- Guidelines in Rheumatology

Содержание
- 2. Genetic Predisposition for Development of Ankylosing Spondylitis (AS) AS and HLA-B27 – strong association Ethnic and
- 3. Natural History of AS Highly variable Early stages: spontaneous remissions and exacerbations Spectrum of severity Mild
- 4. Burden of Illness Functional disability Potential complications Quality-of-life issues Pain, stiffness, fatigue, sleep problems Healthcare costs
- 5. Obstacles to Desirable Outcomes in AS Until Recently Diagnostic and classification limitations Lack of universally accepted
- 6. Advances in Medicine: Hope for Patients With AS Increased understanding of pathophysiologic processes Advent of Anti-TNF
- 7. Pathogenesis of AS Incompletely understood, but knowledge increasing Interaction between HLA-B27 and T-cell response Increased concentration
- 8. Clinical Features of AS
- 9. Modified New York Criteria for the Diagnosis of AS Clinical Criteria Low back pain, > 3
- 10. Disease Activity Assessment BASFI = Bath Ankylosing Spondylitis Functional Index BASDAI = Bath Ankylosing Spondylitis Disease
- 11. Bath Ankylosing Spondylitis Functional Index (BASFI) Visual analog scale (VAS) – 10 cm Mean score of
- 12. Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) A self-administered instrument (using 10-cm horizontal visual analog scales)
- 13. ASsessment in Ankylosing Spondylitis (ASAS) ASAS 20: An improvement of > 20% and absolute improvement of
- 14. Introduction of Anti-TNF Agents for the Treatment of Ankylosing Spondylitis US Modifications of the ASAS International
- 15. Tumor Necrosis Factor: Functions of the Proinflammatory Cytokine Stimulation of endothelial cells to express adhesion molecules
- 16. Pathogenesis of Joint Destruction Bone Erosions Macrophages Endothelium Synoviocytes ↑ Proinflammatory cytokines ↑ Chemokines ↑ Adhesion
- 17. US Modifications of the ASAS International Guidelines: Appropriate Patients for Anti-TNF Therapy Definitive AS according to
- 18. Contraindications for Anti-TNF Therapy Current or recurrent infections Tuberculosis Multiple sclerosis Lupus Malignancy Pregnant or lactating
- 19. Monitoring and Discontinuing Treatment With Anti-TNF Agents ASAS core set of outcome parameters to monitor patients
