- Lung Examination: Abnormal

Содержание
- 5. Illustrative Pathological problems Consolidation Atelectasis Pleural effusion Pneumothorax Mass Diffuse lung disease
- 12. Steps General Examination Mediastinal position Chest expansion Lung resonance Breath sounds Adventitious sounds Voice transmission
- 13. General Examination Respiratory rate Pattern of breathing Cyanosis Clubbing Weight Cough Hospital setting Effort of ventilation
- 14. Respiratory Rate Bradypnea: rate less than 8 per minute Tachypnea: rate greater than 25 per minute
- 15. Pattern of Breathing Kussmals Sleep apnea Cheyne strokes Pursed lip breathing Orthopnoea: Short of breath in
- 16. Sleep apnea syndrome
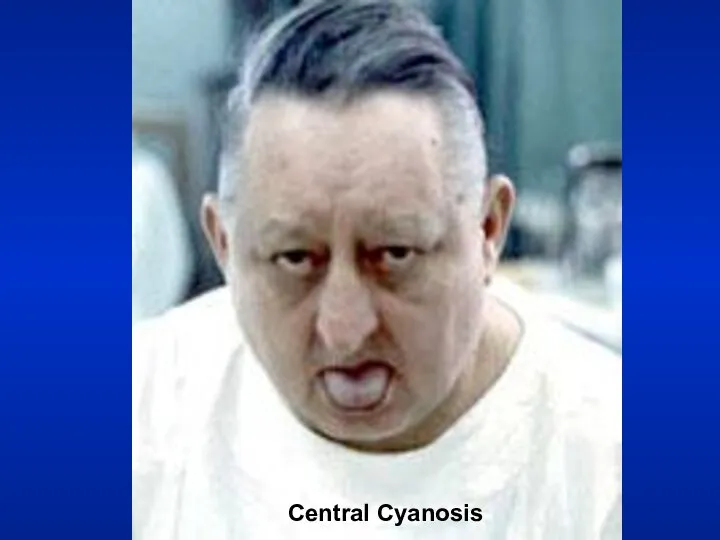
- 17. Central Cyanosis Results from pulmonary dysfunction, the mucous membrane of conjunctiva and tongue are bluish. If
- 18. Central Cyanosis
- 19. Corpulmonale
- 20. Clubbing
- 21. Clubbing In clubbing, there is widening of the AP and lateral diameter of terminal portion of
- 22. Significance: Clubbing Observed In: Intrathoracic malignancy: Primary or secondary (lung, pleural, mediastinal) Suppurative lung disease: (lung
- 23. Gibbus
- 24. Weight Emaciation cachectic Malignancy Tuberculosis
- 25. 320 lbs
- 26. Weight Obese: Sleep apnea syndrome
- 27. 3 Layered sputum
- 28. Cough Productive Dry Whooping Bovine
- 29. 2 liters of O2
- 30. Hospital Setting Isolation room Oxygen set up
- 31. Effort of Ventilation Person appears uncomfortable. Breathing seems voluntary. Accessory muscles are in use, expiratory muscles
- 32. Resting Size and Shape of Thorax Barrel chest Kyphosis Scoliosis Pectus excavatum Gibbus
- 33. Barrel Chest AP Diameter = Transverse Diameter
- 34. Tracheal Position: Mediastinum Any deviation of the mediastinum is abnormal Lateral shift: The mediastinum can be
- 35. Tracheal shift to right
- 36. Chest Expansion Asymmetrical chest expansion is abnormal The abnormal side expands less and lags behind the
