- Chest pain

Содержание
- 2. CHEST PAIN 5% of all ED visits per year Differential diagnosis is difficult
- 3. CHEST PAIN ANATOMY DIFFERENTIAL DIAGNOSIS BRIEF OVERVIEW OF DISEASE PROCESSES CAUSING CHEST PAIN APPROACH TO CHEST
- 4. ANATOMY In devising a differential diagnosis for chest pain, it becomes essential to review the anatomy
- 5. ANATOMY SKIN MUSCLES
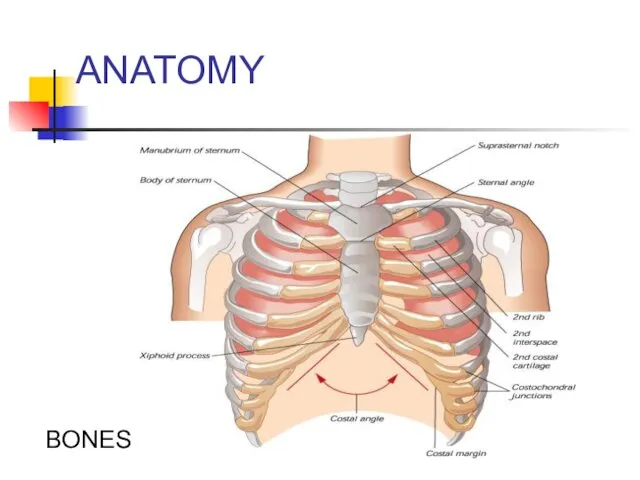
- 6. ANATOMY BONES
- 7. ANATOMY PULMONARY SYSTEM
- 8. ANATOMY HEART
- 9. ANATOMY VASCULAR AND GI SYSTEM AORTA AND ESOPHAGUS
- 10. DIFFERENTIAL DIAGNOSIS OF CHEST PAIN CHEST WALL PAIN PULMONARY CAUSES CARDIAC CAUSES VASCULAR CAUSES GI CAUSES
- 11. DD: CHEST PAIN CHEST WALL PAIN 1 - Skin and sensory nerves -Herpes Zoster 2 -
- 12. DD: CHEST PAIN PULMONARY CAUSES 1 - Pulmonary Embolism 2 – Pneumonia 3 - Pneumothorax/ Tension
- 13. DD: CHEST PAIN CARDIAC CAUSES - Coronary Heart Disease *Myocardial Ischemia *Unstable Angina *Angina - Valvular
- 14. DD: CHEST PAIN Vascular Causes: -Aortic Dissection
- 15. DD: CHEST PAIN GI CAUSES -ESOPHAGEAL *Reflux * Esophagitis * Rupture (Boerhaave Syndrome) * Spasm/Motility Disorder/Foreign
- 16. DD: CHEST PAIN PSYCHIATRIC - PANIC DISORDER - ANXIETY - DEPRESSION - SOMATOFORM DISORDERS
- 17. CHEST PAIN BRIEF OVERVIEW OF DISEASE PROCESSES CAUSING CHEST PAIN
- 18. CHEST WALL PAIN .
- 19. CHEST WALL PAIN HERPES ZOSTER -Reactivation of Herpes Varicellae - Immunocompromised patients often at risk for
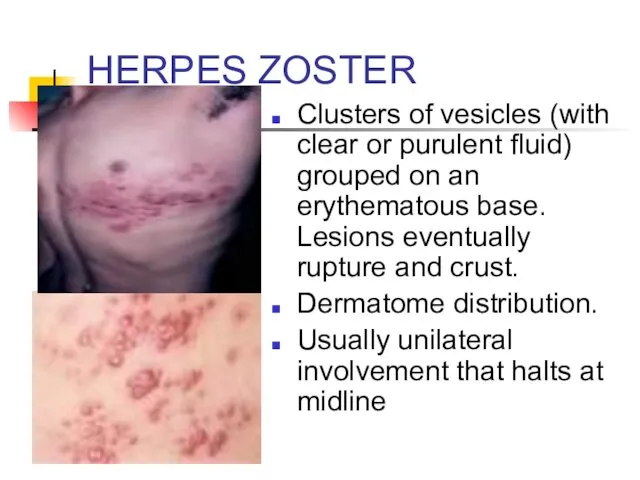
- 20. HERPES ZOSTER Clusters of vesicles (with clear or purulent fluid) grouped on an erythematous base. Lesions
- 21. HERPES ZOSTER TREATMENT: * Antivirals: reduce duration of symptoms; incidence of postherpatic neuralgia. * +/- corticosteroids:
- 22. CHEST WALL PAIN Musculoskeletal Pain - Usually localized, acute, positional; - Pain often reproducible by palpation,
- 23. MUSCULOSKELETAL PAIN DIAGNOSIS COSTOCHONDRITIS TIETZE SYNDROME XIPHODYNIA PRECORDIAL CATCH SYNDROME RIB FRACTURE CLINICAL FEATURES Inflammation of
- 24. MUSCULOSKELETAL PAIN Treatment: Analgesia (NSAIDs)
- 25. PULMONARY CAUSES OF CHEST PAIN .
- 26. PULMONARY EMBOLISM RISK FACTORS: VIRCHOW’S TRIAD - Hypercoagulability *Malignancy *Pregnancy, Early Postpartum, OCPs, HRT *Genetic Mutations:
- 27. PULMONARY EMBOLISM (PE) CLINICAL FEATURES - Shortness of breath - Chest pain: often pleuritic - Tachycardia,
- 28. PE: DIAGNOSTIC TESTS ECG: -Sinus tachycardia most common - Often see nonspecific abnormalities - Look for
- 29. PE: S1Q3T3
- 30. PE: DIAGNOSTIC TESTS CHEST X-RAY - Normal in 25% of cases - Often nonspecific findings -
- 31. CXR: Hampton’s Hump and Westermark’s Sign
- 32. PE: DIAGNOSTIC TESTS ABG: *Look for abnormal PaO2 or A-a gradient D-Dimer: *Often elevated in PE.
- 34. PE: DIAGNOSTIC TESTS VQ SCAN (Ventilation-Perfusion scan)- use in setting of renal insufficiency Helical CT scan
- 35. PE: TREATMENT Initiate Heparin * Unfractionated Heparin: 80 Units/Kg bolus IV, then 18units/kg/hr * Fractionated Heparin
- 36. PNEUMONIA CLINICAL FEATURES - Cough +/- sputum production - Fevers/chills - Pleuritic chest pain - Shortness
- 37. PNEUMONIA: DIAGNOSIS X-Ray If patient is to be hospitalized: Consider GBC (to look for leukocytosis) Consider
- 38. LOCALIZING THE INFILTRATE
- 39. IDENTIFYING LOCATION OF INFILTRATES
- 40. RUL PNEUMONIA RUL INFILTRATE
- 41. RML INFILTRATE Notice that right heart border becomes obscured on PA view of RML pneumonia
- 42. RLL PNEUMONIA RLL infiltrate
- 43. PNEUMONIA: TREATMENT Community- Acquired: - OUT-PATIENT *Doxycycline: Low cost option * Macrolide *Newer fluoroquinolone: Moxifloxacin, Levofloxacin,
- 44. SPONTANEOUS PNEUMOTHORAX RISK FACTORS: - Primary * No underlying lung disease * Young male with greater
- 45. PNEUMOTHORAX CLINICAL FEATURES - Acute pleuritic chest pain: 95% - Usually pain localized to side of
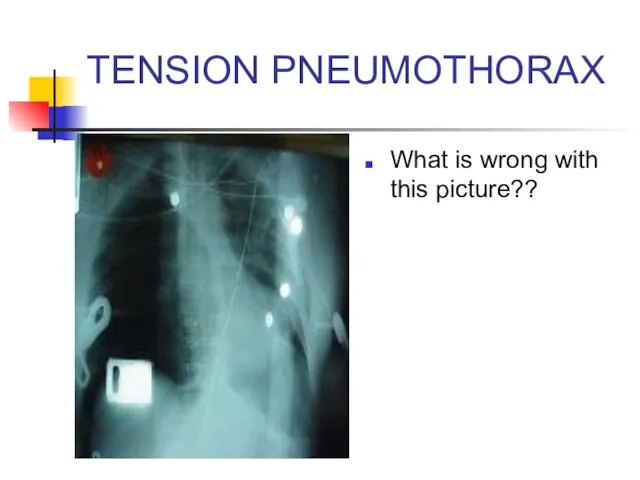
- 46. TENSION PNEUMOTHORAX What is wrong with this picture??
