- Межлекарственные взаимодействия психотропных препаратов

Содержание
- 2. План: Поиск информации в русскоязычных сайтах Использование англоязычных поисковых систем Pubmed AJP
- 4. Вялотекущая шизофрения в общемедицинской практике А.Б.Смулевич НЦПЗ РАМН, Москва На первом этапе комбинированной психофармакотерапии используются антидепрессанты
- 5. Кардиологические аспекты проблемы переносимости и безопасности нейролептика М.Ю.Дробижев Клиника кардиологии ММА им. И.М. Сеченова, НЦПЗ РАМН,
- 6. Комбинированное использование антидепрессантов и нейролептиков при аффективных расстройствах и шизофрении: показания к назначению, побочные эффекты и
- 8. Drug interactions of psychotropic drugs Sawada Y, Satoh H. Laboratory of Drug Informatics, Graduate School of
- 9. Benzodiazepines alone or in combination with antipsychotic drugs for acute psychosis Gillies D, Beck A, McCloud
- 10. Clozapine combined with different antipsychotic drugs for treatment resistant schizophrenia Cipriani A, Boso M, Barbui C
- 11. Trifluoperazine, an Antipsychotic Agent, Inhibits Cancer Stem Cell Growth and Overcomes Drug Resistance of Lung Cancer
- 12. Double-blind placebo-controlled randomized efficacy and safety trial of add-on treatment of dimebon plus risperidone in schizophrenic
- 13. Combination treatment of depression Høiseth G, Solberg DK, Refsum H. Senter for psykofarmakologi, Diakonhjemmet Sykehus, Norway.
- 15. Multiple Versus Single Antipsychotic Agents for Hospitalized Psychiatric Patients: Case-Control Study of Risks Versus Benefits Franca
- 16. Combined use of risperidone and olanzapine in the treatment of patients with resistant schizophrenia: a preliminary
- 17. Metformin Addition Attenuates Olanzapine-Induced Weight Gain in Drug-Naive First-Episode Schizophrenia Patients: A Double-Blind, Placebo-Controlled Study Ren-Rong
- 18. Randomized, Double-Blind, Placebo-Controlled Study of Paliperidone Extended-Release and Quetiapine in Inpatients With Recently Exacerbated Schizophrenia Carla
- 20. Скачать презентацию
План:
Поиск информации в русскоязычных сайтах
Использование англоязычных поисковых систем
Pubmed
AJP
План:
Поиск информации в русскоязычных сайтах
Использование англоязычных поисковых систем
Pubmed
AJP

Вялотекущая шизофрения в общемедицинской практике
А.Б.Смулевич
НЦПЗ РАМН, Москва
На первом этапе комбинированной
Вялотекущая шизофрения в общемедицинской практике
А.Б.Смулевич
НЦПЗ РАМН, Москва
На первом этапе комбинированной
Кардиологические аспекты проблемы переносимости и безопасности нейролептика
М.Ю.Дробижев
Клиника кардиологии ММА им. И.М.
Кардиологические аспекты проблемы переносимости и безопасности нейролептика М.Ю.Дробижев Клиника кардиологии ММА им. И.М.

Комбинированное использование антидепрессантов и нейролептиков при аффективных расстройствах и шизофрении: показания
Комбинированное использование антидепрессантов и нейролептиков при аффективных расстройствах и шизофрении: показания

Drug interactions of psychotropic drugs
Sawada Y, Satoh H.
Laboratory of Drug Informatics, Graduate School of Pharmaceutical Sciences,
Drug interactions of psychotropic drugs Sawada Y, Satoh H. Laboratory of Drug Informatics, Graduate School of Pharmaceutical Sciences,
Benzodiazepines alone or in combination with antipsychotic drugs for acute psychosis
Gillies
Benzodiazepines alone or in combination with antipsychotic drugs for acute psychosis Gillies
Clozapine combined with different antipsychotic drugs for treatment resistant schizophrenia
Cipriani A,
Clozapine combined with different antipsychotic drugs for treatment resistant schizophrenia Cipriani A,
Trifluoperazine, an Antipsychotic Agent, Inhibits Cancer Stem Cell Growth and Overcomes Drug Resistance
Trifluoperazine, an Antipsychotic Agent, Inhibits Cancer Stem Cell Growth and Overcomes Drug Resistance
Double-blind placebo-controlled randomized efficacy and safety trial of add-on treatment of
Double-blind placebo-controlled randomized efficacy and safety trial of add-on treatment of
Combination treatment of depression
Høiseth G, Solberg DK, Refsum H.
Senter for psykofarmakologi, Diakonhjemmet Sykehus, Norway.
Combination treatment of depression Høiseth G, Solberg DK, Refsum H. Senter for psykofarmakologi, Diakonhjemmet Sykehus, Norway.

