- Dermatology. Skin and soft tissue infections dermatitis

Содержание
- 2. ATOPIC DERMATITIS itch usually a family history of atopy trigger factors Dust mite (common) Sweating Sand
- 3. ATOPIC DERMATITIS Criteria for diagnosis Itch Typical morphology and distribution Dry skin History of atopy Chronic
- 4. ATOPIC DERMATITIS ATOPIC STIGMATA Keratosis palmaris Dennie – Morgan fold Hertoghen’s sign Pityriasis Alba Palmar Hyperlinearity
- 5. ATOPIC DERMATITIS Management Education and reassurance Avoid irritants Improve skin condition Medication Topical corticosteroid therapy Topical
- 6. LICHEN SIMPLEX CHRONICUS Circumscribed thick plaques of lichenification Caused by repeated rubbing and scratching of previously
- 7. CONTACT DERMATITIS Site and shape suggest contact Dermatitis ranges from faint erythema to ‘water melon’ face
- 8. CONTACT DERMATITIS PATCH TEST
- 9. STASIS DERMATITIS risk factors: varicose veins high blood pressure obesity, vein surgeries multiple pregnancies a history
- 10. STASIS DERMATITIS clinical features: Bilateral redness in lighter skin tones that may appear brown, purple, gray
- 11. STASIS DERMATITIS Treatment compression stockings diuretics elevating legs above the heart for red or darker-colored, itchy
- 12. SEBORRHEIC DERMATITIS Adults Any age from teenage onwards Quite pruritic The head is a common area:
- 13. Kids Age of onset Mainly within first 3 months Itchiness Nil or mild Distribution Scalp, cheeks,
- 14. SEBORRHEIC DERMATITIS Management Likely to resolve on it’s own Soft baby brush and some baby oil
- 15. CELLULITIS Cellulitis is a common bacterial infection The most common bacteria causing cellulitis are Streptococcus pyogenes
- 16. CELLULITIS Erythematous, edematous and warm skin Risk factors: Anything that causes a break in the skin
- 17. CELLULITIS Treatment Non purulent: Cephalexin Cefazolin Purulent: TMP, Clindamycin or Tetracyclines Systemically ‘’toxic’’ – vancomycin or