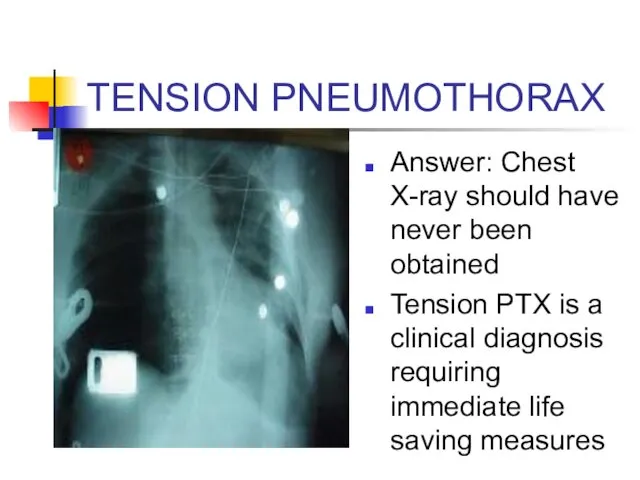
- 47. TENSION PNEUMOTHORAX Answer: Chest X-ray should have never been obtained Tension PTX is a clinical diagnosis
- 48. Tension Pneumothorax Trachea deviates to contralateral side Mediastinum shifts to contralateral side Decreased breath sounds and
- 49. NEEDLE DECOMPRESSION Insert large bore needle (14 or 16 Gauge) with catheter in the 2nd intercostal
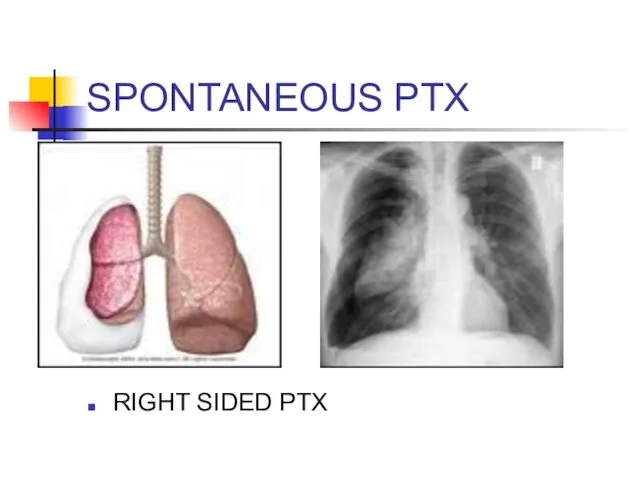
- 50. SPONTANEOUS PTX RIGHT SIDED PTX
- 51. SPONTANEOUS PTX TREATMENT: - If small ( - Give oxygen: Increases pleural air absorption - If
- 52. PLEURITIS/SEROSITIS Inflammation of pleura that covers lung Pleuritic chest pain Causes: - Viral etiology - SLE
- 53. COPD/ASTHMA EXACERBATIONS CLINICAL FEATURES: - Decrease in O2 saturations - Shortness of Breath - May see
- 54. COPD EXACERBATION: TREATMENT Oxygen: Must prevent hypoxemia. Watch for hypercapnia with O2 therapy B2 agonist (albuterol)
- 55. ASTHMA TREATMENT Oxygen Inhaled short acting B2 agonists: Albuterol Anticholinergics: Atrovent Corticosteroids Magnesium Systemic B2 agonists:
- 56. CARDIAC CAUSES OF CHEST PAIN .
- 57. RISK FACTORS FOR CAD Age Diabetes Hypertension Family History Tobacco Use Hypercholesterolemia Cocaine use
- 58. ISCHEMIC CHEST PAIN EXERTIONAL ANGINA * BRIEF EPISODES BROUGHT ON BY EXERTION AND RELIEVED BY REST
- 59. Angina pectoris Stable angina pectoris is a clinical syndrome characterized by precordial or anterior chest discomfort,
- 60. Angina pectoris The chest discomfort may be described by the patient either as a true pain
- 61. The chest discomfort usually lasts up to 20 minutes; a typical episode of angina rarely lasts
- 62. ISCHEMIC CHEST PAIN: DIAGNOSIS 12 LEAD EСG - Look for ST segment elevation (at least 1mm
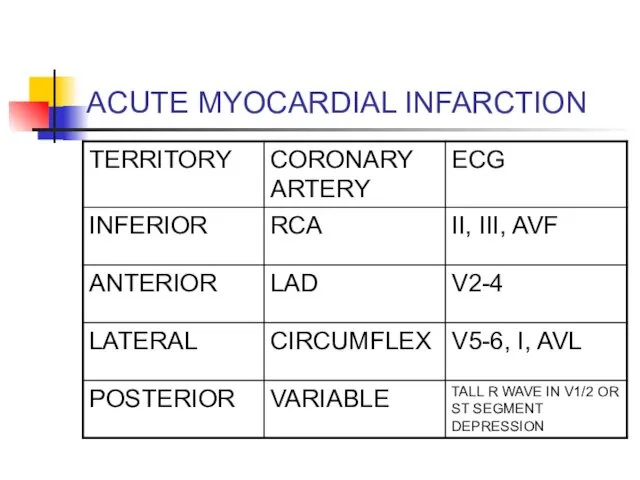
- 63. ACUTE MYOCARDIAL INFARCTION
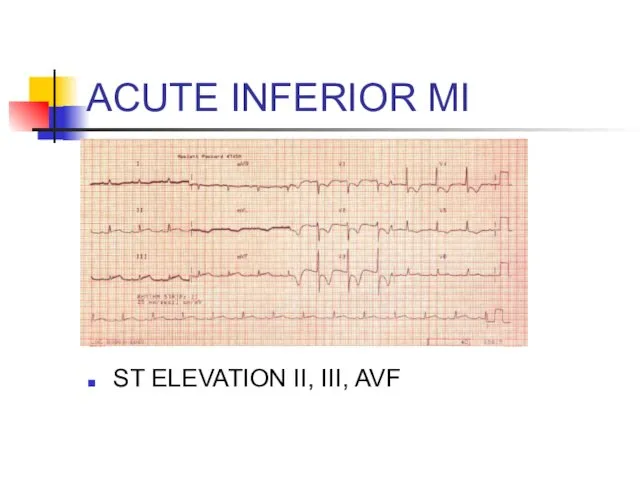
- 64. ACUTE INFERIOR MI ST ELEVATION II, III, AVF
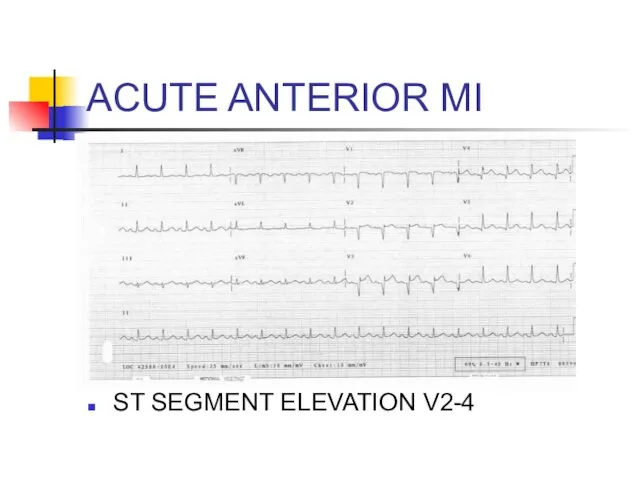
- 65. ACUTE ANTERIOR MI ST SEGMENT ELEVATION V2-4
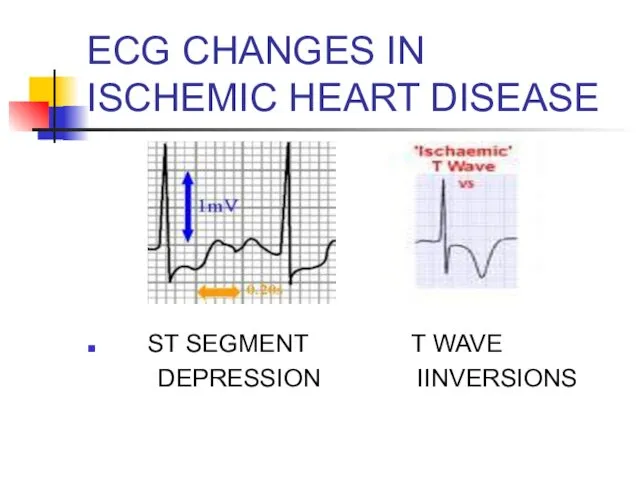
