- Endometriosis

Содержание
- 2. DEFINITION Presence of endometrial tissue (both glands & stroma) outside the uterus. Tissue is
- 3. AETIOLOGY: theories Sampson’s theory of menstrual regurgitation and implantation (Metastatic theory) Retrograde menstruation ↓ Endometrial fragments
- 5. Coelomic metaplasia theory: Original Coelomic membrane transforms into endometrial tissue. Explains endometriosis in ectopic sites. Lymphatic
- 6. 4. Immunological factors: reduced clearance of endometrial cells due to decreased natural killer cell activity or
- 7. SITES
- 8. TYPES OF ENDOMETRIOSIS PELVIC ENDOMETRIOSIS EXTRA PELVIC ENDOMETRIOSIS Peritoneal Gastrointestinal tract Ovarian Urinary tract Deep infiltrating
- 9. CLINICAL PRESENTATION PAIN: Classical triad: dysmenorrhea, dyspareunia & deep seated pelvic pain. Commence before onset of
- 10. ABNORMAL BLEEDING: May include premenstrual spotting, polymenorrhoea & menometrorrhagia. INFERTILITY: Present in majority of the women
- 11. OTHER SYMPTOMS Extrapelvic endometriosis: cyclical rectal bleeding or hematuria. Scar endometriosis: cyclical pain and bleeding at
- 12. SIGNS & SYMPTOMS SIGNS Tenderness in cul-de-sac Nodularity in cul-de-sac Fixed retroverted uterus Adnexal tenderness Adnexal
- 13. INVESTIGATIONS
- 14. TRANSVAGINAL ULTRASOUND SCAN Retroverted uterus with obliteration of cul-de-sac & B\L complex adnexal masses maybe suggestive.
- 15. CA-125 Increased in moderate to severe endometriosis Also increased in non-mucinous epithelial ovarian cancers.
- 16. LAPAROSCOPY Gold Standard During laparoscopy, entire pelvis should be examined systematically in clockwise or counterclockwise direction.
- 17. 1. PERITONEAL LESION CLASSIC LESIONS: Powder burn or gunshot lesion: black to dark brown nodules consisting
- 18. 2. OVARIAN ENDOMETRIOSIS ENDOMETRIOMA OE CHOCOLATE CYST: Cyst contains thick tarry fluid- chocolate fluid – derived
- 19. 3. DEEP INFILTRATING ENDOMETRIOSIS Lesions are usually in rectovaginal space. May involve uterosacral ligaments, cervix, bowel
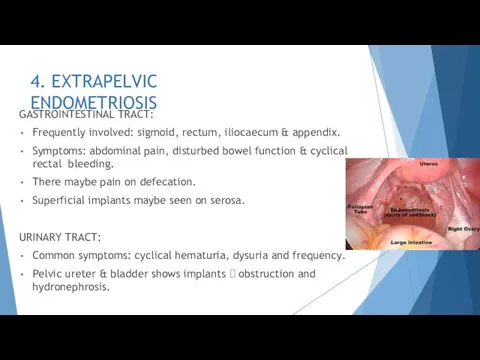
- 20. 4. EXTRAPELVIC ENDOMETRIOSIS GASTROINTESTINAL TRACT: Frequently involved: sigmoid, rectum, iliocaecum & appendix. Symptoms: abdominal pain, disturbed
- 21. Extrapelvic endometriosis cont. SCAR ENDOMETRIOSIS: Seen at umbilicus, port sites following laparoscopy, abdominal incisions following cesarean
- 22. INVESTIGATIONS CT & MRI: Identical picture as in USG COLOUR DOPPLER FLOW: Increased vascularity CYSTOSCOPY: Involvement
