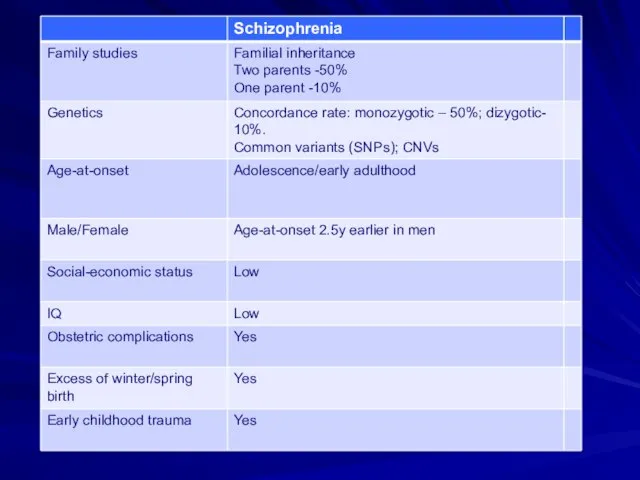
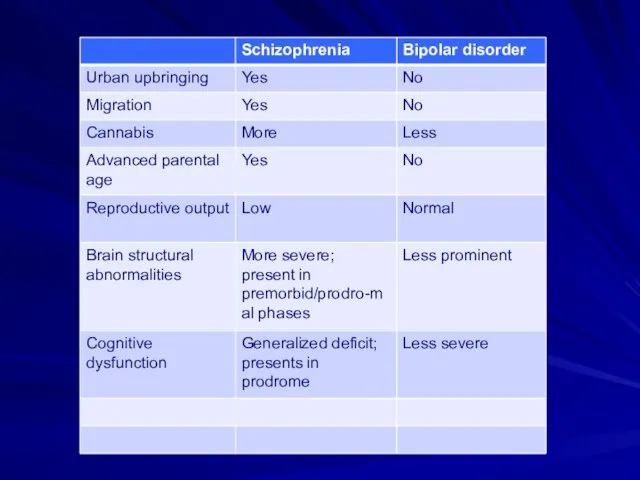
- Schizophrenia. Environmental factors

Содержание
- 3. Environmental factors
- 4. Age of onset and peak of mental disorders Nat Rev Neurosci (2), & 2008
- 6. Schizophrenia: inheritance
- 7. Manhattan plot showing schizophrenia associations S Ripke et al. Nature 1-7 (2014)
- 8. Subdivision of Symptoms into Three Dimensions Psychotic Delusions Hallucinations Disorganized Disorganized speech Disorganized behavior Inappropriate affect
- 9. Types of Hallucinations Auditory Visual Tactile Olfactory
- 10. Types of Delusions Persecutory Grandiose Religious Jealous Somatic
- 11. DSM-5 Criteria for Schizophrenia: The Basics Characteristic symptoms for one month Social/Occupational Dysfunction Overall Duration >
- 12. Differential Diagnosis Mood Disorders Nonpsychotic personality disorders Substance-induced psychotic disorders Psychotic disorders due to a general
- 13. Drugs That May Induce Psychosis Amphetamines Marijuana Hallucinogens Cocaine Cannabis
- 14. Medical Conditions That May Present with Psychosis Temporal lobe epilepsy Tumor Stroke Trauma Endocrine/metabolic abnormalities Infections
- 15. The Dopamine Hypothesis Psychosis (schizophrenia?) is due to excessive dopaminergic tone Psychotic symptoms are relieved by
- 16. Copyright restrictions may apply. Howes, O. D. et al. Arch Gen Psychiatry 2012;0:archgenpsychiatry.2012.169v1-11. Schematic diagram summarizing
- 19. Brain Regions Showing Replicable Neuropathological Abnormalities Temporolimbic regions Thalamus Prefrontal cortex
- 20. Neuropil in Frontal Cortex
- 22. Criterion A: Characteristic Symptoms At least two of the following, each present for a significant portion
- 23. Gender Differences Males have an earlier age at onset, a poorer premorbid history, more negative symptoms,
- 24. Important Epidemiolgical Observations Prevalence is not highly variable over time or over geographical areas Found in
- 25. Bleuler’s Fundamental Symptoms Associations Affective Blunting Avolition Autism Ambivalence Attention
- 26. Schneider: The Psychotic Experience Interested in pathognomonic symptoms “First Rank Symptoms” (FRS) E.g., voices commenting Voices
