- Acute mediastinitis. Lection for students of 5 course

Содержание
- 2. Acute mediastinitis is most often the result of bacterial infection of the mediastinum. Mediastinitis may be
- 3. Causes acute mediastinitis The most common cause is oesophageal perforation. Esophageal perforation may complicate esophagoscopy or
- 4. Causes acute mediastinitis The other causes that are much less common include: postoperative infection, particularly following
- 5. Symptoms patients present with chills chest pain high fever tachycardia
- 6. Diagnostic Chest radiography may show mediastinalChest radiography may show mediastinal widening and findings of mediastinal abscess
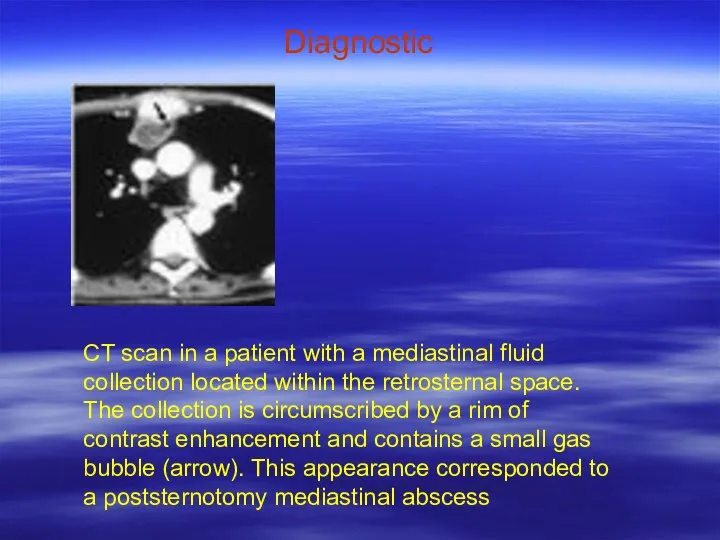
- 7. Diagnostic CT scan in a patient with a mediastinal fluid collection located within the retrosternal space.
- 8. Complications of mediastinitis Abscess formation Empyema Esophagocutaneous fistulas Sternal osteomyelitis Pericardial tamponade
- 9. Complications of mediastinitis Common complications of mediastinitis result from extension of the infectious process into contiguous
- 10. Complications of mediastinitis Pericardial effusion and subsequent tamponade can result from direct extension of the infectious
- 11. Complications of mediastinitis diagnostic Echocardiography demonstrated a moderate to large circumferential pericardial effusion. Pericardiocentesis was subsequently
- 12. Complications of mediastinitis diagnostic Laboratory analysis of the recovered fluid revealed pericardial and pleural exudates, with
- 13. Treatment open surgical drainage and débridement are necessary to prevent serious morbidity and mortality. The importance
- 14. Treatment Percutaneous catheter drainage has been used in less urgent clinical settings, often as a temporizing
- 15. Treatment The patient underwent an open thoracotomy with drainage and removal of right paratracheal and subcarinal
- 17. Скачать презентацию
Acute mediastinitis
is most often the result of bacterial infection
of the
Acute mediastinitis
is most often the result of bacterial infection
of the
Causes acute mediastinitis
The most common cause is oesophageal perforation.
Esophageal perforation
Causes acute mediastinitis
The most common cause is oesophageal perforation.
Esophageal perforation

Causes acute mediastinitis
The other causes that are much less common include:
Causes acute mediastinitis
The other causes that are much less common include:

Symptoms
patients present with chills
chest pain
high fever
tachycardia
Symptoms
patients present with chills
chest pain
high fever
tachycardia
Diagnostic
Chest radiography may show mediastinalChest radiography may show mediastinal widening and
Diagnostic
Chest radiography may show mediastinalChest radiography may show mediastinal widening and
Diagnostic
CT scan in a patient with a mediastinal fluid collection located
Diagnostic
CT scan in a patient with a mediastinal fluid collection located

Complications of mediastinitis
Abscess formation
Empyema
Esophagocutaneous fistulas
Sternal osteomyelitis
Pericardial tamponade
Complications of mediastinitis
Abscess formation
Empyema
Esophagocutaneous fistulas
Sternal osteomyelitis
Pericardial tamponade
Complications of mediastinitis
Common complications of mediastinitis result from extension of the
Complications of mediastinitis
Common complications of mediastinitis result from extension of the
Complications of mediastinitis
Pericardial effusion and subsequent tamponade can result from direct
Complications of mediastinitis
Pericardial effusion and subsequent tamponade can result from direct
Complications of mediastinitis
diagnostic
Echocardiography demonstrated a moderate to large circumferential pericardial
Complications of mediastinitis
diagnostic
Echocardiography demonstrated a moderate to large circumferential pericardial