- 23. HISTOLOGY Histologic confirmation is essential. On microscopy, typical endometrial implant with endometrial glands &
- 24. CLASSIFICATION OF ENDOMETRIOSIS Stage I: MINIMAL: Score 1-5 Small spots of endometriosis seen at laparoscopy, but
- 25. Stage IV: SEVERE: Score >40 Endometriomas exceed 2cm. Dense Peritubal & periovarian adhesions restrict motility. Thickened
- 26. DIFFEERENTIAL DIAGNOSIS Chronic PID Postoperative adhesions Old ectopic gestation Pelvic congestion syndrome Irritable bowel syndrome Diverticulitis
- 27. MANAGEMENT
- 28. Management of Endometriosis Asymptomatic minimal endometriosis Observe 6-8 months, Investigate infertility Symptomatic cases Drug treatment Minimal
- 29. DRUG TREATMENT Combined oral contraceptives: Administered intermittently or continuously. High Incidence of side effects & risk
- 30. DRUG TREATMENT Danazol A synthetic derivative of ethinyl testosterone, Mildly anabolic , anti-oestrogenic and anti-progestational 200-800mg
- 31. Drug treatment Gonadotropin releasing hormone: GnRH is administered continuously to down regulate and suppress pituitary gonadotropins
- 32. DRUG THERAPY Failure of drug therapy is due to : Drug cannot penetrate fibrotic capsule. Ectopic
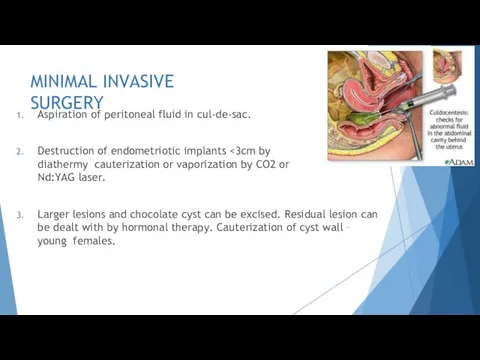
- 33. MINIMAL INVASIVE SURGERY Aspiration of peritoneal fluid in cul-de-sac. Destruction of endometriotic implants Larger lesions and
- 34. MINIMAL INVASIVE SURGERY Role of surgery: Failed Medical therapy Infertility Recurrence Chocolate
- 35. SURGERY Indications for surgery: Advanced stage of disease detected Large lesion Medical therapy
- 36. SURGERY Laparotomy: In advanced & larger lesions if medical therapy fails. Dissection and excision of a
- 37. COMBINED THERAPY Preoperative GnRH: monthly for 3 months reduces size & extend of lesions, softens adhesions
- 38. PROPHYLAXIS Low-dose OCP reduce the menstrual flow & protect against endometriosis. 3 monthly OCP’s are convenient
- 40. Скачать презентацию
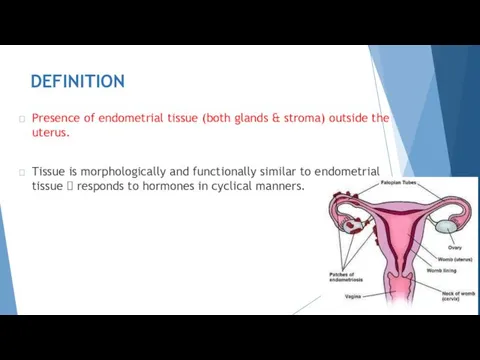
DEFINITION
Presence of endometrial tissue (both glands & stroma) outside the uterus.
Tissue
DEFINITION
Presence of endometrial tissue (both glands & stroma) outside the uterus.
Tissue
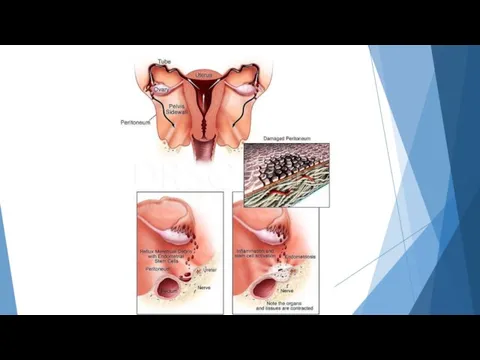
AETIOLOGY: theories
Sampson’s theory of menstrual regurgitation and implantation (Metastatic theory)
Retrograde menstruation
↓
Endometrial
AETIOLOGY: theories
Sampson’s theory of menstrual regurgitation and implantation (Metastatic theory)
Retrograde menstruation
↓
Endometrial
Coelomic metaplasia theory:
Original Coelomic membrane transforms into endometrial tissue.
