- Cardiovascular disease In pregnancy

Содержание
- 2. Cardiac Diseases Rheumatic heart disease Congenital heart disease Hypertensive heart disease Coronary Thyroid Syphilitic Kyphoscoliotic cardiac
- 3. Physiological Consideration with Heart Disease In Pregnancy The most important changes in cardiac function occurs in
- 4. cont… Later in pregnancy COP is higher when women is in the lateral recumbent position than
- 5. cont… Heart: The heart is displaced upward and to the left with lateral rotation on its
- 6. conti…. Systolic murmur is heard in 90 % of cases Soft diastolic murmur transiently in 20
- 7. Diagnosis of Heart Disease Some clinical indicators of heart disease during Pregnancy Symptoms: Progressive dyspnea or
- 8. Clinical findings Cyanosis Clubbing of fingers persistent neck vein distension Systolic murmur grade 3/6 or greater
- 9. Diagnostic studies Electrocardiography An average 15 – degree left – axis deviation in the ECG ,
- 10. Echocardiography: Normal changes include : Tricuspid regurgitation , Significantly increase left atrial size and left ventricular
- 11. Clinical clssification The New York Heart Association’s Functional Classification [ NYHA] “ First published in 1928
- 12. Preconceptional counseling Maternal mortality generally varies directly with functional classification at pregnancy onset; However this relationship
- 13. cont… Life threatening cardiac abnormalities can be reversed by corrective surgery and subsequent pregnancy is less
- 14. Risks for Maternal Mortality Caused by Various Heart Disease Cardiac Disorder Mortality % Group 1 –
- 15. Group 2 – Moderate Risk 5 -15 % 2A : Mitral stenosis , NYHA classes 3
- 16. Group 3 – Major Risk 25 -50 % Pulmonary hypertension Aortic coarctation with valvar involvement Marfan
- 17. Management In assuring an optimal outcome , management should be a team approach involving ;obstetrician, cardiologist
- 18. Management Four concepts that affect management are emphasized by the American College of Obs /Gyn :-
- 19. Management of Class 1 & 2 General measures: _ avoid contact with persons who have respiratory
- 20. management cont….. sign’s of heart failure: » persistent basilar rales » nocturnal cough » a sudden
- 21. Management cont….. Labor and Delivery : * vaginal delivery is preferred unless there is obstetrical indication
- 22. * fluid balance and antibiotic prophylactic * semi recumbent position with lateral tilt * intensive medical
- 23. puerperium * avoid complication of pph, anemia, infection and thromboembolism * delay the procedure of tubal
- 24. Management of class 3&4 ؟ whether pregnancy should be undertaken ؟ consider pregnancy interruption ؟ prolonged
- 25. Most common lesions: _Rheumatic heart disease Incidence of rheumatic fever is decreasing in developed countries ,
- 26. Peripartum cardiomyopathy : this is a diagnosis of exclusion , it describe women with peripartum heart
- 28. Скачать презентацию
Cardiac Diseases
Rheumatic heart disease
Congenital heart disease
Hypertensive heart disease
Coronary
Thyroid
Syphilitic
Kyphoscoliotic cardiac disease
Idiopathic
Cardiac Diseases
Rheumatic heart disease
Congenital heart disease
Hypertensive heart disease
Coronary
Thyroid
Syphilitic
Kyphoscoliotic cardiac disease
Idiopathic
Physiological Consideration with Heart Disease In Pregnancy
The most important changes
Physiological Consideration with Heart Disease In Pregnancy
The most important changes
cont…
Later in pregnancy COP is higher when women is
cont…
Later in pregnancy COP is higher when women is
cont…
Heart:
The heart is displaced upward and to the
cont…
Heart:
The heart is displaced upward and to the
conti….
Systolic murmur is heard in 90 % of cases
conti….