- 18. OSTEOMYELITIS is mainly a disease of childhood Main organisms—S. aureus, S. pneumonia, Kingella kingae, Propionibacterium acnes
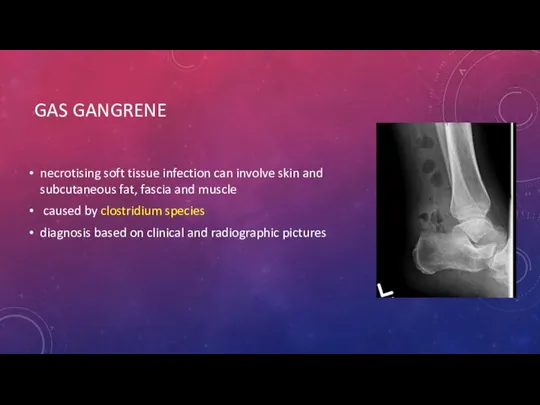
- 19. GAS GANGRENE necrotising soft tissue infection can involve skin and subcutaneous fat, fascia and muscle caused
- 20. GAS GANGRENE Clinical features sweet smelling odor edema, discoloration, ecchymosis blebs and hemorrhagic bullae ''dishwater pus''
- 21. GAS GANGRENE Management Debridement and excision with possible amputation Start benzylpenicillin 2.4 g IV, 4 hourly
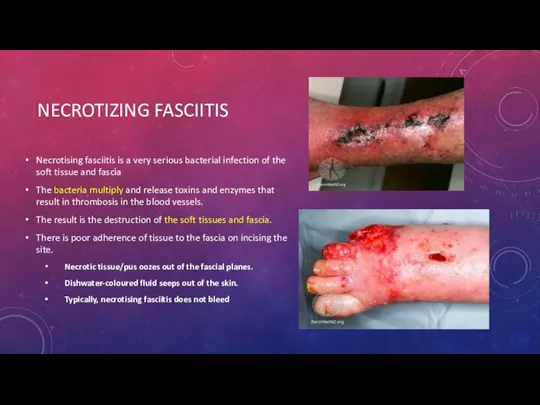
- 22. NECROTIZING FASCIITIS Necrotising fasciitis is a very serious bacterial infection of the soft tissue and fascia
- 23. NECROTIZING FASCIITIS Treatment Immediate surgical debridement The third generation cephalosporins + Clinda
- 24. IMPETIGO caused by Streptococcus pyogenes or Staphylococcus aureus kids honey crusted lesions on the face Treatment
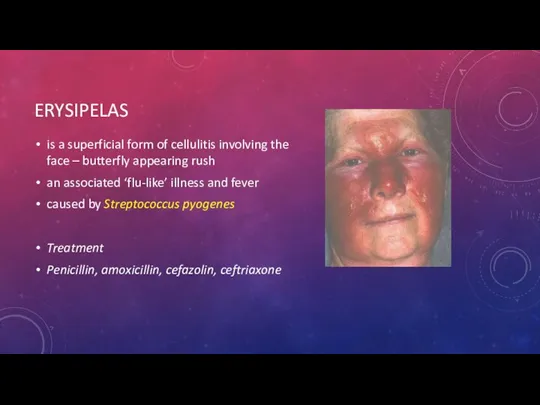
- 25. ERYSIPELAS is a superficial form of cellulitis involving the face – butterfly appearing rush an associated
- 26. DIFFERENTIAL DIAGNOSIS
- 27. TINEA Tinea pedis (Athlete’s foot) Red, itchy feet, maceration in between the toes Tinea cruris Jock
- 28. CELLULITIS Deep dermis and subcutaneous adipose tissue Indolent onset Localised symptoms Non-purulent or purulent Non-purulent: Beta-hemolytic
- 32. Скачать презентацию
ATOPIC DERMATITIS
itch
usually a family history of atopy
trigger factors
Dust mite
ATOPIC DERMATITIS
itch
usually a family history of atopy
trigger factors
Dust mite
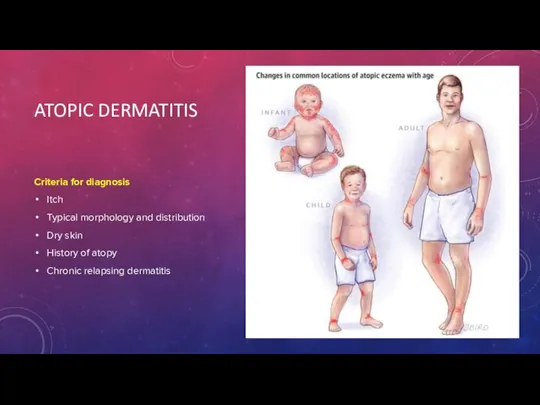
ATOPIC DERMATITIS
Criteria for diagnosis
Itch
Typical morphology and distribution
Dry skin
History of atopy
Chronic
ATOPIC DERMATITIS
Criteria for diagnosis
Itch
Typical morphology and distribution
Dry skin
History of atopy
Chronic
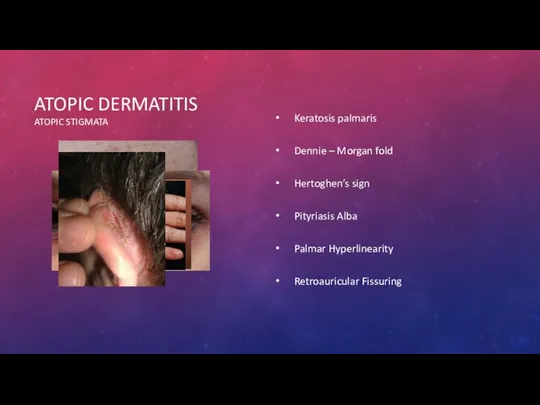
ATOPIC DERMATITIS
ATOPIC STIGMATA
Keratosis palmaris
Dennie – Morgan fold
Hertoghen’s sign
Pityriasis Alba