- 37. Percussion: Decreased or Increased Resonance is Abnormal Dullness Decreased resonance is noted with pleural effusion and
- 38. Breath Sounds: Diminished or Absent Intensity of breath sounds, in general, is a good index of
- 39. Bronchial Bronchial breathing anywhere other than over the trachea, right clavicle or right inter-scapular space is
- 40. Bronchial breathing
- 41. Rhonchi Rhonchi are long continuous adventitious sounds, generated by obstruction to airways. When detected, note whether
- 42. Rhonchi Asthmatic Continuous
- 43. Rhonchi Localized rhonchi suggests obstruction of any etiology e.g., tumor, foreign body or mucous. Mucous secretions
- 44. Pleural Rub Normal parietal and visceral pleura glide smoothly during respiration. If the pleura is roughened
- 45. Pleural rub Scratching, Grating Related to respiration
- 46. Stridor Loud audible inspiratory rhonchi is called a stridor. Inspiratory rhonchi in general, implies large airway
- 47. Stridor Asthma
- 48. Crackles Interrupted adventitious sounds are called crackles. Make a notation about timing, intensity, effect with respiration,
- 49. Crackles When the crackles are heard at the end of inspiration and the beginning of expiration
- 50. Voice Transmission (tactile fremitus, vocal resonance) Asymmetrical voice transmission points to disease on one side. Increased:
- 51. Voice Transmission (tactile fremitus, vocal resonance) Decreased: A quantitative decrease in voice transmission could be due
- 53. Скачать презентацию


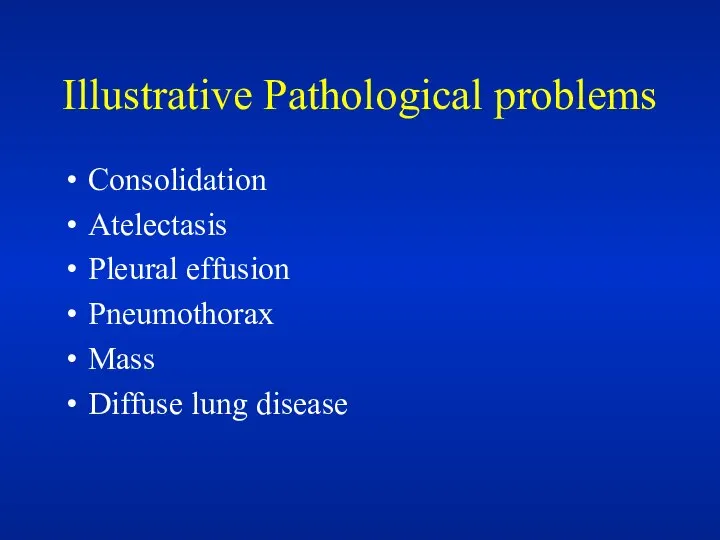
Illustrative Pathological problems
Consolidation
Atelectasis
Pleural effusion
Pneumothorax
Mass
Diffuse lung disease
Illustrative Pathological problems
Consolidation
Atelectasis
Pleural effusion
Pneumothorax
Mass
Diffuse lung disease





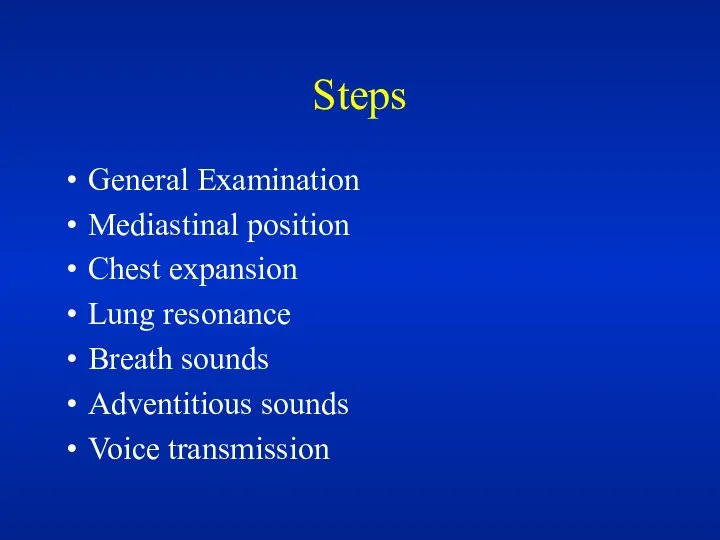
Steps
General Examination
Mediastinal position
Chest expansion
Lung resonance
Breath sounds
Adventitious sounds
Voice transmission
Steps
General Examination
Mediastinal position
Chest expansion
Lung resonance
Breath sounds