Systolic murmur is heard in 90 % of cases
Diagnosis of Heart Disease
Some clinical indicators of heart disease during
Pregnancy
Diagnosis of Heart Disease
Some clinical indicators of heart disease during
Pregnancy

Clinical findings
Cyanosis
Clubbing of fingers
persistent neck vein
Clinical findings
Cyanosis
Clubbing of fingers
persistent neck vein
Diagnostic studies
Electrocardiography
An average 15 – degree left – axis deviation
Diagnostic studies
Electrocardiography
An average 15 – degree left – axis deviation
Echocardiography:
Normal changes include : Tricuspid regurgitation ,
Significantly increase left
Echocardiography:
Normal changes include : Tricuspid regurgitation ,
Significantly increase left
![Clinical clssification The New York Heart Association’s Functional Classification [ NYHA]](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/502270/slide-10.jpg)
Clinical clssification
The New York Heart Association’s Functional
Classification [ NYHA]
Clinical clssification
The New York Heart Association’s Functional
Classification [ NYHA]
Preconceptional counseling
Maternal mortality generally varies directly with
functional classification at
Preconceptional counseling
Maternal mortality generally varies directly with
functional classification at
cont…
Life threatening cardiac abnormalities can be reversed
by
cont…
Life threatening cardiac abnormalities can be reversed
by
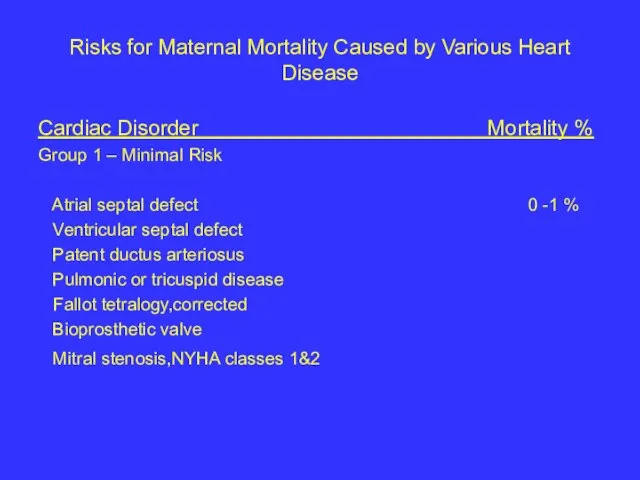
Risks for Maternal Mortality Caused by Various Heart Disease
Cardiac Disorder
Risks for Maternal Mortality Caused by Various Heart Disease
Cardiac Disorder
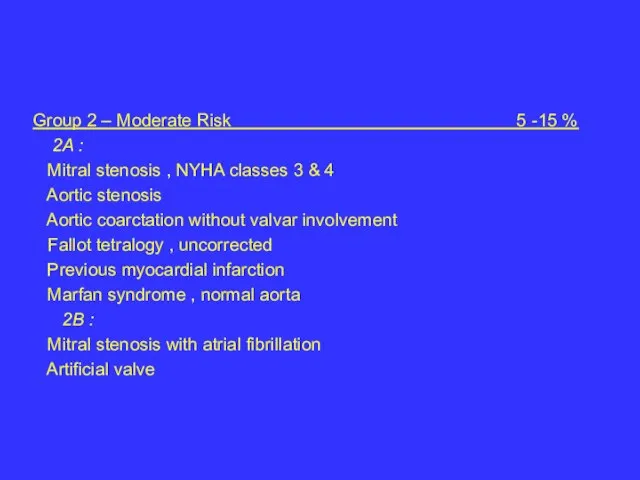
Group 2 – Moderate Risk 5 -15 %
2A :
Mitral
Group 2 – Moderate Risk 5 -15 %
2A :
Mitral
Group 3 – Major Risk 25 -50 %
Pulmonary hypertension
Group 3 – Major Risk 25 -50 %
Pulmonary hypertension

Management
In assuring an optimal outcome , management should
Management
In assuring an optimal outcome , management should
Management
Four concepts that affect management are emphasized
by the American
Management
Four concepts that affect management are emphasized
by the American
Management of Class 1 & 2
General measures:
_ avoid contact with
Management of Class 1 & 2
General measures:
_ avoid contact with
management cont…..
sign’s of heart failure:
» persistent basilar rales
management cont…..
sign’s of heart failure:
» persistent basilar rales
Management cont…..