Explains endometriosis in
Coelomic metaplasia theory:
Original Coelomic membrane transforms into endometrial tissue.
Explains endometriosis in
4. Immunological factors: reduced clearance of endometrial cells due to decreased natural
4. Immunological factors: reduced clearance of endometrial cells due to decreased natural
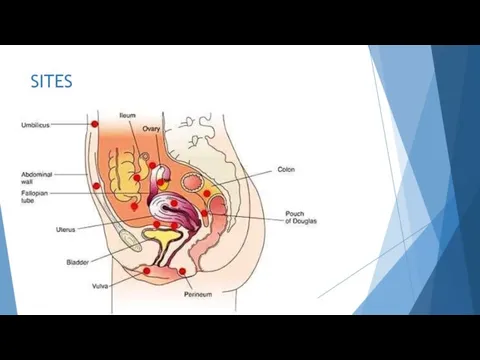
SITES
SITES
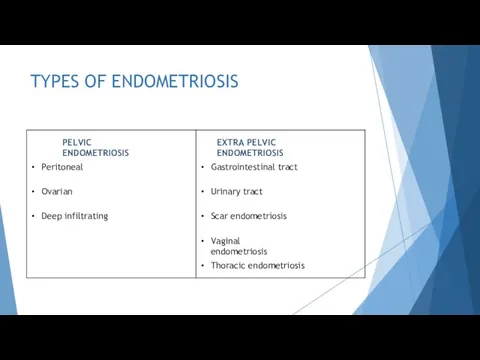
TYPES OF ENDOMETRIOSIS
PELVIC ENDOMETRIOSIS
EXTRA PELVIC ENDOMETRIOSIS
Peritoneal
Gastrointestinal tract
Ovarian
Urinary tract
Deep infiltrating
Scar endometriosis
Vaginal endometriosis
Thoracic
TYPES OF ENDOMETRIOSIS
PELVIC ENDOMETRIOSIS
EXTRA PELVIC ENDOMETRIOSIS
Peritoneal
Gastrointestinal tract
Ovarian
Urinary tract
Deep infiltrating
Scar endometriosis
Vaginal endometriosis
Thoracic
CLINICAL PRESENTATION
PAIN:
Classical triad: dysmenorrhea, dyspareunia & deep seated pelvic pain.
Commence before
CLINICAL PRESENTATION
PAIN:
Classical triad: dysmenorrhea, dyspareunia & deep seated pelvic pain.
Commence before
ABNORMAL BLEEDING:
May include premenstrual spotting, polymenorrhoea & menometrorrhagia.
INFERTILITY:
Present in majority of
ABNORMAL BLEEDING:
May include premenstrual spotting, polymenorrhoea & menometrorrhagia.
INFERTILITY:
Present in majority of
OTHER SYMPTOMS
Extrapelvic endometriosis: cyclical rectal bleeding or hematuria.
Scar endometriosis: cyclical pain
OTHER SYMPTOMS
Extrapelvic endometriosis: cyclical rectal bleeding or hematuria.