- 20. Anti-TNF Agents Etanercept Approved in the United States and Europe for treatment of AS Dose: 50
- 21. Etanercept Vs. Infliximab: Pharmacologic Characteristics
- 22. Etanercept vs Infliximab: Clinical Differences Etanercept Approved by FDA for treatment of psoriatic arthritis, rheumatoid arthritis,
- 23. Etanercept for the Treatment of AS: Clinical Trials Marzo-Ortega, et al. Significant improvement in all clinical
- 24. Etanercept for the Treatment of AS: Clinical Trials (cont) Brandt, et al. 57% etanercept-treated patients and
- 25. Etanercept: Adverse Events *P
- 26. Etanercept: Adverse Events (cont) Serious infections and sepsis Mainly in patients with underlying illness or receiving
- 27. Infliximab for the Treatment of AS: Clinical Trials Brandt, et al. ≥ 50% improvement on outcome
- 28. Infliximab for the Treatment of AS: Clinical Trials (cont) Stone, et al. Improvement of > 60%
- 29. Infliximab: Adverse Events * Approximation based on all clinical studies
- 30. Infliximab: Adverse Events (cont) Serious infections and sepsis Cases in patients on concomitant immunosuppressive therapy Neurologic
- 31. Anti-TNF Agents: Summary Anti-TNF agents target underlying inflammatory process Alter disease progression Provide symptomatic relief Recommended
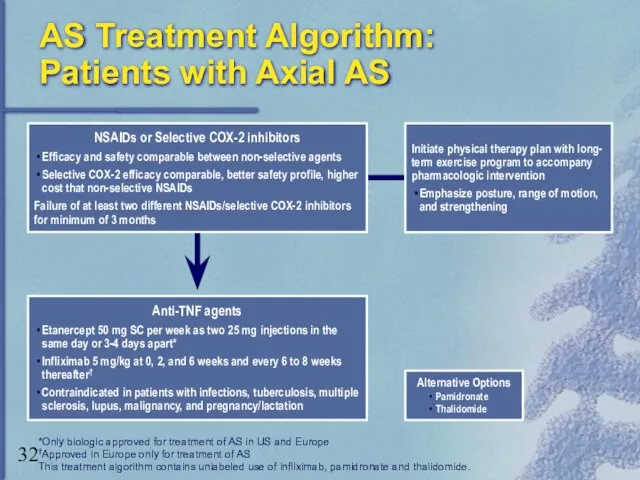
- 32. AS Treatment Algorithm: Patients with Axial AS Alternative Options Pamidronate Thalidomide *Only biologic approved for treatment
- 34. Скачать презентацию
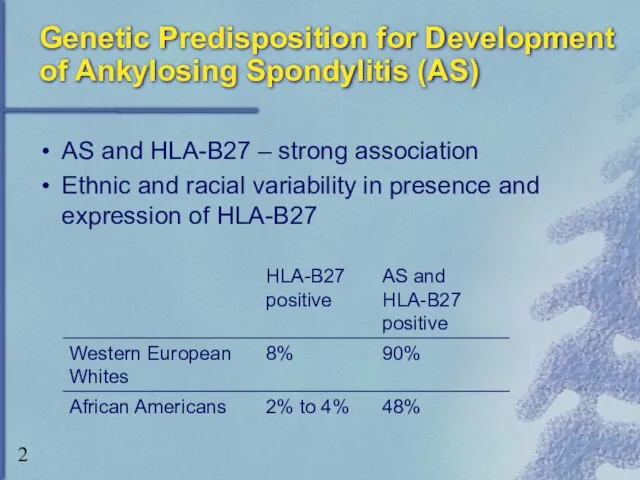
Genetic Predisposition for Development of Ankylosing Spondylitis (AS)
AS and HLA-B27 –
Genetic Predisposition for Development of Ankylosing Spondylitis (AS)
AS and HLA-B27 –

Natural History of AS
Highly variable
Early stages: spontaneous remissions and exacerbations
Spectrum of
Natural History of AS
Highly variable
Early stages: spontaneous remissions and exacerbations
Spectrum of
Burden of Illness
Functional disability
Potential complications
Quality-of-life issues
Pain, stiffness, fatigue, sleep problems
Healthcare costs
Burden of Illness
Functional disability
Potential complications
Quality-of-life issues
Pain, stiffness, fatigue, sleep problems
Healthcare costs
Obstacles to Desirable Outcomes in AS Until Recently