- 66. EСG CHANGES IN ISCHEMIC HEART DISEASE ST SEGMENT T WAVE DEPRESSION IINVERSIONS
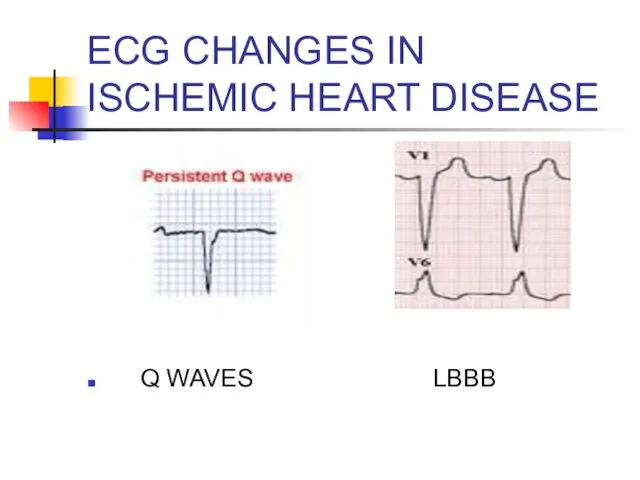
- 67. EСG CHANGES IN ISCHEMIC HEART DISEASE Q WAVES LBBB
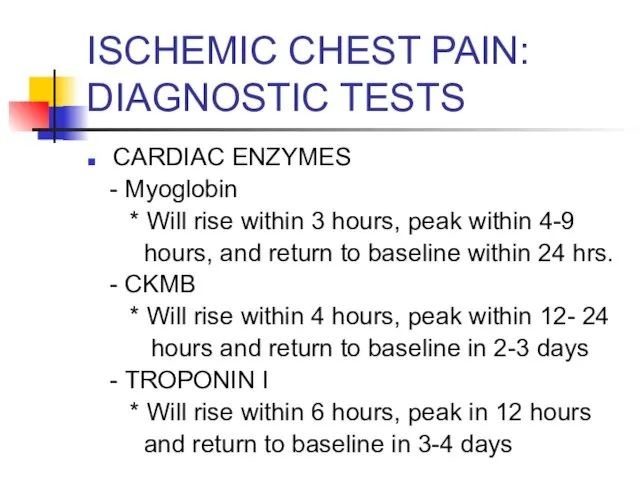
- 68. ISCHEMIC CHEST PAIN: DIAGNOSTIC TESTS CARDIAC ENZYMES - Myoglobin * Will rise within 3 hours, peak
- 69. ISCHEMIC HEART DISEASE TREATMENT: ACUTE ST SEGMENT ELEVATION MI - OXYGEN - ASPIRIN (4 BABY ASPIRIN)
- 70. ISCHEMIC HEART DISEASE TREATMENT: NONSTEMI AND UNSTABLE ANGINA - OXYGEN - ASPIRIN (4 BABY ASPIRIN) -
- 71. LOW RISK CARDIAC CHEST PAIN If low risk chest pain, can consider serial EСGs and enzymes.
- 72. VALVULAR HEART DISEASE AORTIC STENOSIS *Classic triad: dyspnea, chest pain, and syncope * Harsh systolic ejection
- 73. ACUTE PERICARDITIS CLINICAL FEATURES - Acute, stabbing chest pain - Pleuritic chest pain - Pain often
- 74. ACUTE PERICARDITIS COMMON CAUSES * IDIOPATHIC * INFECTIOUS * MALIGNANCY * UREMIA * RADIATION INDUCED *
- 75. ACUTE PERICARDITIS: DIAGNOSTIC TESTS ECG *Look for diffuse ST segment elevation and PR depression. * If
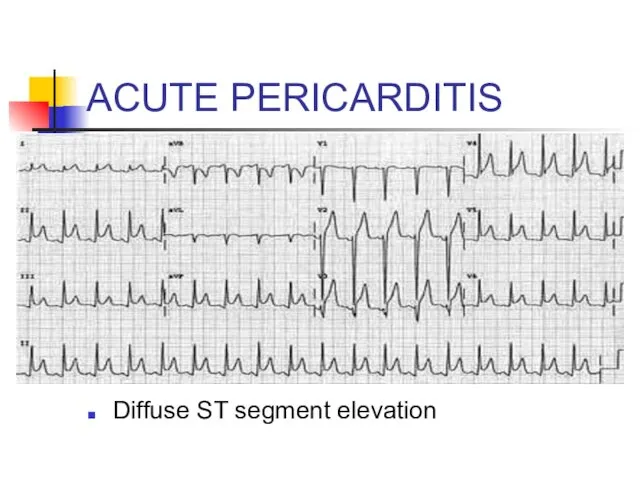
- 76. ACUTE PERICARDITIS Diffuse ST segment elevation
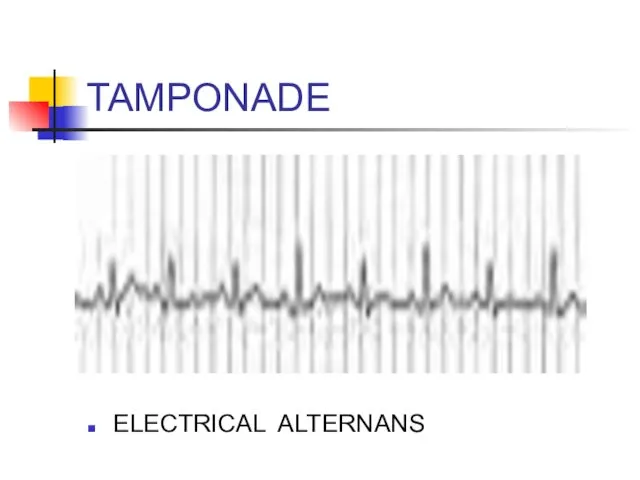
- 77. TAMPONADE ELECTRICAL ALTERNANS
- 78. ACUTE PERICARDITIS TREATMENT: - If idiopathic or viral: NSAIDs - Otherwise treat underlying pathology
- 79. MYOCARDITIS Inflammation of heart muscle Frequently accompanied by pericarditis Fever Tachycardia out of proportion to fever
- 80. VASCULAR CAUSES OF CHEST PAIN .
- 81. AORTIC DISSECTION RISK FACTORS - UNCONTROLLED HYPERTENSION - CONGENITAL HEART DISEASE - CONNECTIVE TISSUE DISEASE -
- 82. AORTIC DISSECTION CLINICAL FEATURES * Abrupt onset of chest pain or pain between scapulae * Tearing
- 83. DIAGNOSIS: AORTIC DISSECTION CXR: Look for widened mediastinum CT SCAN: ANGIOGRAPHY TEE ** suspected dissectons must
- 84. AORTIC DISSECTION WIDENED MEDIASTINUM
- 85. AORTIC DISSECTION TREATMENT: - ANTIHYPERTENSIVE THERAPY *Start with beta blockers (smell, labetalol) * Can add vasodilators
- 86. GI CAUSES OF CHEST PAIN .