Labor and Delivery :
* vaginal delivery is preferred
Management cont…..
Labor and Delivery :
* vaginal delivery is preferred

* fluid balance and antibiotic prophylactic
* semi recumbent position
* fluid balance and antibiotic prophylactic
* semi recumbent position
puerperium
* avoid complication of pph, anemia, infection
and
puerperium
* avoid complication of pph, anemia, infection
and
Management of class 3&4
؟ whether pregnancy should be undertaken
؟
Management of class 3&4
؟ whether pregnancy should be undertaken
؟
Most common lesions:
_Rheumatic heart disease
Incidence of rheumatic fever
Most common lesions:
_Rheumatic heart disease
Incidence of rheumatic fever
Peripartum cardiomyopathy :
this is a diagnosis of exclusion , it
Peripartum cardiomyopathy :
this is a diagnosis of exclusion , it
 Узкий и клинически узкий таз в современном акушерстве
Узкий и клинически узкий таз в современном акушерстве Фармакоэпидемиология. Главные задачи фармакоэпидемиологических исследований
Фармакоэпидемиология. Главные задачи фармакоэпидемиологических исследований Вирусные дерматозы
Вирусные дерматозы Сарысудағы белокты электрофоретикалық патологиялық талдау
Сарысудағы белокты электрофоретикалық патологиялық талдау Хроническая обструктивная болезнь лёгких
Хроническая обструктивная болезнь лёгких Современные возможности лечения мигрени
Современные возможности лечения мигрени Женские и мужские половые гормоны
Женские и мужские половые гормоны Психічні пізнавальні процеси особистості військовослужбовця, його емоційно-волева сфера, психічні стани та утворення
Психічні пізнавальні процеси особистості військовослужбовця, його емоційно-волева сфера, психічні стани та утворення ЛФК при заболеваниях сердечно-сосудистой системы. Инфаркт миокарда
ЛФК при заболеваниях сердечно-сосудистой системы. Инфаркт миокарда Особенности копинг-стратегий подростков, входящих в группу суицидального риска
Особенности копинг-стратегий подростков, входящих в группу суицидального риска Двигательная сфера. Методы исследования
Двигательная сфера. Методы исследования Фармакодинамика
Фармакодинамика Сүт және сүт өнiмдерiн өндіру технологиясы мен малдәрiгерлiк санитариялық сараптау
Сүт және сүт өнiмдерiн өндіру технологиясы мен малдәрiгерлiк санитариялық сараптау Endometriosis
Endometriosis Ультрафиолетовая недостаточность, ее проявления и профилактика
Ультрафиолетовая недостаточность, ее проявления и профилактика Шизоаффективный психоз
Шизоаффективный психоз Воспаление. Острое воспаление
Воспаление. Острое воспаление Технология приготовления, состав и свойства ситаллов. Назначение в стоматологии
Технология приготовления, состав и свойства ситаллов. Назначение в стоматологии Қант диабеті. Жүктілік кезіндегі қант диабеті. Тамақтану ерекшеліктері
Қант диабеті. Жүктілік кезіндегі қант диабеті. Тамақтану ерекшеліктері Поставь на стрессе точку
Поставь на стрессе точку Физиологиялық зерттеу әдістері
Физиологиялық зерттеу әдістері Правовое обеспечение оказания медицинской услуги Катетеризация подключичной и других центральных вен
Правовое обеспечение оказания медицинской услуги Катетеризация подключичной и других центральных вен Бульбарный и псевдобульбарный синдромы
Бульбарный и псевдобульбарный синдромы Методы лечения аномалий прикуса в периоде смешанных зубах
Методы лечения аномалий прикуса в периоде смешанных зубах Эндовидеолапароскопические операции при опухолях желудка и ободочной кишки
Эндовидеолапароскопические операции при опухолях желудка и ободочной кишки Ультразвуковое исследование поджелудочной железы
Ультразвуковое исследование поджелудочной железы Заболеваемость. Расчет показателя заболеваемости
Заболеваемость. Расчет показателя заболеваемости Medical control over organization and full value of individual nutrition and nutrition
Medical control over organization and full value of individual nutrition and nutrition