Palmar Hyperlinearity
Retroauricular
ATOPIC DERMATITIS
ATOPIC STIGMATA
Keratosis palmaris
Dennie – Morgan fold
Hertoghen’s sign
Pityriasis Alba
Palmar Hyperlinearity
Retroauricular
ATOPIC DERMATITIS
Management
Education and reassurance
Avoid irritants
Improve skin condition
Medication
Topical corticosteroid therapy
Topical calcineurin inhibitors
ATOPIC DERMATITIS
Management
Education and reassurance
Avoid irritants
Improve skin condition
Medication
Topical corticosteroid therapy
Topical calcineurin inhibitors
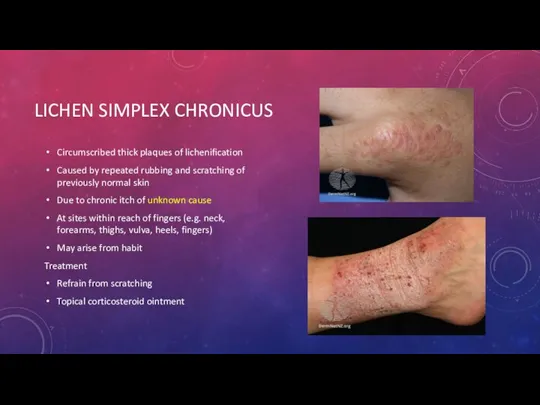
LICHEN SIMPLEX CHRONICUS
Circumscribed thick plaques of lichenification
Caused by repeated rubbing and
LICHEN SIMPLEX CHRONICUS
Circumscribed thick plaques of lichenification
Caused by repeated rubbing and
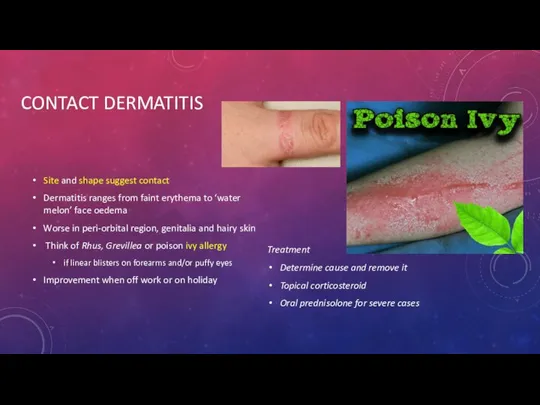
CONTACT DERMATITIS
Site and shape suggest contact
Dermatitis ranges from faint erythema to
CONTACT DERMATITIS
Site and shape suggest contact
Dermatitis ranges from faint erythema to

CONTACT DERMATITIS
PATCH TEST
CONTACT DERMATITIS
PATCH TEST
STASIS DERMATITIS
risk factors:
varicose veins
high blood pressure
obesity, vein surgeries
multiple pregnancies
a history of
STASIS DERMATITIS
risk factors:
varicose veins
high blood pressure
obesity, vein surgeries
multiple pregnancies
a history of
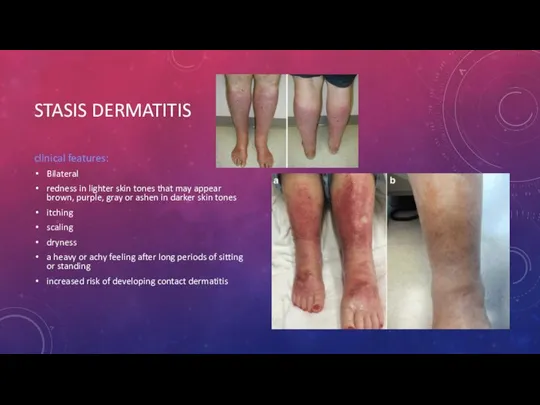
STASIS DERMATITIS
clinical features:
Bilateral
redness in lighter skin tones that may appear
STASIS DERMATITIS
clinical features:
Bilateral
redness in lighter skin tones that may appear
STASIS DERMATITIS
Treatment
compression stockings
diuretics
elevating legs above the heart
for red or
STASIS DERMATITIS
Treatment
compression stockings
diuretics
elevating legs above the heart
for red or
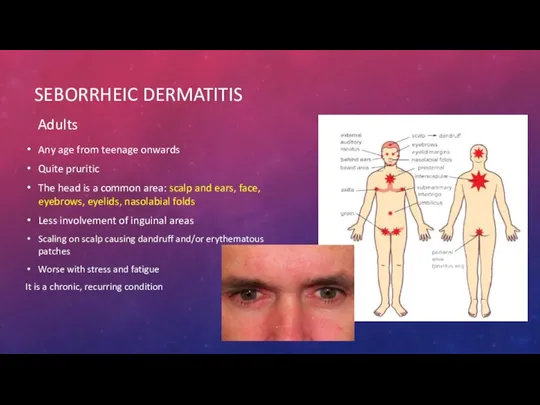
SEBORRHEIC DERMATITIS
Adults
Any age from teenage onwards
Quite pruritic
The head is a common
SEBORRHEIC DERMATITIS
Adults
Any age from teenage onwards
Quite pruritic
The head is a common