Scar endometriosis: cyclical pain
SIGNS & SYMPTOMS
SIGNS
Tenderness in cul-de-sac
Nodularity in cul-de-sac
Fixed retroverted uterus
Adnexal tenderness
Adnexal masses
SYMPTOMS
Dysmenorrhoea
Dyspareunia
Deep
SIGNS & SYMPTOMS
SIGNS
Tenderness in cul-de-sac
Nodularity in cul-de-sac
Fixed retroverted uterus
Adnexal tenderness
Adnexal masses
SYMPTOMS
Dysmenorrhoea
Dyspareunia
Deep

INVESTIGATIONS
INVESTIGATIONS
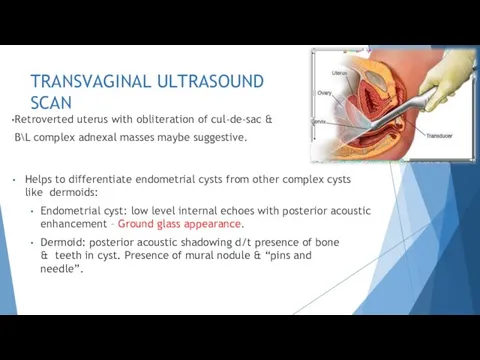
TRANSVAGINAL ULTRASOUND SCAN
Retroverted uterus with obliteration of cul-de-sac & B\L complex
TRANSVAGINAL ULTRASOUND SCAN
Retroverted uterus with obliteration of cul-de-sac & B\L complex

CA-125
Increased in moderate to severe endometriosis
Also increased in non-mucinous epithelial ovarian
CA-125
Increased in moderate to severe endometriosis
Also increased in non-mucinous epithelial ovarian
LAPAROSCOPY
Gold Standard
During laparoscopy, entire pelvis should be examined systematically in clockwise
LAPAROSCOPY
Gold Standard
During laparoscopy, entire pelvis should be examined systematically in clockwise
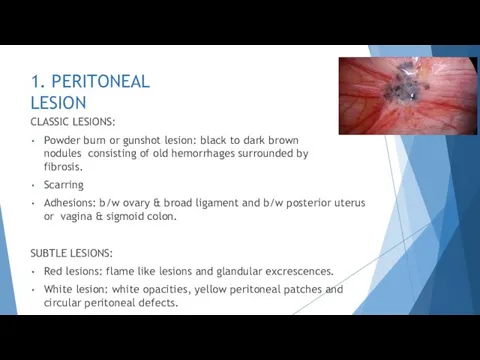
1. PERITONEAL LESION
CLASSIC LESIONS:
Powder burn or gunshot lesion: black to dark
1. PERITONEAL LESION
CLASSIC LESIONS:
Powder burn or gunshot lesion: black to dark
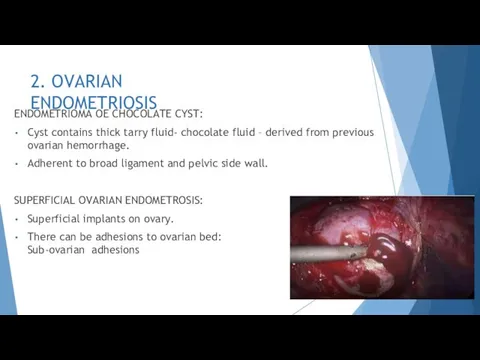
2. OVARIAN ENDOMETRIOSIS
ENDOMETRIOMA OE CHOCOLATE CYST:
Cyst contains thick tarry fluid- chocolate
2. OVARIAN ENDOMETRIOSIS
ENDOMETRIOMA OE CHOCOLATE CYST:
Cyst contains thick tarry fluid- chocolate
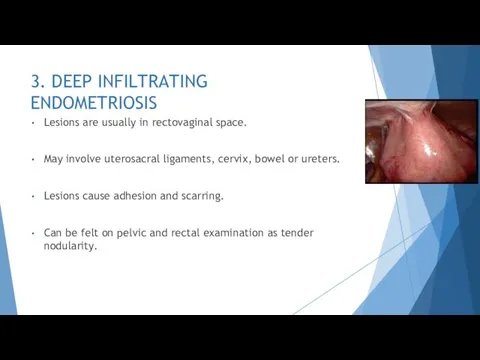
3. DEEP INFILTRATING ENDOMETRIOSIS
Lesions are usually in rectovaginal space.
May involve uterosacral
3. DEEP INFILTRATING ENDOMETRIOSIS
Lesions are usually in rectovaginal space.
May involve uterosacral
4. EXTRAPELVIC ENDOMETRIOSIS
GASTROINTESTINAL TRACT:
Frequently involved: sigmoid, rectum, iliocaecum & appendix.