- 87. ESOPHAGEAL CAUSES REFLUX ESOPHAGITIS ESOPHAGEAL PERFORATION SPASM/MOTILITY DISORDER/
- 88. GERD RISK FACTORS * High food fat * Caffeine * Nicotine, alcohol * Medicines: CCB, nitrates,
- 89. GERD CLINICAL FEATURES * Burning pain * Association with sour taste in mouth, nausea/vomiting * May
- 90. ESOPHAGITIS CLINICAL FEATURES *Chest pain +Odynophagia (pain with swallowing) Causes *Inflammatory process: GERD or med related
- 91. ESOPHAGEAL PERFORATION CAUSES *Iatrogenic: Endoscopy * Boerhaave Syndrome: Spontaneous rupture secondary to increased intraesophageal pressure. -
- 92. ESOPHAGEAL PERFORATION CLINICAL FEATURES *Acute persistent chest pain that may radiate to back, shoulders, neck *
- 93. ESOPHAGEAL PERFORATION DIAGNOSIS *x-Ray: May see pleural effusion (usually on left). Also may see subQ emphysema,
- 94. ESOPHAGEAL MOTILITY DISORDERS CLINICAL FEATURES: * Chest pain often induced by ingestion of liquids at extremes
- 95. OTHER GI CAUSES In appropriate setting, consider PUD, Biliary Disease, and Pancreatitis in differential of chest
- 96. PSYCHOLOGIC CAUSES Diagnosis of exclusion
- 97. APPROACH TO THE PATIENT WITH CHEST PAIN PUTTING IT ALL TOGETHER
- 98. INITIAL APPROACH Like everything else: ABCs A: Airway B: Breathing C: Circulation IV, O2, cardiac monitor
- 99. CHEST PAIN: HISTORY Time and character of onset Quality Location Radiation Associated symptoms Aggravating symptoms Alleviating
- 100. CHEST PAIN: HISTORY TIME AND CHARACTER OF ONSET: * Abrupt onset with greatest intensity at start:
- 101. CHEST PAIN: HISTORY Quality: *Pleuritic Pain: PE, Pleurisy, Pneumonia, Pericarditis, PTX *Esophageal: Burning, etc *MI: squeezing,
- 102. CHEST PAIN: HISTORY RADIATION: * To neck, jaw, down either arm: consider Ischemia ASSOCIATED SYMPTOMS: *
- 103. CHEST PAIN: HISTORY AGGRAVATING SYMPTOMS: * Activity: consider ischemic heart disease * Food: Consider esophageal disease
- 104. CHEST PAIN: HISTORY ALLEVIATING SYMPTOMS * Rest/ Cessation of Activity: Ischemic * NTG: (Cardiac or esophageal)
- 105. CHEST PAIN: HISTORY RISK FACTORS * Hypertension, DM, high cholesterol, tobacco, family history: Ischemia * Long
- 106. CHEST PAIN: HISTORY When did the pain start? What were you doing when the pain started?
- 107. CHEST PAIN: PHYSICAL EXAM Review vital signs * Fever: Pericarditis, Pneumonia * Check BP in both
- 108. CHEST PAIN: PHYSICAL EXAM CV EXAM * Assess heart rate * Listen for murmurs: * Listen
- 109. CHEST PAIN: ANCILLARY TESTING LABS: Consider……. * Baseline labs: CBC, BMP, PT/PTT * D dimer (PE)
- 110. CHEST PAIN: ANCILLARY TESTS IMAGING: CONSIDER…… * x-Ray - Rib fractures - Hampton’s Hump/ Westermark’s sign:
- 112. Скачать презентацию
CHEST PAIN
5% of all ED visits per year
Differential diagnosis is difficult
CHEST PAIN
5% of all ED visits per year
Differential diagnosis is difficult
CHEST PAIN
ANATOMY
DIFFERENTIAL DIAGNOSIS
BRIEF OVERVIEW OF DISEASE PROCESSES CAUSING CHEST PAIN
APPROACH TO
CHEST PAIN
ANATOMY
DIFFERENTIAL DIAGNOSIS
BRIEF OVERVIEW OF DISEASE PROCESSES CAUSING CHEST PAIN
APPROACH TO
ANATOMY
In devising a differential diagnosis for chest pain, it becomes essential
ANATOMY
In devising a differential diagnosis for chest pain, it becomes essential
ANATOMY
SKIN MUSCLES
ANATOMY
SKIN MUSCLES
ANATOMY
BONES
ANATOMY
BONES
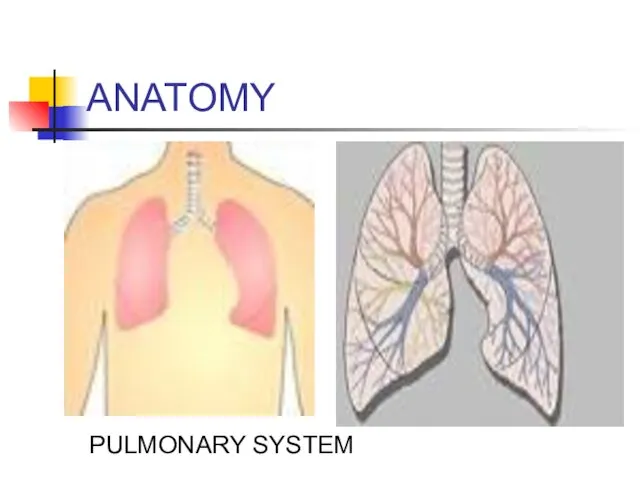
ANATOMY
PULMONARY SYSTEM
ANATOMY
PULMONARY SYSTEM
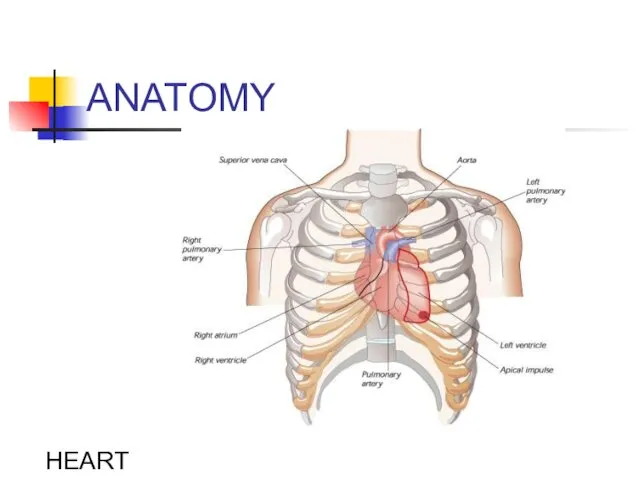
ANATOMY
HEART
ANATOMY
HEART
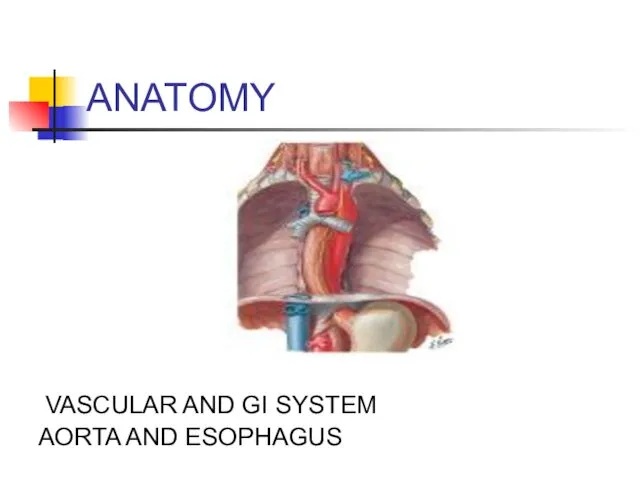
ANATOMY
VASCULAR AND GI SYSTEM
AORTA AND ESOPHAGUS
ANATOMY
VASCULAR AND GI SYSTEM
AORTA AND ESOPHAGUS
DIFFERENTIAL DIAGNOSIS OF CHEST PAIN
CHEST WALL PAIN
PULMONARY CAUSES
CARDIAC CAUSES
VASCULAR CAUSES
GI CAUSES
OTHER
DIFFERENTIAL DIAGNOSIS OF CHEST PAIN
CHEST WALL PAIN
PULMONARY CAUSES
CARDIAC CAUSES
VASCULAR CAUSES
GI CAUSES
OTHER
DD: CHEST PAIN
CHEST WALL PAIN
1 - Skin and sensory nerves
DD: CHEST PAIN
CHEST WALL PAIN
1 - Skin and sensory nerves
DD: CHEST PAIN
PULMONARY CAUSES
1 - Pulmonary Embolism
2 – Pneumonia
3
DD: CHEST PAIN
PULMONARY CAUSES
1 - Pulmonary Embolism
2 – Pneumonia
3
DD: CHEST PAIN
CARDIAC CAUSES
- Coronary Heart Disease
*Myocardial Ischemia
*Unstable
DD: CHEST PAIN
CARDIAC CAUSES
- Coronary Heart Disease
*Myocardial Ischemia
*Unstable
DD: CHEST PAIN
Vascular Causes:
-Aortic Dissection
DD: CHEST PAIN
Vascular Causes:
-Aortic Dissection
DD: CHEST PAIN
GI CAUSES
-ESOPHAGEAL
*Reflux
* Esophagitis
* Rupture (Boerhaave
DD: CHEST PAIN
GI CAUSES
-ESOPHAGEAL
*Reflux
* Esophagitis
* Rupture (Boerhaave
DD: CHEST PAIN
PSYCHIATRIC
- PANIC DISORDER
- ANXIETY
- DEPRESSION
-
DD: CHEST PAIN
PSYCHIATRIC
- PANIC DISORDER
- ANXIETY
- DEPRESSION
-
CHEST PAIN
BRIEF OVERVIEW OF DISEASE PROCESSES CAUSING CHEST PAIN
CHEST PAIN
BRIEF OVERVIEW OF DISEASE PROCESSES CAUSING CHEST PAIN
CHEST WALL PAIN
.