- 27. Characteristic Symptoms Schneider: specific types of delusions and hallucinations Bleuler: fragmented thinking, inability to relate to
- 28. Criterion B: Social/Occupational Dysfunction For a significant portion of the time since the onset of the
- 29. Criterion C: Overall Duration Continuous signs of the disturbance persist for at least six months This
- 30. Criterion D: Schizoaffective and Mood Disorder Exclusion Schizoaffective Disorder and Mood Disorder with Psychotic Features have
- 31. Criterion E: Substance / General Medical Condition Exclusion The disturbance is not due to the direct
- 32. DSM 5: Categories of Psychosis Schizophreniform Disorder Schizophrenia Brief Psychotic Disorder Schizoaffective Disorder Delusional Disorder Shared
- 33. Poor Outcome: Predictors Prominent negative symptoms Early age of onset Insidious onset Poor premorbid adjustment Low
- 35. Lower Social Class in Schizophrenia Consistently observed in patients Lower social class is a result—not a
- 36. Genetic Questions Is the disorder familial? Relative contributions of genes and environment Mode of transmission Location
- 37. Genetic Methods Family history studies Family studies Twin studies Adoption studies Linkage and association studies, candidate
- 38. Manhattan plot showing schizophrenia associations S Ripke et al. Nature 1-7 (2014)
- 39. Family History and Family Studies Provide evidence for a modest level of familial transmission Morbid risk
- 40. Possible Reasons for Lack of Measurable Abnormalities Problems in defining the phenotype No single pathophysiology Due
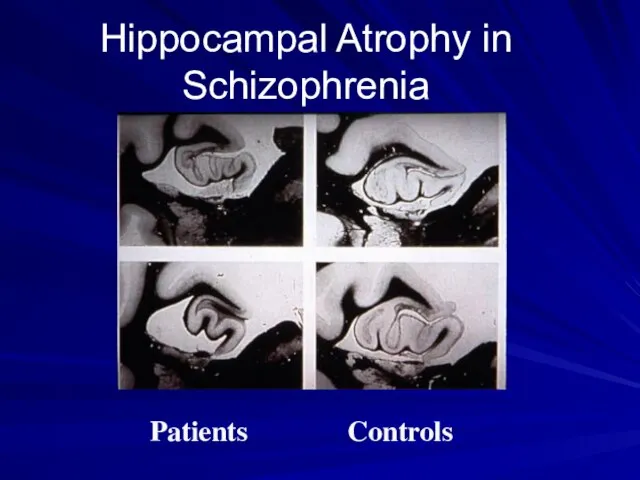
- 41. Hippocampal Atrophy in Schizophrenia Patients Controls
- 42. Thalamic Nuclei
- 43. A Neurodevelopmental Disorder: Supporting Evidence from Neuropathology Absence of gliosis Abnormal cytoarchitecture Visible markers of neurodevelopmental
- 44. Classified Images Continuous Discrete
- 45. MR Studies: Brain Abnormalities Decreased temporal lobe size Decreased frontal lobe size Decreased hippocampal size Decreased
- 46. A Neurodevelopmental Brain Disease Most brain abnormalities are present at onset: e.g., decrease in total brain