Symptoms: abdominal
4. EXTRAPELVIC ENDOMETRIOSIS
GASTROINTESTINAL TRACT:
Frequently involved: sigmoid, rectum, iliocaecum & appendix.
Symptoms: abdominal
Extrapelvic endometriosis cont.
SCAR ENDOMETRIOSIS:
Seen at umbilicus, port sites following laparoscopy, abdominal
Extrapelvic endometriosis cont.
SCAR ENDOMETRIOSIS:
Seen at umbilicus, port sites following laparoscopy, abdominal
INVESTIGATIONS
CT & MRI: Identical picture as in USG
COLOUR DOPPLER FLOW: Increased
INVESTIGATIONS
CT & MRI: Identical picture as in USG
COLOUR DOPPLER FLOW: Increased

HISTOLOGY
Histologic confirmation is essential.
On microscopy, typical endometrial implant with endometrial glands
HISTOLOGY
Histologic confirmation is essential.
On microscopy, typical endometrial implant with endometrial glands
CLASSIFICATION OF ENDOMETRIOSIS
Stage I: MINIMAL: Score 1-5
Small spots of endometriosis seen
CLASSIFICATION OF ENDOMETRIOSIS
Stage I: MINIMAL: Score 1-5
Small spots of endometriosis seen
Stage IV: SEVERE: Score >40
Endometriomas exceed 2cm.
Dense Peritubal & periovarian adhesions
Stage IV: SEVERE: Score >40
Endometriomas exceed 2cm.
Dense Peritubal & periovarian adhesions
DIFFEERENTIAL DIAGNOSIS
Chronic PID
Postoperative adhesions
Old ectopic gestation
Pelvic congestion syndrome
Irritable bowel syndrome
Diverticulitis
Ulcerative colitis
Crohn’s
DIFFEERENTIAL DIAGNOSIS
Chronic PID
Postoperative adhesions
Old ectopic gestation
Pelvic congestion syndrome
Irritable bowel syndrome
Diverticulitis
Ulcerative colitis
Crohn’s

MANAGEMENT
MANAGEMENT
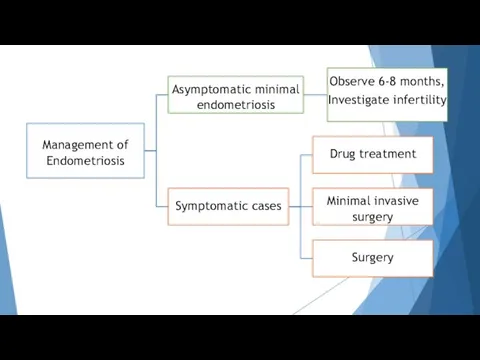
Management of Endometriosis
Asymptomatic minimal endometriosis
Observe 6-8 months, Investigate infertility
Symptomatic cases
Drug treatment
Minimal
Management of Endometriosis
Asymptomatic minimal endometriosis
Observe 6-8 months, Investigate infertility
Symptomatic cases
Drug treatment
Minimal
DRUG TREATMENT
Combined oral contraceptives:
Administered intermittently or continuously.
High Incidence of side effects
DRUG TREATMENT
Combined oral contraceptives:
Administered intermittently or continuously.
High Incidence of side effects
DRUG TREATMENT
Danazol
A synthetic derivative of ethinyl testosterone,
Mildly anabolic , anti-oestrogenic and
DRUG TREATMENT
Danazol
A synthetic derivative of ethinyl testosterone,
Mildly anabolic , anti-oestrogenic and
Drug treatment
Gonadotropin releasing hormone:
GnRH is administered continuously to down regulate and
Drug treatment
Gonadotropin releasing hormone:
GnRH is administered continuously to down regulate and
DRUG THERAPY
Failure of drug therapy is due to :
Drug cannot penetrate
DRUG THERAPY
Failure of drug therapy is due to :
Drug cannot penetrate
MINIMAL INVASIVE SURGERY
Aspiration of peritoneal fluid in cul-de-sac.