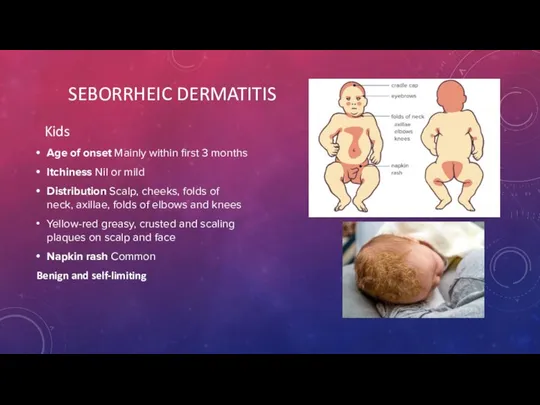
Kids
Age of onset Mainly within first 3 months
Itchiness Nil or
Kids
Age of onset Mainly within first 3 months
Itchiness Nil or
SEBORRHEIC DERMATITIS
Management
Likely to resolve on it’s own
Soft baby brush and some
SEBORRHEIC DERMATITIS
Management
Likely to resolve on it’s own
Soft baby brush and some
CELLULITIS
Cellulitis is a common bacterial infection
The most common bacteria causing cellulitis
CELLULITIS
Cellulitis is a common bacterial infection
The most common bacteria causing cellulitis
CELLULITIS
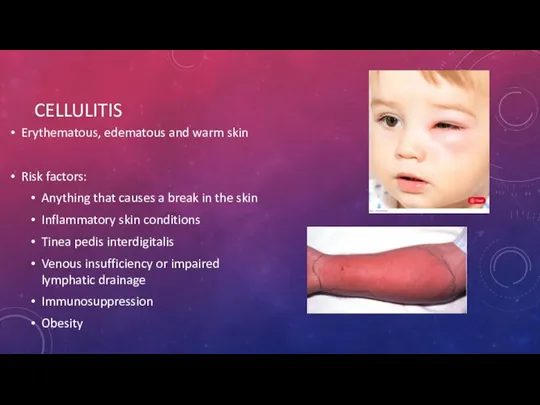
Erythematous, edematous and warm skin
Risk factors:
Anything that causes a break in
CELLULITIS
Erythematous, edematous and warm skin
Risk factors:
Anything that causes a break in
CELLULITIS
Treatment
Non purulent: Cephalexin Cefazolin
Purulent: TMP, Clindamycin or Tetracyclines
Systemically ‘’toxic’’ – vancomycin
CELLULITIS
Treatment
Non purulent: Cephalexin Cefazolin
Purulent: TMP, Clindamycin or Tetracyclines
Systemically ‘’toxic’’ – vancomycin
OSTEOMYELITIS
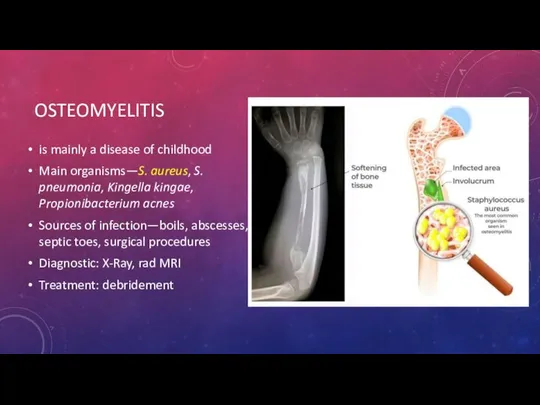
is mainly a disease of childhood
Main organisms—S. aureus, S. pneumonia, Kingella
OSTEOMYELITIS
is mainly a disease of childhood
Main organisms—S. aureus, S. pneumonia, Kingella
GAS GANGRENE
necrotising soft tissue infection can involve skin and subcutaneous fat,
GAS GANGRENE
necrotising soft tissue infection can involve skin and subcutaneous fat,

GAS GANGRENE
Clinical features
sweet smelling odor
edema, discoloration, ecchymosis
blebs and hemorrhagic bullae
''dishwater pus''
GAS GANGRENE
Clinical features
sweet smelling odor
edema, discoloration, ecchymosis
blebs and hemorrhagic bullae
''dishwater pus''
GAS GANGRENE
Management
Debridement and excision with possible amputation
Start benzylpenicillin 2.4 g IV,
GAS GANGRENE
Management
Debridement and excision with possible amputation
Start benzylpenicillin 2.4 g IV,
NECROTIZING FASCIITIS