Diagnostic and classification limitations
Lack
Obstacles to Desirable Outcomes in AS Until Recently
Diagnostic and classification limitations
Lack
Advances in Medicine:
Hope for Patients With AS
Increased understanding of pathophysiologic processes
Advances in Medicine:
Hope for Patients With AS
Increased understanding of pathophysiologic processes
Pathogenesis of AS
Incompletely understood, but knowledge increasing
Interaction between HLA-B27 and T-cell
Pathogenesis of AS
Incompletely understood, but knowledge increasing
Interaction between HLA-B27 and T-cell
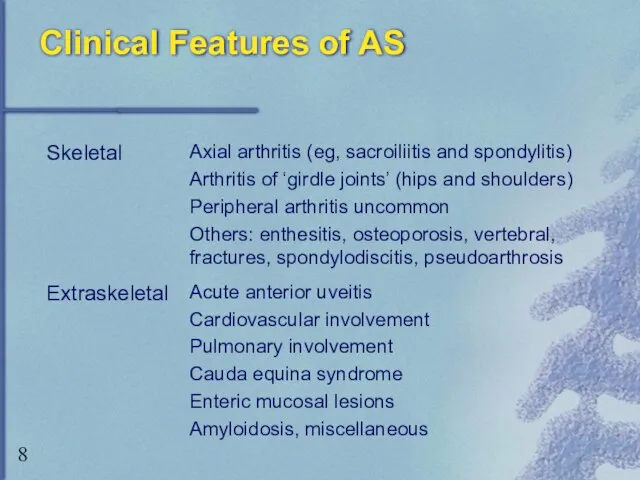
Clinical Features of AS
Clinical Features of AS
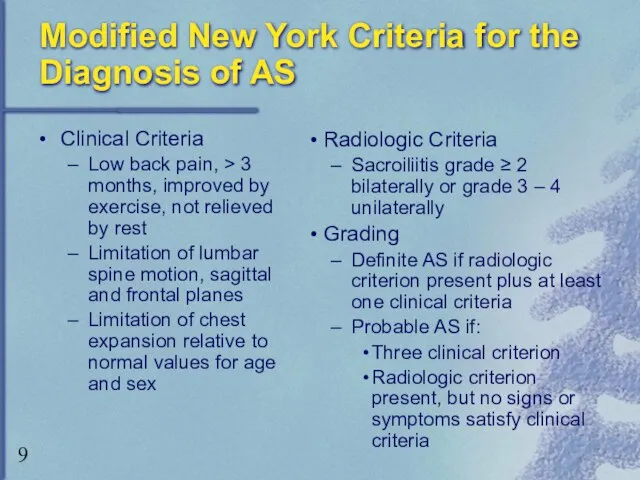
Modified New York Criteria for the Diagnosis of AS
Clinical Criteria
Low back
Modified New York Criteria for the Diagnosis of AS
Clinical Criteria
Low back

Disease Activity Assessment
BASFI = Bath Ankylosing Spondylitis Functional Index
BASDAI = Bath
Disease Activity Assessment
BASFI = Bath Ankylosing Spondylitis Functional Index
BASDAI = Bath
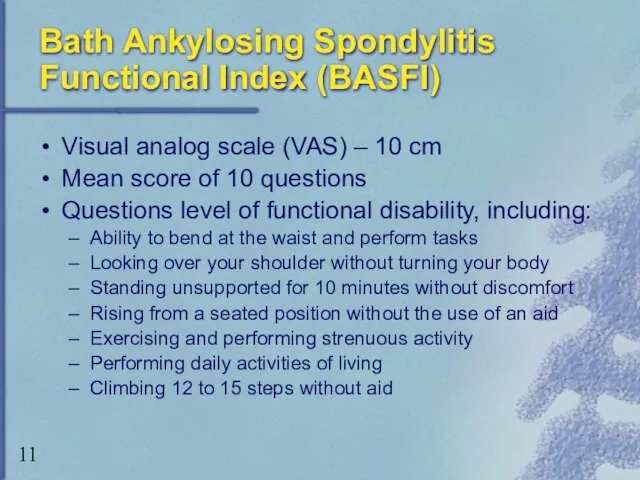
Bath Ankylosing Spondylitis Functional Index (BASFI)
Visual analog scale (VAS) – 10
Bath Ankylosing Spondylitis Functional Index (BASFI)
Visual analog scale (VAS) – 10
Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)
A self-administered instrument (using 10-cm
Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)
A self-administered instrument (using 10-cm
ASsessment in Ankylosing Spondylitis (ASAS)
ASAS 20: An improvement of > 20%
ASsessment in Ankylosing Spondylitis (ASAS)
ASAS 20: An improvement of > 20%

Introduction of Anti-TNF
Agents for the Treatment of Ankylosing Spondylitis
US Modifications
Introduction of Anti-TNF
Agents for the Treatment of Ankylosing Spondylitis
US Modifications
Tumor Necrosis Factor: Functions of the Proinflammatory Cytokine
Stimulation of endothelial cells
Tumor Necrosis Factor: Functions of the Proinflammatory Cytokine
Stimulation of endothelial cells
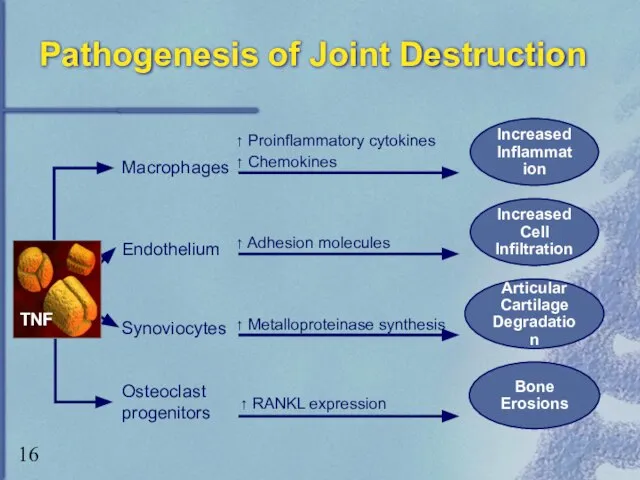
Pathogenesis of Joint Destruction
Bone
Erosions
Macrophages
Endothelium
Synoviocytes
↑ Proinflammatory cytokines
↑ Chemokines
↑ Adhesion molecules
↑
Pathogenesis of Joint Destruction
Bone
Erosions
Macrophages