CHEST WALL PAIN
.
CHEST WALL PAIN
HERPES ZOSTER
-Reactivation of Herpes Varicellae
- Immunocompromised patients
CHEST WALL PAIN
HERPES ZOSTER
-Reactivation of Herpes Varicellae
- Immunocompromised patients
HERPES ZOSTER
Clusters of vesicles (with clear or purulent fluid) grouped on
HERPES ZOSTER
Clusters of vesicles (with clear or purulent fluid) grouped on
HERPES ZOSTER
TREATMENT:
* Antivirals: reduce duration of symptoms; incidence of postherpatic
HERPES ZOSTER
TREATMENT:
* Antivirals: reduce duration of symptoms; incidence of postherpatic
CHEST WALL PAIN
Musculoskeletal Pain
- Usually localized, acute, positional;
- Pain
CHEST WALL PAIN
Musculoskeletal Pain
- Usually localized, acute, positional;
- Pain
MUSCULOSKELETAL PAIN
DIAGNOSIS
COSTOCHONDRITIS
TIETZE SYNDROME
XIPHODYNIA
PRECORDIAL CATCH SYNDROME
RIB FRACTURE
CLINICAL FEATURES
Inflammation of costal cartilages +/-
MUSCULOSKELETAL PAIN
DIAGNOSIS
COSTOCHONDRITIS
TIETZE SYNDROME
XIPHODYNIA
PRECORDIAL CATCH SYNDROME
RIB FRACTURE
CLINICAL FEATURES
Inflammation of costal cartilages +/-
MUSCULOSKELETAL PAIN
Treatment:
Analgesia (NSAIDs)
MUSCULOSKELETAL PAIN
Treatment:
Analgesia (NSAIDs)
PULMONARY CAUSES OF CHEST PAIN
.
PULMONARY CAUSES OF CHEST PAIN
.
PULMONARY EMBOLISM
RISK FACTORS: VIRCHOW’S TRIAD
- Hypercoagulability
*Malignancy
*Pregnancy, Early Postpartum,
PULMONARY EMBOLISM
RISK FACTORS: VIRCHOW’S TRIAD
- Hypercoagulability
*Malignancy
*Pregnancy, Early Postpartum,
PULMONARY EMBOLISM (PE)
CLINICAL FEATURES
- Shortness of breath
- Chest pain:
PULMONARY EMBOLISM (PE)
CLINICAL FEATURES
- Shortness of breath
- Chest pain:
PE: DIAGNOSTIC TESTS
ECG:
-Sinus tachycardia most common
- Often see
PE: DIAGNOSTIC TESTS
ECG:
-Sinus tachycardia most common
- Often see
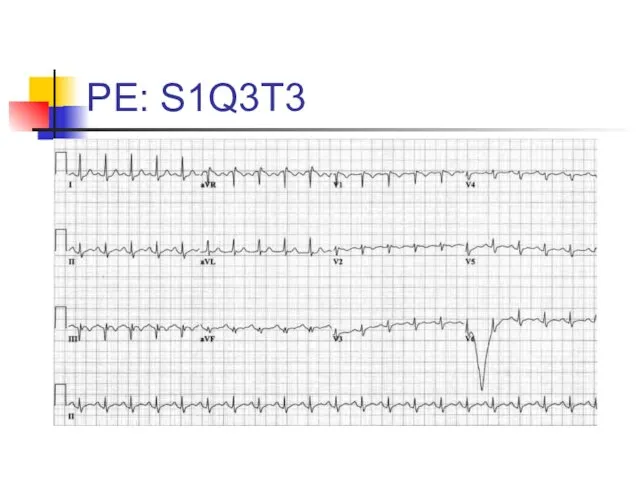
PE: S1Q3T3
PE: S1Q3T3
PE: DIAGNOSTIC TESTS
CHEST X-RAY
- Normal in 25% of cases
-
PE: DIAGNOSTIC TESTS
CHEST X-RAY
- Normal in 25% of cases
-
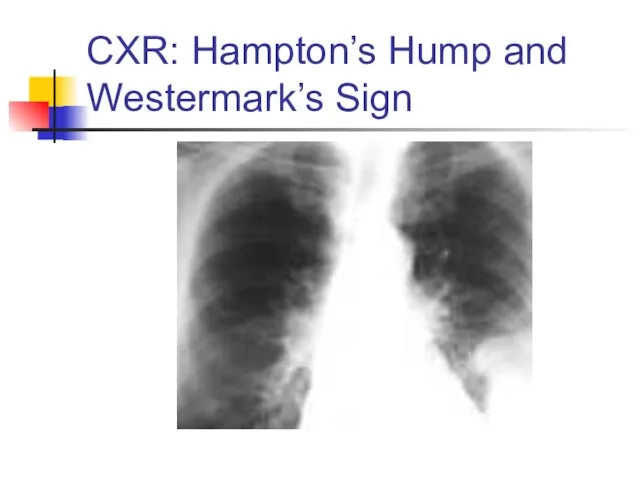
CXR: Hampton’s Hump and Westermark’s Sign
CXR: Hampton’s Hump and Westermark’s Sign
PE: DIAGNOSTIC TESTS
ABG:
*Look for abnormal PaO2 or A-a gradient
D-Dimer:
PE: DIAGNOSTIC TESTS
ABG:
*Look for abnormal PaO2 or A-a gradient
D-Dimer:
PE: DIAGNOSTIC TESTS
VQ SCAN (Ventilation-Perfusion scan)- use in setting of renal
PE: DIAGNOSTIC TESTS
VQ SCAN (Ventilation-Perfusion scan)- use in setting of renal
PE: TREATMENT
Initiate Heparin
* Unfractionated Heparin: 80 Units/Kg bolus IV, then
PE: TREATMENT
Initiate Heparin
* Unfractionated Heparin: 80 Units/Kg bolus IV, then
PNEUMONIA
CLINICAL FEATURES
- Cough +/- sputum production
- Fevers/chills
- Pleuritic
PNEUMONIA
CLINICAL FEATURES
- Cough +/- sputum production
- Fevers/chills
- Pleuritic
PNEUMONIA: DIAGNOSIS
X-Ray
If patient is to be hospitalized:
Consider GBC (to look for
PNEUMONIA: DIAGNOSIS
X-Ray
If patient is to be hospitalized:
Consider GBC (to look for
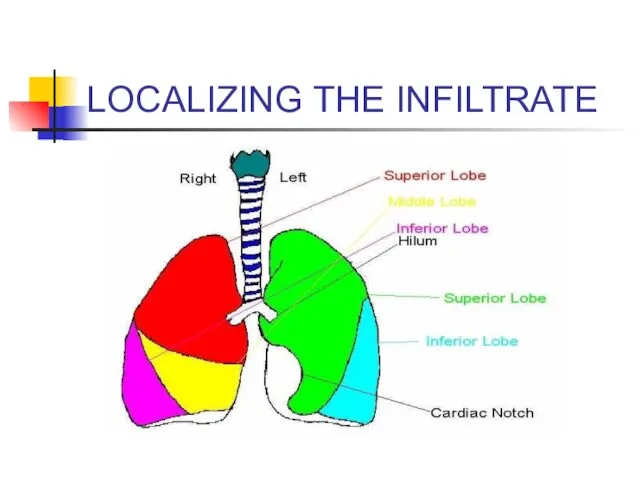