Necrotising fasciitis is a very serious bacterial infection of the
NECROTIZING FASCIITIS
Necrotising fasciitis is a very serious bacterial infection of the

NECROTIZING FASCIITIS
Treatment
Immediate surgical debridement
The third generation cephalosporins
+ Clinda
NECROTIZING FASCIITIS
Treatment
Immediate surgical debridement
The third generation cephalosporins
+ Clinda

IMPETIGO
caused by Streptococcus pyogenes or Staphylococcus aureus
kids
honey crusted lesions on the
IMPETIGO
caused by Streptococcus pyogenes or Staphylococcus aureus
kids
honey crusted lesions on the
ERYSIPELAS
is a superficial form of cellulitis involving the face – butterfly
ERYSIPELAS
is a superficial form of cellulitis involving the face – butterfly

DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
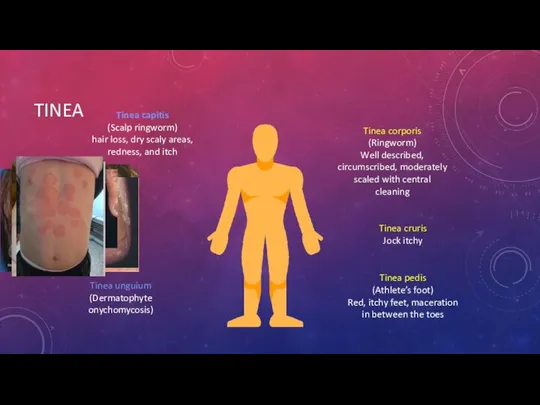
TINEA
Tinea pedis
(Athlete’s foot)
Red, itchy feet, maceration in between the toes
Tinea cruris
TINEA
Tinea pedis
(Athlete’s foot)
Red, itchy feet, maceration in between the toes
Tinea cruris
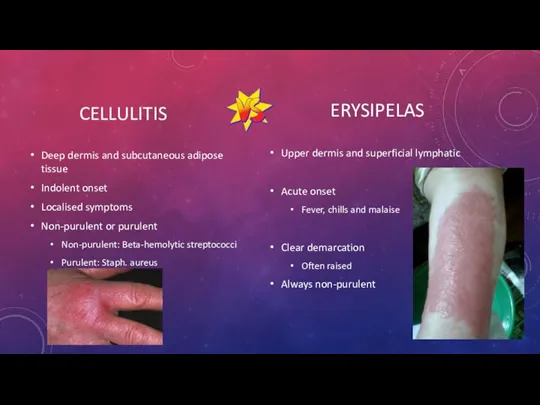
CELLULITIS
Deep dermis and subcutaneous adipose tissue
Indolent onset
Localised symptoms
Non-purulent or purulent
Non-purulent: Beta-hemolytic
CELLULITIS
Deep dermis and subcutaneous adipose tissue
Indolent onset
Localised symptoms
Non-purulent or purulent
Non-purulent: Beta-hemolytic


 Патофизиология и диагностика вегетативных и коматозных состояний
Патофизиология и диагностика вегетативных и коматозных состояний Дентикюр. Забота о зубах и деснах
Дентикюр. Забота о зубах и деснах Коронaвирус Covid-19
Коронaвирус Covid-19 Врожденная краснуха
Врожденная краснуха Стерильные лекарственные формы, изготавливаемые в условиях аптеки и промышленного производства
Стерильные лекарственные формы, изготавливаемые в условиях аптеки и промышленного производства Periconception endogenous and exogenous maternal sex steroid hormones and risk of asthma and allergy in offspring