Endothelium
Synoviocytes
↑ Proinflammatory cytokines
↑ Chemokines
↑ Adhesion molecules
↑
US Modifications of the ASAS International Guidelines: Appropriate Patients for Anti-TNF
US Modifications of the ASAS International Guidelines: Appropriate Patients for Anti-TNF

Contraindications for
Anti-TNF Therapy
Current or recurrent infections
Tuberculosis
Multiple sclerosis
Lupus
Malignancy
Pregnant or lactating
Contraindications for
Anti-TNF Therapy
Current or recurrent infections
Tuberculosis
Multiple sclerosis
Lupus
Malignancy
Pregnant or lactating
Monitoring and Discontinuing Treatment With Anti-TNF Agents
ASAS core set of outcome
Monitoring and Discontinuing Treatment With Anti-TNF Agents
ASAS core set of outcome
Anti-TNF Agents
Etanercept
Approved in the United States and Europe for treatment of
Anti-TNF Agents
Etanercept
Approved in the United States and Europe for treatment of
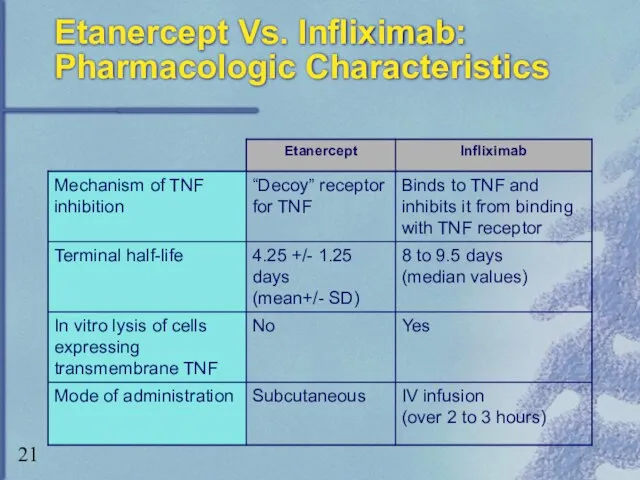
Etanercept Vs. Infliximab:
Pharmacologic Characteristics
Etanercept Vs. Infliximab:
Pharmacologic Characteristics
Etanercept vs Infliximab:
Clinical Differences
Etanercept
Approved by FDA for treatment of psoriatic arthritis,
Etanercept vs Infliximab:
Clinical Differences
Etanercept
Approved by FDA for treatment of psoriatic arthritis,
Etanercept for the Treatment of AS: Clinical Trials
Marzo-Ortega, et al.
Significant
Etanercept for the Treatment of AS: Clinical Trials
Marzo-Ortega, et al.
Significant
Etanercept for the Treatment of AS: Clinical Trials (cont)
Brandt, et al.
57%
Etanercept for the Treatment of AS: Clinical Trials (cont)
Brandt, et al.
57%
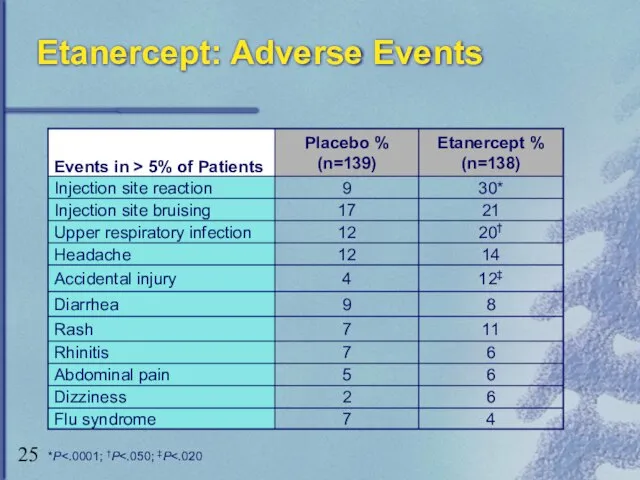
Etanercept: Adverse Events
*P<.0001; †P<.050; ‡P<.020
Etanercept: Adverse Events
*P<.0001; †P<.050; ‡P<.020
Etanercept: Adverse Events (cont)
Serious infections and sepsis
Mainly in patients with underlying
Etanercept: Adverse Events (cont)
Serious infections and sepsis
Mainly in patients with underlying
Infliximab for the Treatment of AS: Clinical Trials
Brandt, et al.
≥ 50%
Infliximab for the Treatment of AS: Clinical Trials
Brandt, et al.
≥ 50%
Infliximab for the Treatment of AS: Clinical Trials (cont)
Stone, et al.
Improvement
Infliximab for the Treatment of AS: Clinical Trials (cont)
Stone, et al.