LOCALIZING THE INFILTRATE
LOCALIZING THE INFILTRATE
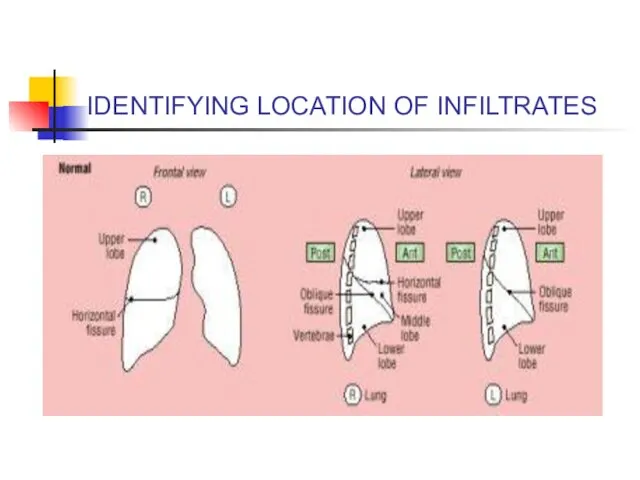
IDENTIFYING LOCATION OF INFILTRATES
IDENTIFYING LOCATION OF INFILTRATES
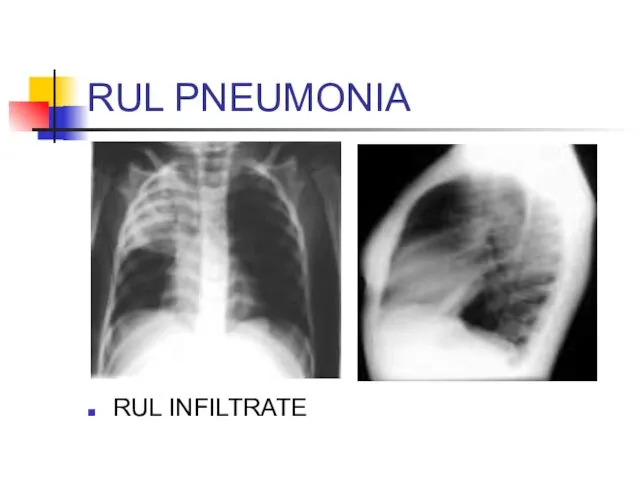
RUL PNEUMONIA
RUL INFILTRATE
RUL PNEUMONIA
RUL INFILTRATE
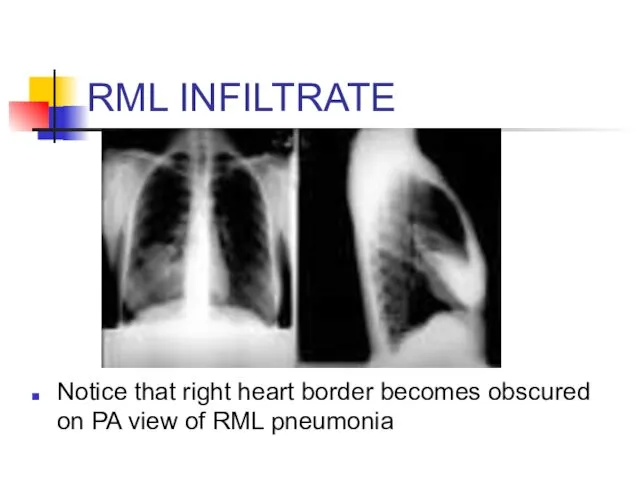
RML INFILTRATE
Notice that right heart border becomes obscured on PA view
RML INFILTRATE
Notice that right heart border becomes obscured on PA view
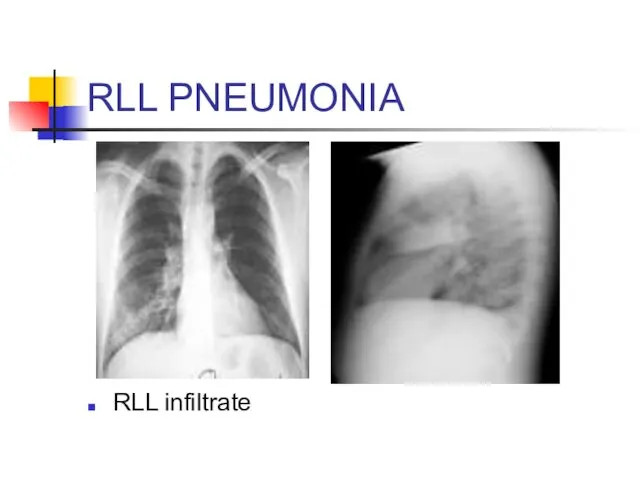
RLL PNEUMONIA
RLL infiltrate
RLL PNEUMONIA
RLL infiltrate
PNEUMONIA: TREATMENT
Community- Acquired:
- OUT-PATIENT
*Doxycycline: Low cost option
*
PNEUMONIA: TREATMENT
Community- Acquired:
- OUT-PATIENT
*Doxycycline: Low cost option
*
SPONTANEOUS PNEUMOTHORAX
RISK FACTORS:
- Primary
* No underlying lung disease
SPONTANEOUS PNEUMOTHORAX
RISK FACTORS:
- Primary
* No underlying lung disease
PNEUMOTHORAX
CLINICAL FEATURES
- Acute pleuritic chest pain: 95%
- Usually pain
PNEUMOTHORAX
CLINICAL FEATURES
- Acute pleuritic chest pain: 95%
- Usually pain
TENSION PNEUMOTHORAX
What is wrong with this picture??
TENSION PNEUMOTHORAX
What is wrong with this picture??
TENSION PNEUMOTHORAX
Answer: Chest X-ray should have never been obtained
Tension PTX is
TENSION PNEUMOTHORAX
Answer: Chest X-ray should have never been obtained
Tension PTX is
Tension Pneumothorax
Trachea deviates to contralateral side
Mediastinum shifts to contralateral side
Decreased breath
Tension Pneumothorax
Trachea deviates to contralateral side
Mediastinum shifts to contralateral side
Decreased breath

NEEDLE DECOMPRESSION
Insert large bore needle (14 or 16 Gauge) with catheter
NEEDLE DECOMPRESSION
Insert large bore needle (14 or 16 Gauge) with catheter
SPONTANEOUS PTX
RIGHT SIDED PTX
SPONTANEOUS PTX
RIGHT SIDED PTX
SPONTANEOUS PTX
TREATMENT:
- If small (<20%), observe with repeated X-rays
-
SPONTANEOUS PTX
TREATMENT:
- If small (<20%), observe with repeated X-rays
-
PLEURITIS/SEROSITIS
Inflammation of pleura that covers lung
Pleuritic chest pain
Causes:
- Viral etiology
PLEURITIS/SEROSITIS
Inflammation of pleura that covers lung
Pleuritic chest pain
Causes:
- Viral etiology
COPD/ASTHMA EXACERBATIONS
CLINICAL FEATURES:
- Decrease in O2 saturations
- Shortness of
COPD/ASTHMA EXACERBATIONS
CLINICAL FEATURES:
- Decrease in O2 saturations
- Shortness of
COPD EXACERBATION: TREATMENT
Oxygen: Must prevent hypoxemia. Watch for hypercapnia with O2
COPD EXACERBATION: TREATMENT
Oxygen: Must prevent hypoxemia. Watch for hypercapnia with O2
ASTHMA TREATMENT
Oxygen
Inhaled short acting B2 agonists: Albuterol
Anticholinergics: Atrovent
Corticosteroids
Magnesium
Systemic B2 agonists: Terbutaline
Heliox
If
ASTHMA TREATMENT
Oxygen
Inhaled short acting B2 agonists: Albuterol
Anticholinergics: Atrovent
Corticosteroids
Magnesium
Systemic B2 agonists: Terbutaline
Heliox
If
CARDIAC CAUSES OF CHEST PAIN
.
CARDIAC CAUSES OF CHEST PAIN
.