Adventitious sounds
Voice transmission
General Examination
Respiratory rate
Pattern of breathing
Cyanosis
Clubbing
Weight
Cough
Hospital setting
Effort of ventilation
Shape of thorax
General Examination
Respiratory rate
Pattern of breathing
Cyanosis
Clubbing
Weight
Cough
Hospital setting
Effort of ventilation
Shape of thorax
Respiratory Rate
Bradypnea: rate less than 8 per minute
Tachypnea: rate greater
Respiratory Rate
Bradypnea: rate less than 8 per minute
Tachypnea: rate greater
Pattern of Breathing
Kussmals
Sleep apnea
Cheyne strokes
Pursed lip breathing
Orthopnoea: Short of breath in
Pattern of Breathing
Kussmals
Sleep apnea
Cheyne strokes
Pursed lip breathing
Orthopnoea: Short of breath in
Sleep apnea syndrome
Sleep apnea syndrome
Central Cyanosis
Results from pulmonary dysfunction, the mucous membrane of conjunctiva and
Central Cyanosis
Results from pulmonary dysfunction, the mucous membrane of conjunctiva and
Central Cyanosis
Central Cyanosis

Corpulmonale
Corpulmonale

Clubbing
Clubbing
Clubbing
In clubbing, there is widening of the AP and lateral diameter
Clubbing
In clubbing, there is widening of the AP and lateral diameter
Significance: Clubbing Observed In:
Intrathoracic malignancy: Primary or secondary (lung, pleural, mediastinal)
Suppurative
Significance: Clubbing Observed In:
Intrathoracic malignancy: Primary or secondary (lung, pleural, mediastinal)
Suppurative

Gibbus
Gibbus
Weight
Emaciation cachectic
Malignancy
Tuberculosis
Weight
Emaciation cachectic
Malignancy
Tuberculosis
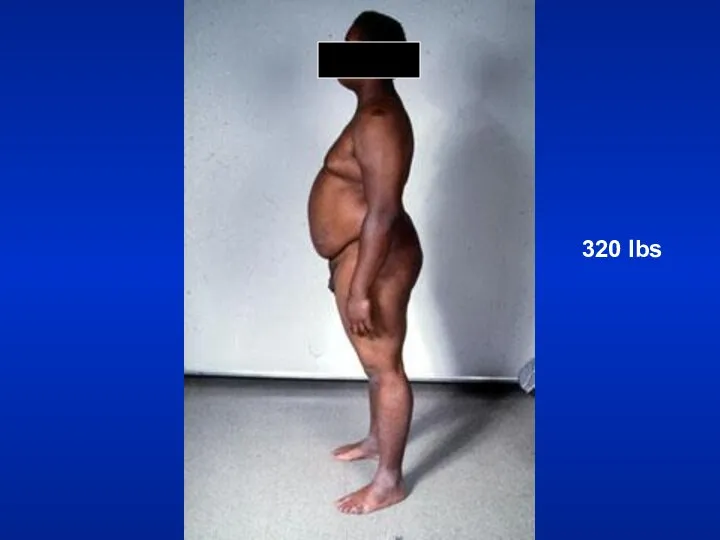
320 lbs
320 lbs
Weight
Obese: Sleep apnea syndrome
Weight
Obese: Sleep apnea syndrome
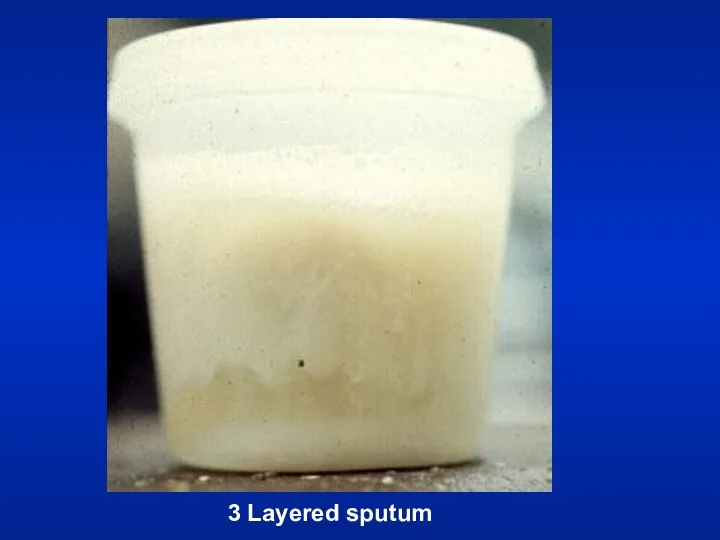
3 Layered sputum
3 Layered sputum
Cough
Productive
Dry
Whooping
Bovine
Cough
Productive
Dry
Whooping
Bovine

2 liters of O2
2 liters of O2
Hospital Setting
Isolation room
Oxygen set up
Hospital Setting
Isolation room
Oxygen set up
Effort of Ventilation
Person appears uncomfortable. Breathing seems voluntary.