Destruction of endometriotic implants <3cm
MINIMAL INVASIVE SURGERY
Aspiration of peritoneal fluid in cul-de-sac.
Destruction of endometriotic implants <3cm
MINIMAL INVASIVE SURGERY
Role of surgery:
Failed Medical therapy
Infertility
Recurrence
Chocolate
MINIMAL INVASIVE SURGERY
Role of surgery:
Failed Medical therapy
Infertility
Recurrence
Chocolate
SURGERY
Indications for surgery:
Advanced stage of disease detected
Large lesion
Medical therapy fails or
SURGERY
Indications for surgery:
Advanced stage of disease detected
Large lesion
Medical therapy fails or
SURGERY
Laparotomy:
In advanced & larger lesions if medical therapy fails.
Dissection and excision
SURGERY
Laparotomy:
In advanced & larger lesions if medical therapy fails.
Dissection and excision

COMBINED THERAPY
Preoperative GnRH:
monthly for 3 months
reduces size & extend of lesions,
softens
COMBINED THERAPY
Preoperative GnRH:
monthly for 3 months
reduces size & extend of lesions,
softens
PROPHYLAXIS
Low-dose OCP reduce the menstrual flow & protect against endometriosis. 3
PROPHYLAXIS
Low-dose OCP reduce the menstrual flow & protect against endometriosis. 3
 Первая помощь пострадавшим и её значение
Первая помощь пострадавшим и её значение Болезнь Стилла у взрослых
Болезнь Стилла у взрослых Респираторные инфекции нижних дыхательных путей – клинические аспекты резистентности к антимикробной терапии
Респираторные инфекции нижних дыхательных путей – клинические аспекты резистентности к антимикробной терапии Функциональная анатомия центральной нервной системы
Функциональная анатомия центральной нервной системы 1 декабря - День борьбы со СПИДом
1 декабря - День борьбы со СПИДом ЭКГ изменения при Заднем Инфаркте Миокарда
ЭКГ изменения при Заднем Инфаркте Миокарда Клинический случай
Клинический случай Этапы подготовки к выступлению
Этапы подготовки к выступлению Современные представления о предмете социальной психологии
Современные представления о предмете социальной психологии Введение в клинику профессиональных болезней
Введение в клинику профессиональных болезней Острый инфаркт миокарда
Острый инфаркт миокарда Гормоны, их синтетические аналоги, антигормональные средства
Гормоны, их синтетические аналоги, антигормональные средства Ас қорыту жүйесі ауруларындағы негізгі синдромдар
Ас қорыту жүйесі ауруларындағы негізгі синдромдар Особенности онкологических заболеваний у детей
Особенности онкологических заболеваний у детей Профилактика утомления глаз
Профилактика утомления глаз Герпетический энцефалит
Герпетический энцефалит Диагностика гепатита С
Диагностика гепатита С Вирусология. Клиническая и экологическая микробиология. Вирусы гепатитов. Ретровирусы. Онковирусы. (Модуль 3.24)
Вирусология. Клиническая и экологическая микробиология. Вирусы гепатитов. Ретровирусы. Онковирусы. (Модуль 3.24) Понятие о системе здравоохранения в России. СД как профессия, перспективы равзвития СД в России
Понятие о системе здравоохранения в России. СД как профессия, перспективы равзвития СД в России Клинико-анатомические особенности крестцового канала (canalis sacralis)
Клинико-анатомические особенности крестцового канала (canalis sacralis) Организация работы участкового врача-терапевта
Организация работы участкового врача-терапевта Розацеа. Қызғылт безеу
Розацеа. Қызғылт безеу Наследственные заболевания
Наследственные заболевания Теория поколений. Кто такие I Generation?
Теория поколений. Кто такие I Generation? Хирургический сепсис
Хирургический сепсис Тромбоз глубоких вен нижних конечностей
Тромбоз глубоких вен нижних конечностей Генетикалық инженерия негіздері
Генетикалық инженерия негіздері Анемия у беременных
Анемия у беременных