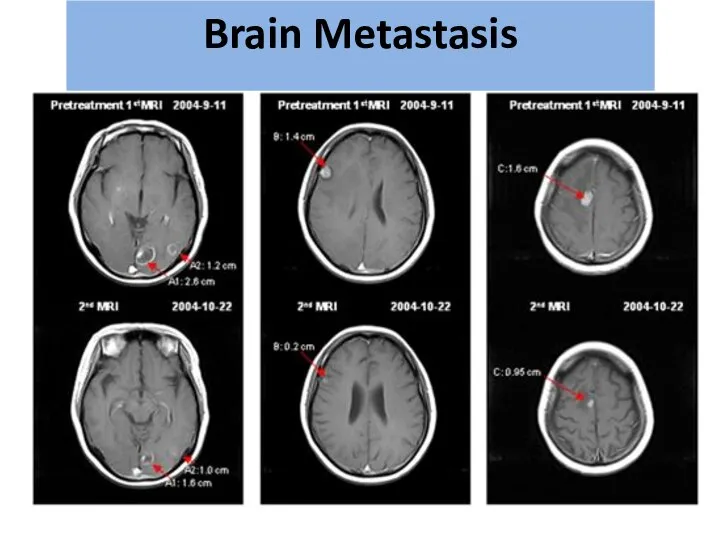
Diagnosis:
CT with and without contrast
MRI – modality of choice for small
Diagnosis:
CT with and without contrast
MRI – modality of choice for small
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
Treatment:
Steroids – Dexamethasone 16mg*2
Anticonvulsant
Surgery?
Radiation therapy
גרורות מוחיות
Brain Metastasis
Treatment:
Steroids – Dexamethasone 16mg*2
Anticonvulsant
Surgery?
Radiation therapy
גרורות מוחיות
Brain Metastasis
Radiation therapy
WBRT=Whole Brain RT
SRS=Stereotactic Radio Surgery
גרורות מוחיות
Brain Metastasis
Radiation therapy
WBRT=Whole Brain RT
SRS=Stereotactic Radio Surgery
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
German
Helmet
Brain Metastasis
גרורות מוחיות
German
Helmet
Brain Metastasis
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
SRS
SRS
גרורות מוחיות
Brain Metastasis
גרורות מוחיות
Brain Metastasis
 Христианская церковь в раннее Средневековья
Христианская церковь в раннее Средневековья Станок Нартова 1 часть
Станок Нартова 1 часть Машины для разметки покрытий, содержания обстановки, озеленения и благоустройства дорог
Машины для разметки покрытий, содержания обстановки, озеленения и благоустройства дорог Prezentatsiya_Metodi_v_filosofiyi_Talashov_Yegor_Volodimirovich
Prezentatsiya_Metodi_v_filosofiyi_Talashov_Yegor_Volodimirovich Инновационный подход к контрольно-оценочной деятельности в начальной школе. Портфолио
Инновационный подход к контрольно-оценочной деятельности в начальной школе. Портфолио 20170604_teatr_zadach
20170604_teatr_zadach Презентация Mой прадед Михайлов НГ
Презентация Mой прадед Михайлов НГ Три ступени, ведущие вниз
Три ступени, ведущие вниз Виды профилей. Прокатка. Прессование. Волочени
Виды профилей. Прокатка. Прессование. Волочени День самоуправления в школе
День самоуправления в школе Я здоровье сберегу, сам себе я помогу
Я здоровье сберегу, сам себе я помогу H480 Harvester Head Training Material
H480 Harvester Head Training Material Иконы, фрески, роспись церкви
Иконы, фрески, роспись церкви 20130304_35_ur_lit.5kl._obraz_rodiny_v_stihah_poetov_19v
20130304_35_ur_lit.5kl._obraz_rodiny_v_stihah_poetov_19v Работа над метроритмом размер 4/4
Работа над метроритмом размер 4/4 Досуговый центр
Досуговый центр Македония
Македония 0702А102_Тучкова М.Е
0702А102_Тучкова М.Е Оборудование отсеков и системы разгрузки танкера дедвейтом 3800т
Оборудование отсеков и системы разгрузки танкера дедвейтом 3800т Как читать молитву Отче наш
Как читать молитву Отче наш Подобие в жизни человека и немного юмора
Подобие в жизни человека и немного юмора Личная карточка инструктажа по безопасным методам работы, промсанитарии и противопожарной безопасности
Личная карточка инструктажа по безопасным методам работы, промсанитарии и противопожарной безопасности эрудит-викторина
эрудит-викторина Как зернышко на стол хлебом пришло
Как зернышко на стол хлебом пришло Моделирование
Моделирование ПромежуточнаяЗащита_2
ПромежуточнаяЗащита_2 Викторина. Где логика
Викторина. Где логика Система авто-полива сада
Система авто-полива сада