Accessory muscles are in
Effort of Ventilation
Person appears uncomfortable. Breathing seems voluntary.
Accessory muscles are in
Resting Size and Shape of Thorax
Barrel chest
Kyphosis
Scoliosis
Pectus excavatum
Gibbus
Resting Size and Shape of Thorax
Barrel chest
Kyphosis
Scoliosis
Pectus excavatum
Gibbus
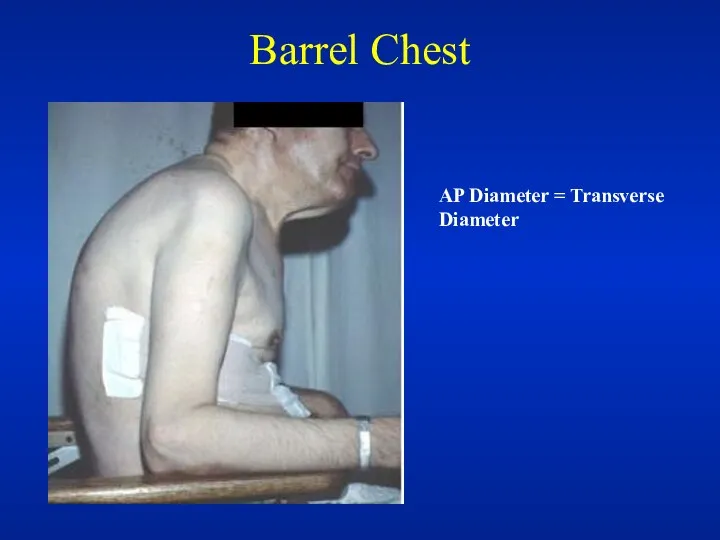
Barrel Chest
AP Diameter = Transverse Diameter
Barrel Chest
AP Diameter = Transverse Diameter
Tracheal Position: Mediastinum
Any deviation of the mediastinum is abnormal
Lateral shift: The
Tracheal Position: Mediastinum
Any deviation of the mediastinum is abnormal
Lateral shift: The
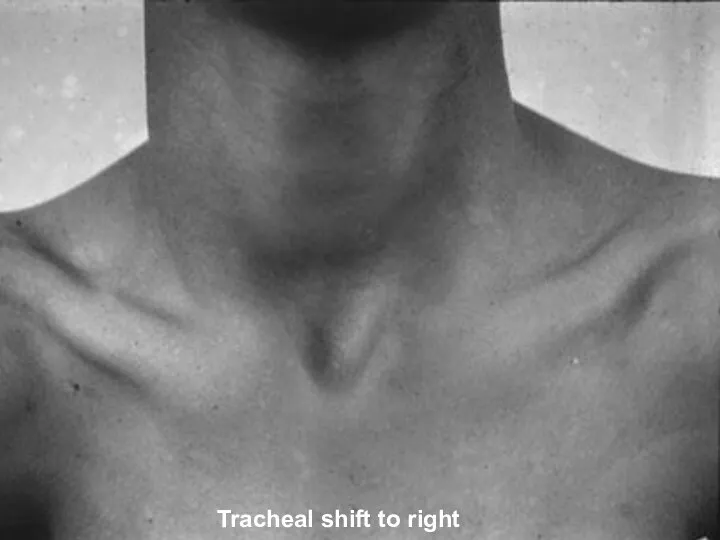
Tracheal shift to right
Tracheal shift to right
Chest Expansion
Asymmetrical chest expansion is abnormal
The abnormal side expands less and
Chest Expansion
Asymmetrical chest expansion is abnormal
The abnormal side expands less and
Percussion: Decreased or Increased Resonance is Abnormal
Dullness
Decreased resonance is noted with
Percussion: Decreased or Increased Resonance is Abnormal
Dullness
Decreased resonance is noted with
Breath Sounds: Diminished or Absent
Intensity of breath sounds, in general, is
Breath Sounds: Diminished or Absent
Intensity of breath sounds, in general, is
Bronchial
Bronchial breathing anywhere other than over the trachea, right clavicle or
Bronchial
Bronchial breathing anywhere other than over the trachea, right clavicle or
Bronchial breathing
Bronchial breathing
Rhonchi
Rhonchi are long continuous adventitious sounds, generated by obstruction to airways.
When
Rhonchi
Rhonchi are long continuous adventitious sounds, generated by obstruction to airways.