RISK FACTORS FOR CAD
Age
Diabetes
Hypertension
Family History
Tobacco Use
Hypercholesterolemia
Cocaine use
RISK FACTORS FOR CAD
Age
Diabetes
Hypertension
Family History
Tobacco Use
Hypercholesterolemia
Cocaine use
ISCHEMIC CHEST PAIN
EXERTIONAL ANGINA
* BRIEF EPISODES BROUGHT ON BY EXERTION
ISCHEMIC CHEST PAIN
EXERTIONAL ANGINA
* BRIEF EPISODES BROUGHT ON BY EXERTION
Angina pectoris
Stable angina pectoris is a clinical syndrome characterized by precordial
Angina pectoris
Stable angina pectoris is a clinical syndrome characterized by precordial
Angina pectoris
The chest discomfort may be described by the patient either
Angina pectoris
The chest discomfort may be described by the patient either
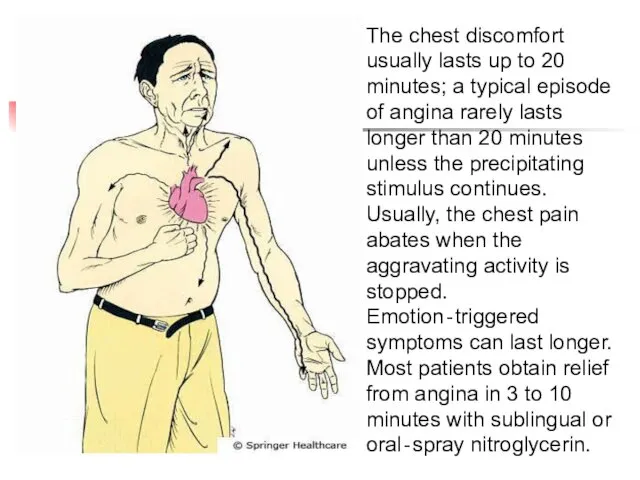
The chest discomfort usually lasts up to 20 minutes; a typical
The chest discomfort usually lasts up to 20 minutes; a typical
ISCHEMIC CHEST PAIN: DIAGNOSIS
12 LEAD EСG
- Look for ST segment
ISCHEMIC CHEST PAIN: DIAGNOSIS
12 LEAD EСG
- Look for ST segment
ACUTE MYOCARDIAL INFARCTION
ACUTE MYOCARDIAL INFARCTION
ACUTE INFERIOR MI
ST ELEVATION II, III, AVF
ACUTE INFERIOR MI
ST ELEVATION II, III, AVF
ACUTE ANTERIOR MI
ST SEGMENT ELEVATION V2-4
ACUTE ANTERIOR MI
ST SEGMENT ELEVATION V2-4
EСG CHANGES IN ISCHEMIC HEART DISEASE
ST SEGMENT T WAVE
EСG CHANGES IN ISCHEMIC HEART DISEASE
ST SEGMENT T WAVE
EСG CHANGES IN ISCHEMIC HEART DISEASE
Q WAVES LBBB
EСG CHANGES IN ISCHEMIC HEART DISEASE
Q WAVES LBBB
ISCHEMIC CHEST PAIN: DIAGNOSTIC TESTS
CARDIAC ENZYMES
- Myoglobin
* Will rise
ISCHEMIC CHEST PAIN: DIAGNOSTIC TESTS
CARDIAC ENZYMES
- Myoglobin
* Will rise
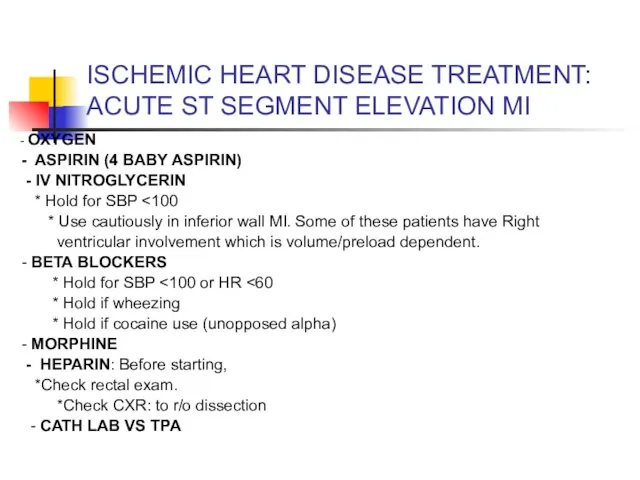
ISCHEMIC HEART DISEASE TREATMENT:
ACUTE ST SEGMENT ELEVATION MI
- OXYGEN
-
ISCHEMIC HEART DISEASE TREATMENT:
ACUTE ST SEGMENT ELEVATION MI
- OXYGEN
-
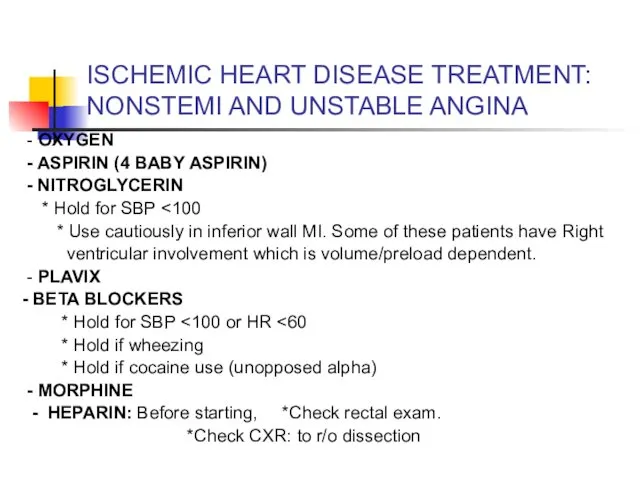
ISCHEMIC HEART DISEASE TREATMENT: NONSTEMI AND UNSTABLE ANGINA
- OXYGEN
-
ISCHEMIC HEART DISEASE TREATMENT: NONSTEMI AND UNSTABLE ANGINA
- OXYGEN
-
LOW RISK CARDIAC CHEST PAIN
If low risk chest pain, can consider
LOW RISK CARDIAC CHEST PAIN
If low risk chest pain, can consider
VALVULAR HEART DISEASE
AORTIC STENOSIS
*Classic triad: dyspnea, chest pain, and syncope
VALVULAR HEART DISEASE
AORTIC STENOSIS
*Classic triad: dyspnea, chest pain, and syncope
ACUTE PERICARDITIS
CLINICAL FEATURES
- Acute, stabbing chest pain
- Pleuritic chest
ACUTE PERICARDITIS
CLINICAL FEATURES
- Acute, stabbing chest pain
- Pleuritic chest
ACUTE PERICARDITIS
COMMON CAUSES
* IDIOPATHIC
* INFECTIOUS
* MALIGNANCY
* UREMIA
ACUTE PERICARDITIS
COMMON CAUSES
* IDIOPATHIC
* INFECTIOUS
* MALIGNANCY
* UREMIA
ACUTE PERICARDITIS: DIAGNOSTIC TESTS
ECG
*Look for diffuse ST segment elevation and
ACUTE PERICARDITIS: DIAGNOSTIC TESTS
ECG
*Look for diffuse ST segment elevation and
ACUTE PERICARDITIS
Diffuse ST segment elevation
ACUTE PERICARDITIS
Diffuse ST segment elevation
TAMPONADE
ELECTRICAL ALTERNANS
TAMPONADE
ELECTRICAL ALTERNANS
ACUTE PERICARDITIS
TREATMENT:
- If idiopathic or viral: NSAIDs
- Otherwise treat
ACUTE PERICARDITIS
TREATMENT:
- If idiopathic or viral: NSAIDs
- Otherwise treat
MYOCARDITIS
Inflammation of heart muscle
Frequently accompanied by pericarditis
Fever
Tachycardia out of proportion to
MYOCARDITIS
Inflammation of heart muscle
Frequently accompanied by pericarditis
Fever
Tachycardia out of proportion to
VASCULAR CAUSES OF CHEST PAIN
.
VASCULAR CAUSES OF CHEST PAIN
.
AORTIC DISSECTION
RISK FACTORS
- UNCONTROLLED HYPERTENSION
- CONGENITAL HEART DISEASE
-
AORTIC DISSECTION
RISK FACTORS
- UNCONTROLLED HYPERTENSION
- CONGENITAL HEART DISEASE
-
AORTIC DISSECTION
CLINICAL FEATURES
* Abrupt onset of chest pain or pain
AORTIC DISSECTION
CLINICAL FEATURES
* Abrupt onset of chest pain or pain
DIAGNOSIS: AORTIC DISSECTION
CXR: Look for widened mediastinum
CT SCAN:
ANGIOGRAPHY
TEE
** suspected dissectons
DIAGNOSIS: AORTIC DISSECTION
CXR: Look for widened mediastinum
CT SCAN:
ANGIOGRAPHY
TEE
** suspected dissectons
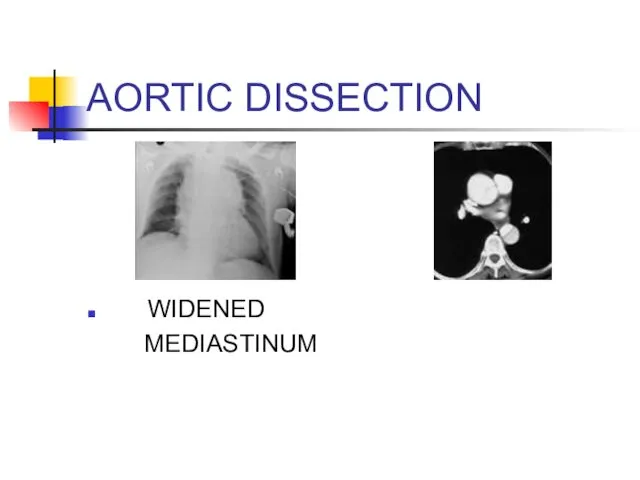
AORTIC DISSECTION
WIDENED
MEDIASTINUM
AORTIC DISSECTION
WIDENED
MEDIASTINUM
AORTIC DISSECTION
TREATMENT:
- ANTIHYPERTENSIVE THERAPY
*Start with beta blockers (smell, labetalol)
AORTIC DISSECTION
TREATMENT:
- ANTIHYPERTENSIVE THERAPY
*Start with beta blockers (smell, labetalol)
GI CAUSES OF CHEST PAIN
.