Multiple Versus Single Antipsychotic Agents for Hospitalized Psychiatric Patients: Case-Control Study
Multiple Versus Single Antipsychotic Agents for Hospitalized Psychiatric Patients: Case-Control Study
Combined use of risperidone and olanzapine in the treatment of patients with resistant
Combined use of risperidone and olanzapine in the treatment of patients with resistant
Metformin Addition Attenuates Olanzapine-Induced Weight Gain in Drug-Naive First-Episode Schizophrenia Patients:
Metformin Addition Attenuates Olanzapine-Induced Weight Gain in Drug-Naive First-Episode Schizophrenia Patients:
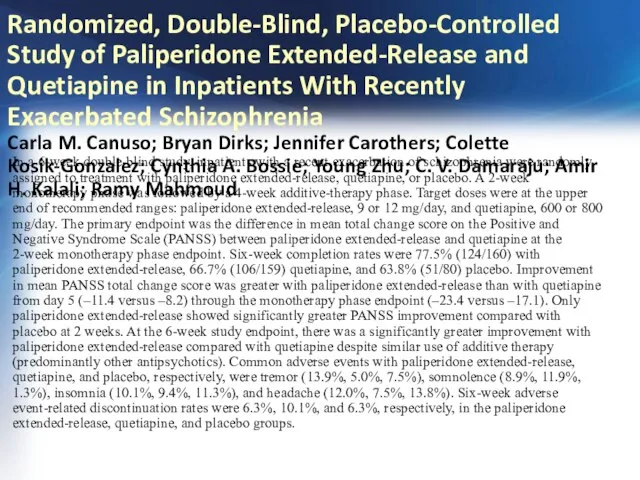
Randomized, Double-Blind, Placebo-Controlled Study of Paliperidone Extended-Release and Quetiapine in Inpatients
Randomized, Double-Blind, Placebo-Controlled Study of Paliperidone Extended-Release and Quetiapine in Inpatients
 Реабилитация заболеваний дыхательной системы у детей
Реабилитация заболеваний дыхательной системы у детей Аллергия - проблема XXI века
Аллергия - проблема XXI века Обструктивный синдром у детей
Обструктивный синдром у детей Физическое развитие детей раннего возраста
Физическое развитие детей раннего возраста Лечебная физкультура (ЛФК) для восстановления позвоночника
Лечебная физкультура (ЛФК) для восстановления позвоночника Остеомиелит салдары
Остеомиелит салдары Пандемии прошлого в сравнении с пандемией COVID-19
Пандемии прошлого в сравнении с пандемией COVID-19 Грипп: профилактика и лечение
Грипп: профилактика и лечение Удивительная жидкость - кровь
Удивительная жидкость - кровь Сосудистые средства
Сосудистые средства Диагностика психологической готовности ребенка к школе
Диагностика психологической готовности ребенка к школе Основные характеристики ВИЧ - инфекции
Основные характеристики ВИЧ - инфекции Синдром анемии в обще-врачебной практике
Синдром анемии в обще-врачебной практике Всемирный день борьбы против рака
Всемирный день борьбы против рака Преодоление конфликтов. Виды конфликтов
Преодоление конфликтов. Виды конфликтов Обучение альтернативной коммуникации детей с ОПФР
Обучение альтернативной коммуникации детей с ОПФР Дифференцированный логопедический массаж
Дифференцированный логопедический массаж Организация питания пациентов терапевтического и хирургического профиля
Организация питания пациентов терапевтического и хирургического профиля Жатыр мойны обыры
Жатыр мойны обыры Психология малой группы
Психология малой группы Алгоритмы диагностики и лечения злокачественных новообразований
Алгоритмы диагностики и лечения злокачественных новообразований Черепно-мозговая травма. Основные клинические формы
Черепно-мозговая травма. Основные клинические формы Conflict
Conflict Переломы костей
Переломы костей Как понять, что нужно клиенту
Как понять, что нужно клиенту Гиршпрунг ауруының визуалды диагностикасы
Гиршпрунг ауруының визуалды диагностикасы Новая линия косметических средств MEZOcomplex
Новая линия косметических средств MEZOcomplex Диэнай. Зачем нужна фрагментированная ДНК
Диэнай. Зачем нужна фрагментированная ДНК