Complications of mediastinitis
diagnostic
Laboratory analysis of the recovered fluid revealed pericardial and
Complications of mediastinitis
diagnostic
Laboratory analysis of the recovered fluid revealed pericardial and
Treatment
open surgical drainage and débridement are necessary to prevent serious morbidity
Treatment
open surgical drainage and débridement are necessary to prevent serious morbidity
Treatment
Percutaneous catheter drainage has been used in less urgent clinical settings,
Treatment
Percutaneous catheter drainage has been used in less urgent clinical settings,

Treatment
The patient underwent an open thoracotomy with drainage and removal of
Treatment
The patient underwent an open thoracotomy with drainage and removal of
 Exercises
Exercises A tour around my home city Anzhero-Sudzhensk
A tour around my home city Anzhero-Sudzhensk Present Perfect УМК К.И. Кауфман, 7 класс “Happy English.ru” Левченко Наталья Владимировна, МОУ СОШ 14 с. Заветное 2012г.
Present Perfect УМК К.И. Кауфман, 7 класс “Happy English.ru” Левченко Наталья Владимировна, МОУ СОШ 14 с. Заветное 2012г. Monuments to World War I in Russia
Monuments to World War I in Russia Topic: Bitcoin
Topic: Bitcoin Have you ever faced any rocket science tasks/challenges at work?
Have you ever faced any rocket science tasks/challenges at work? A synopsis is a brief summary of a written work or a movie..
A synopsis is a brief summary of a written work or a movie..  How to write an essay
How to write an essay DOTTY THE DOG AND HIS FRIENDS.
DOTTY THE DOG AND HIS FRIENDS. Van Gogh Museum
Van Gogh Museum В замке герцога to Be
В замке герцога to Be Stylistics of the English Language 8. Morphological Expressive Means Outline
Stylistics of the English Language 8. Morphological Expressive Means Outline СТРАДАТЕЛЬНЫЙ ЗАЛОГ PASSIVE VOICE
СТРАДАТЕЛЬНЫЙ ЗАЛОГ PASSIVE VOICE Items and actions
Items and actions Презентация к уроку английского языка “Applying for a job” (Writing a letter of application) для 9 класса. УMK Биболетовой М. З. Учитель английского языка МБОУ гимназии №19 имени Н.З.Поповичевой г. Липецка Жаглина Татьяна Владимировна.
Презентация к уроку английского языка “Applying for a job” (Writing a letter of application) для 9 класса. УMK Биболетовой М. З. Учитель английского языка МБОУ гимназии №19 имени Н.З.Поповичевой г. Липецка Жаглина Татьяна Владимировна. Конструкция Used to
Конструкция Used to МУНИЦИПАЛЬНОЕ БЮДЖЕТНОЕ ОБЩЕОБРАЗОВАТЕЛЬНОЕ УЧРЕЖДЕНИЕ СРЕДНЯЯ ОБЩЕОБРАЗОВАТЕЛЬНАЯ ШКОЛА № 45 СТАНИЦЫ СЕВЕРСКОЙ МУНИЦИПАЛЬНОГО
МУНИЦИПАЛЬНОЕ БЮДЖЕТНОЕ ОБЩЕОБРАЗОВАТЕЛЬНОЕ УЧРЕЖДЕНИЕ СРЕДНЯЯ ОБЩЕОБРАЗОВАТЕЛЬНАЯ ШКОЛА № 45 СТАНИЦЫ СЕВЕРСКОЙ МУНИЦИПАЛЬНОГО Time & clocks
Time & clocks Summer course
Summer course Saul Bellow 1915 – 2005
Saul Bellow 1915 – 2005 Презентация к уроку английского языка "Kite skiing" - скачать
Презентация к уроку английского языка "Kite skiing" - скачать  Экскурсия по Бонну Бонн-это город культуры и традиций, город, который гордится тем, что здесь родился композитор Людвиг ван Бетхов
Экскурсия по Бонну Бонн-это город культуры и традиций, город, который гордится тем, что здесь родился композитор Людвиг ван Бетхов You are what you eat
You are what you eat My ideal school Prepared by the pupil of the 11th form Holub Margaryta
My ideal school Prepared by the pupil of the 11th form Holub Margaryta  DOUBLE-DECKER BUSES
DOUBLE-DECKER BUSES Squick Thesis
Squick Thesis Perfekt ПРОСТОЕ ПРОШЕДШЕЕ ВРЕМЯ
Perfekt ПРОСТОЕ ПРОШЕДШЕЕ ВРЕМЯ Презентация к уроку английского языка "Национальные кухни на английском" - скачать бесплатно
Презентация к уроку английского языка "Национальные кухни на английском" - скачать бесплатно