Periconception endogenous and exogenous maternal sex steroid hormones and risk of asthma and allergy in offspring История развития донорства
История развития донорства Алгоритм работы при отработке заболевших Сovid-19
Алгоритм работы при отработке заболевших Сovid-19 Психомоторное развитие на первом году жизни
Психомоторное развитие на первом году жизни Операции на сухожилиях, костях, суставах, мягких тканях
Операции на сухожилиях, костях, суставах, мягких тканях Мама-Судьба
Мама-Судьба Аспекты эндокринологии в практике кардиолога
Аспекты эндокринологии в практике кардиолога Халықтың табиғи қозғалысын бағалау
Халықтың табиғи қозғалысын бағалау Самоменеджмент пациентов и его роль в ПУЗ
Самоменеджмент пациентов и его роль в ПУЗ Новые методы в санитарно-гигиенических исследованиях
Новые методы в санитарно-гигиенических исследованиях Первая помощь и правила иммобилизации при переломах черепа, позвоночника и таза
Первая помощь и правила иммобилизации при переломах черепа, позвоночника и таза Точечный массаж
Точечный массаж Физиология психической деятельности. Лекция 12
Физиология психической деятельности. Лекция 12 Тромбофилия. Заболевания, связанные с генетическими дефектами
Тромбофилия. Заболевания, связанные с генетическими дефектами Курс по восстановлению и уходу за волосами
Курс по восстановлению и уходу за волосами Основы патологии
Основы патологии Общая артрология
Общая артрология Нейропсихологическая диагностика детей раннего возраста. Зачем нужна нейропсихологическая диагностика детям в 2 года?
Нейропсихологическая диагностика детей раннего возраста. Зачем нужна нейропсихологическая диагностика детям в 2 года? Психическое развитие в младенчестве
Психическое развитие в младенчестве Энурез у детей
Энурез у детей Caries (clinical application)
Caries (clinical application) Школьный возраст
Школьный возраст «Өзін-өзі тану» рухани-адамгершілік білім бағдарламасының психологиялық-педагогикалық негіздері
«Өзін-өзі тану» рухани-адамгершілік білім бағдарламасының психологиялық-педагогикалық негіздері