Improvement
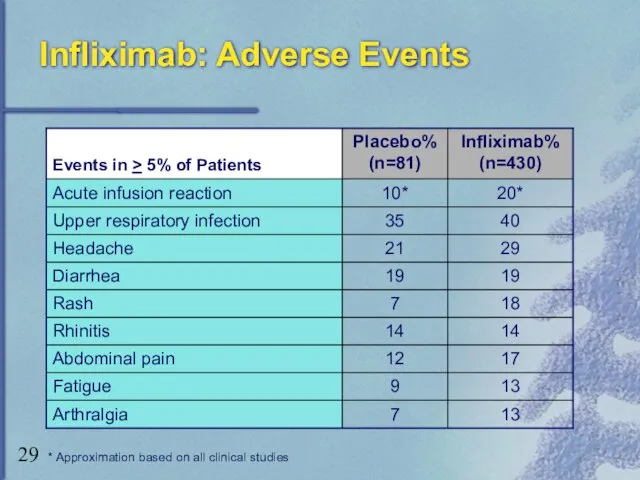
Infliximab: Adverse Events
* Approximation based on all clinical studies
Infliximab: Adverse Events
* Approximation based on all clinical studies
Infliximab: Adverse Events (cont)
Serious infections and sepsis
Cases in patients on concomitant
Infliximab: Adverse Events (cont)
Serious infections and sepsis
Cases in patients on concomitant
Anti-TNF Agents: Summary
Anti-TNF agents target underlying inflammatory process
Alter disease progression
Provide symptomatic
Anti-TNF Agents: Summary
Anti-TNF agents target underlying inflammatory process
Alter disease progression
Provide symptomatic
AS Treatment Algorithm:
Patients with Axial AS
Alternative Options
Pamidronate
Thalidomide
*Only biologic approved for treatment
AS Treatment Algorithm:
Patients with Axial AS
Alternative Options
Pamidronate
Thalidomide
*Only biologic approved for treatment
 Анатомия, физиология и патология органов речи
Анатомия, физиология и патология органов речи Нарушения обмена углеводов
Нарушения обмена углеводов Жедел панкреатит емдеу тәсілдері
Жедел панкреатит емдеу тәсілдері Менің жан дұнием.Таным
Менің жан дұнием.Таным Геморрагический шок в гинекологии
Геморрагический шок в гинекологии Як можна зберегти здоров’я в умовах сучасної екології. Франція
Як можна зберегти здоров’я в умовах сучасної екології. Франція Понятие о клинической смерти. Правила обращения с трупом
Понятие о клинической смерти. Правила обращения с трупом Теория поглаживаний
Теория поглаживаний Белково-калорийная недостаточность и её последствия. Пищевые аллергии. Аллергия на глютен
Белково-калорийная недостаточность и её последствия. Пищевые аллергии. Аллергия на глютен Школа сахарного диабета
Школа сахарного диабета Новые возможности органосохраняющего лечения миомы матки
Новые возможности органосохраняющего лечения миомы матки Бактериофаги - враги наших врагов
Бактериофаги - враги наших врагов Пороки развития позвонков и врожденные деформации позвоночника
Пороки развития позвонков и врожденные деформации позвоночника Хирургиялық стоматологиядағы дәлелді медецина
Хирургиялық стоматологиядағы дәлелді медецина Нормальная артикуляция. Согласные звуки
Нормальная артикуляция. Согласные звуки Аудиометрия. Звуковые методы исследования в медицине: перкуссия, аускультация. Фонокардиография
Аудиометрия. Звуковые методы исследования в медицине: перкуссия, аускультация. Фонокардиография Учение об эпидемическом процессе. Организация профилактических и противоэпидемических мероприятий
Учение об эпидемическом процессе. Организация профилактических и противоэпидемических мероприятий Первая помощь при инфаркте и инсульте
Первая помощь при инфаркте и инсульте Психологические особенности детей с нарушениями зрения
Психологические особенности детей с нарушениями зрения Масштаб проблемы ВБИ. Структура ВБИ
Масштаб проблемы ВБИ. Структура ВБИ Аса қауіпті инфекциялардағы профилактикалық шаралар мен алгоритмдер
Аса қауіпті инфекциялардағы профилактикалық шаралар мен алгоритмдер Анатомическое строение треугольника Пти
Анатомическое строение треугольника Пти Су-электролиттік бұзылыстар және инфузиялық терапияның принциптері
Су-электролиттік бұзылыстар және инфузиялық терапияның принциптері Возбудитель скарлатины
Возбудитель скарлатины Как эффективно начать и убедительно закончить выступление
Как эффективно начать и убедительно закончить выступление Гидропическая дистрофия эпителия проксимальных извитых канальцев почки
Гидропическая дистрофия эпителия проксимальных извитых канальцев почки Құрсақ ішілік инфекциялар. Қызамық
Құрсақ ішілік инфекциялар. Қызамық Личность в теории Эрика Берна
Личность в теории Эрика Берна