GI CAUSES OF CHEST PAIN
.
ESOPHAGEAL CAUSES
REFLUX
ESOPHAGITIS
ESOPHAGEAL PERFORATION
SPASM/MOTILITY DISORDER/
ESOPHAGEAL CAUSES
REFLUX
ESOPHAGITIS
ESOPHAGEAL PERFORATION
SPASM/MOTILITY DISORDER/
GERD
RISK FACTORS
* High food fat
* Caffeine
* Nicotine, alcohol
GERD
RISK FACTORS
* High food fat
* Caffeine
* Nicotine, alcohol
GERD
CLINICAL FEATURES
* Burning pain
* Association with sour taste in
GERD
CLINICAL FEATURES
* Burning pain
* Association with sour taste in
ESOPHAGITIS
CLINICAL FEATURES
*Chest pain +Odynophagia (pain with swallowing)
Causes
*Inflammatory process: GERD
ESOPHAGITIS
CLINICAL FEATURES
*Chest pain +Odynophagia (pain with swallowing)
Causes
*Inflammatory process: GERD
ESOPHAGEAL PERFORATION
CAUSES
*Iatrogenic: Endoscopy
* Boerhaave Syndrome: Spontaneous rupture secondary to
ESOPHAGEAL PERFORATION
CAUSES
*Iatrogenic: Endoscopy
* Boerhaave Syndrome: Spontaneous rupture secondary to
ESOPHAGEAL PERFORATION
CLINICAL FEATURES
*Acute persistent chest pain that may radiate to
ESOPHAGEAL PERFORATION
CLINICAL FEATURES
*Acute persistent chest pain that may radiate to
ESOPHAGEAL PERFORATION
DIAGNOSIS
*x-Ray: May see pleural effusion (usually on left). Also
ESOPHAGEAL PERFORATION
DIAGNOSIS
*x-Ray: May see pleural effusion (usually on left). Also
ESOPHAGEAL MOTILITY DISORDERS
CLINICAL FEATURES:
* Chest pain often induced by ingestion
ESOPHAGEAL MOTILITY DISORDERS
CLINICAL FEATURES:
* Chest pain often induced by ingestion
OTHER GI CAUSES
In appropriate setting, consider PUD, Biliary Disease, and Pancreatitis
OTHER GI CAUSES
In appropriate setting, consider PUD, Biliary Disease, and Pancreatitis
PSYCHOLOGIC CAUSES
Diagnosis of exclusion
PSYCHOLOGIC CAUSES
Diagnosis of exclusion
APPROACH TO THE PATIENT WITH CHEST PAIN
PUTTING IT ALL TOGETHER
APPROACH TO THE PATIENT WITH CHEST PAIN
PUTTING IT ALL TOGETHER
INITIAL APPROACH
Like everything else: ABCs
A: Airway
B: Breathing
C: Circulation
IV,
INITIAL APPROACH
Like everything else: ABCs
A: Airway
B: Breathing
C: Circulation
IV,
CHEST PAIN: HISTORY
Time and character of onset
Quality
Location
Radiation
Associated symptoms
Aggravating symptoms
Alleviating symptoms
Prior episodes
Severity
Review
CHEST PAIN: HISTORY
Time and character of onset
Quality
Location
Radiation
Associated symptoms
Aggravating symptoms
Alleviating symptoms
Prior episodes
Severity
Review
CHEST PAIN: HISTORY
TIME AND CHARACTER OF ONSET:
* Abrupt onset with
CHEST PAIN: HISTORY
TIME AND CHARACTER OF ONSET:
* Abrupt onset with
CHEST PAIN: HISTORY
Quality:
*Pleuritic Pain: PE, Pleurisy, Pneumonia, Pericarditis, PTX
*Esophageal:
CHEST PAIN: HISTORY
Quality:
*Pleuritic Pain: PE, Pleurisy, Pneumonia, Pericarditis, PTX
*Esophageal:
CHEST PAIN: HISTORY
RADIATION:
* To neck, jaw, down either arm: consider
CHEST PAIN: HISTORY
RADIATION:
* To neck, jaw, down either arm: consider
CHEST PAIN: HISTORY
AGGRAVATING SYMPTOMS:
* Activity: consider ischemic heart disease
*
CHEST PAIN: HISTORY
AGGRAVATING SYMPTOMS:
* Activity: consider ischemic heart disease
*
CHEST PAIN: HISTORY
ALLEVIATING SYMPTOMS
* Rest/ Cessation of Activity: Ischemic
*
CHEST PAIN: HISTORY
ALLEVIATING SYMPTOMS
* Rest/ Cessation of Activity: Ischemic
*
CHEST PAIN: HISTORY
RISK FACTORS
* Hypertension, DM, high cholesterol, tobacco, family
CHEST PAIN: HISTORY
RISK FACTORS
* Hypertension, DM, high cholesterol, tobacco, family
CHEST PAIN: HISTORY
When did the pain start?
What were you doing when
CHEST PAIN: HISTORY
When did the pain start?
What were you doing when
CHEST PAIN: PHYSICAL EXAM
Review vital signs
* Fever: Pericarditis, Pneumonia
CHEST PAIN: PHYSICAL EXAM
Review vital signs
* Fever: Pericarditis, Pneumonia
CHEST PAIN: PHYSICAL EXAM
CV EXAM
* Assess heart rate
* Listen
CHEST PAIN: PHYSICAL EXAM
CV EXAM
* Assess heart rate
* Listen
CHEST PAIN: ANCILLARY TESTING
LABS: Consider…….
* Baseline labs: CBC, BMP, PT/PTT
CHEST PAIN: ANCILLARY TESTING
LABS: Consider…….
* Baseline labs: CBC, BMP, PT/PTT
CHEST PAIN: ANCILLARY TESTS
IMAGING: CONSIDER……
* x-Ray
- Rib fractures
-
CHEST PAIN: ANCILLARY TESTS
IMAGING: CONSIDER……
* x-Ray
- Rib fractures
-
 Лекарственные растения Кузбасса
Лекарственные растения Кузбасса Дифференциальная диагностика при гепатомегалии
Дифференциальная диагностика при гепатомегалии Острый аппендицит или воспаление червеобразного отростка
Острый аппендицит или воспаление червеобразного отростка Ерте токсикоздардың сирек түрлері
Ерте токсикоздардың сирек түрлері Экзантема (сыпь)
Экзантема (сыпь) Холинолитические ЛС
Холинолитические ЛС Правила наложения повязок
Правила наложения повязок Целиакия (глютеновая энтеропатия)
Целиакия (глютеновая энтеропатия) Этика и деонтология в медицине
Этика и деонтология в медицине Анализ многолетней динамики заболеваемости в эпидемиологической диагностике
Анализ многолетней динамики заболеваемости в эпидемиологической диагностике Стоматологические проявления при ЖДА
Стоматологические проявления при ЖДА Қазақстан Республикасы аймағандағы туберкулез ауруының құрлымы мен деңгейін талдау
Қазақстан Республикасы аймағандағы туберкулез ауруының құрлымы мен деңгейін талдау Управление конфликтами
Управление конфликтами Паллиативная помощь онкологическим больным
Паллиативная помощь онкологическим больным Телесно-ориентированная психотерапия в массаже и детской абилитации
Телесно-ориентированная психотерапия в массаже и детской абилитации Патогенез себореи (акне). Механизм высыпаний
Патогенез себореи (акне). Механизм высыпаний Тотальная внутривенная анестезия
Тотальная внутривенная анестезия Болезнь Рейно
Болезнь Рейно Подстройка под собеседника. Вербальные и невербальные параметры
Подстройка под собеседника. Вербальные и невербальные параметры Электролечение постоянным и импульсным током низкой частоты
Электролечение постоянным и импульсным током низкой частоты Лекарственные препараты растительного происхождения
Лекарственные препараты растительного происхождения Воздушно-капельные инфекции
Воздушно-капельные инфекции Заболевания новорожденных
Заболевания новорожденных Геморрагические диатезы
Геморрагические диатезы Гипертоническая болезнь
Гипертоническая болезнь История развития сестринского дела
История развития сестринского дела Моя профессия - медицинская сестра
Моя профессия - медицинская сестра Эпикриз. Практика
Эпикриз. Практика