When
Rhonchi
Asthmatic
Continuous
Rhonchi
Asthmatic
Continuous
Rhonchi
Localized rhonchi suggests obstruction of any etiology e.g., tumor, foreign body
Rhonchi
Localized rhonchi suggests obstruction of any etiology e.g., tumor, foreign body
Pleural Rub
Normal parietal and visceral pleura glide smoothly during respiration.
If the
Pleural Rub
Normal parietal and visceral pleura glide smoothly during respiration.
If the
Pleural rub
Scratching, Grating
Related to respiration
Pleural rub
Scratching, Grating
Related to respiration
Stridor
Loud audible inspiratory rhonchi is called a stridor.
Inspiratory rhonchi in general,
Stridor
Loud audible inspiratory rhonchi is called a stridor.
Inspiratory rhonchi in general,
Stridor
Asthma
Stridor
Asthma
Crackles
Interrupted adventitious sounds are called crackles.
Make a notation about timing, intensity,
Crackles
Interrupted adventitious sounds are called crackles.
Make a notation about timing, intensity,
Crackles
When the crackles are heard at the end of inspiration and
Crackles
When the crackles are heard at the end of inspiration and
Voice Transmission (tactile fremitus, vocal resonance)
Asymmetrical voice transmission points to disease
Voice Transmission (tactile fremitus, vocal resonance)
Asymmetrical voice transmission points to disease
Voice Transmission (tactile fremitus, vocal resonance)
Decreased: A quantitative decrease in voice
Voice Transmission (tactile fremitus, vocal resonance)
Decreased: A quantitative decrease in voice
 Массаж. Вид приема
Массаж. Вид приема Сонная болезнь
Сонная болезнь Экстракорпоральные методы детоксикации
Экстракорпоральные методы детоксикации Методика «Несуществующее животное»
Методика «Несуществующее животное» Первичная профилактика инсульта
Первичная профилактика инсульта Что нужно знать о ВИЧ-инфекции каждому
Что нужно знать о ВИЧ-инфекции каждому Ингарон. Лекарственная форма
Ингарон. Лекарственная форма Сестринская помощь при хронической сердечной недостаточности. Тема 4.3
Сестринская помощь при хронической сердечной недостаточности. Тема 4.3 Апластическая анемия
Апластическая анемия Антиаритмические ЛС
Антиаритмические ЛС Анатомо-физиологические особенности мочевыделительной системы
Анатомо-физиологические особенности мочевыделительной системы Психологиядағы және наркологиядағы сараптама түрлері
Психологиядағы және наркологиядағы сараптама түрлері Формирование единого регионального профилактического пространства на территории Архангельской области
Формирование единого регионального профилактического пространства на территории Архангельской области Мозг и разум. Личностные компетенции молодого ученого: современные механизмы реализации и коммуникации
Мозг и разум. Личностные компетенции молодого ученого: современные механизмы реализации и коммуникации Теории и типы любви
Теории и типы любви Вирусный гепатит В, желтушная форма, тяжелое течение. Клинический случай
Вирусный гепатит В, желтушная форма, тяжелое течение. Клинический случай Разработка медицинской цифровой платформы для связи врачей и пациентов
Разработка медицинской цифровой платформы для связи врачей и пациентов Шесть шляп мышления. Эдвард Де Боно
Шесть шляп мышления. Эдвард Де Боно Пропедевтика внутренних болезней
Пропедевтика внутренних болезней Диагностика тромбоэмболии легочной артерии (ТЭЛА)
Диагностика тромбоэмболии легочной артерии (ТЭЛА) Өкпе туберкулемасы
Өкпе туберкулемасы Бронхиальная астма у детей
Бронхиальная астма у детей Хронические миелопролиферативные заболевания
Хронические миелопролиферативные заболевания Клинический случай HHV-6 ассоциированного менингоэнцефалита на фоне генерализованной кишечной инфекции
Клинический случай HHV-6 ассоциированного менингоэнцефалита на фоне генерализованной кишечной инфекции Фонокардиограф. Технические характеристики
Фонокардиограф. Технические характеристики Современные методы комплексного лечения больных туберкулезом. Современные схемы лечения различных групп больных
Современные методы комплексного лечения больных туберкулезом. Современные схемы лечения различных групп больных Охрана здоровья граждан в Российской Федерации
Охрана здоровья граждан в Российской Федерации Способы, с помощью которых возможно избежать последствия хронического недосыпания
Способы, с помощью которых возможно избежать последствия хронического недосыпания