- 47. Increased Blood Flow in Striatum due to Chronic Dopamine Blockade by Haloperidol
- 48. Functional Imaging Tools Single Photon Emission Computed Tomography (SPECT) Positron Emission Tomography (PET) Functional Magnetic Resonance
- 49. Conclusions from PET Studies Schizophrenia is not a disease of a single brain region Areas of
- 50. The fMR Blood Flow Signal
- 51. Verbal Fluency Patients Controls
- 52. The N-Back Task for fMR Probe x x Target Experimental Task (2-Back): Remember the Probe and
- 53. 2-Back Task in Normals Bilateral dorsolateral frontal Bilateral parietal Anterior cingulate
- 54. 2-Back Task in Schizophrenia (unmedicated) Blood flow markedly decreased or absent in regions used by normals
- 55. Sensory Gating A problem in filtering or gating information Leads to the subject experience of being
- 56. Cognitive Dysmetria A defect in coordinating mental activity Due to disturbed functional connectivity between the cortex
- 58. Simplified Summary of Various Anatomical Refinements of the Dopamine Hypotheses of Schizophrenia Laruelle, Biol psychiatry 2013;74:80–81
- 59. Copyright restrictions may apply. Howes, O. D. et al. Arch Gen Psychiatry 2012;0:archgenpsychiatry.2012.169v1-11. Schematic diagram summarizing
- 60. Multiple hits interact to result in (1) striatal dopamine dysregulation to alter (2) the appraisal of
- 63. The Essence of Schizophrenia Originally called “dementia praecox” Produces severe incapacity – “dementia” Typically begins in
- 64. Kraepelin: Course and Outcome Split “dementia praecox” from manic-depressive illness Early onset Marked deterioration Chronic course
- 65. Fundamental Questions about Schizophrenia What are the characteristic symptoms? What are the boundaries of the concept?
- 66. Lifetime Prevalence What proportion of the population will develop the disorder at some time during their
- 74. Скачать презентацию
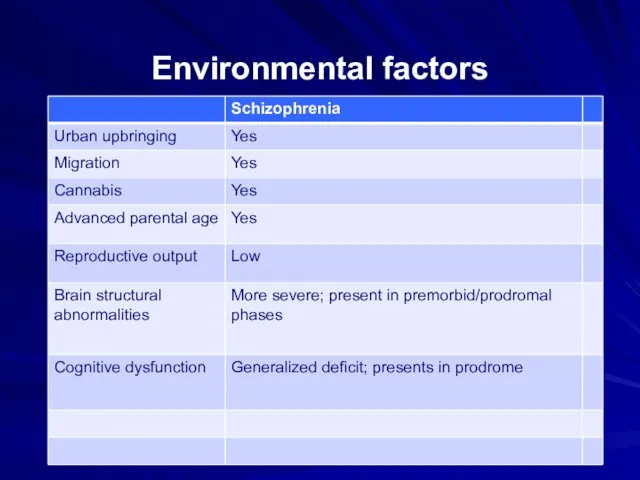
Environmental factors
Environmental factors
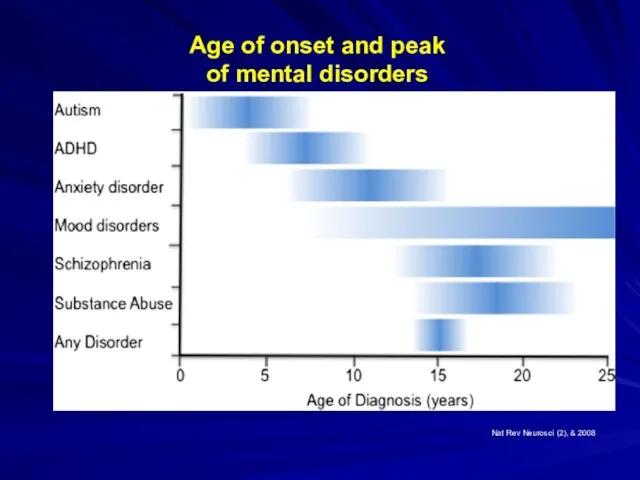
Age of onset and peak
of mental disorders
Nat Rev Neurosci (2),
Age of onset and peak
of mental disorders
Nat Rev Neurosci (2),

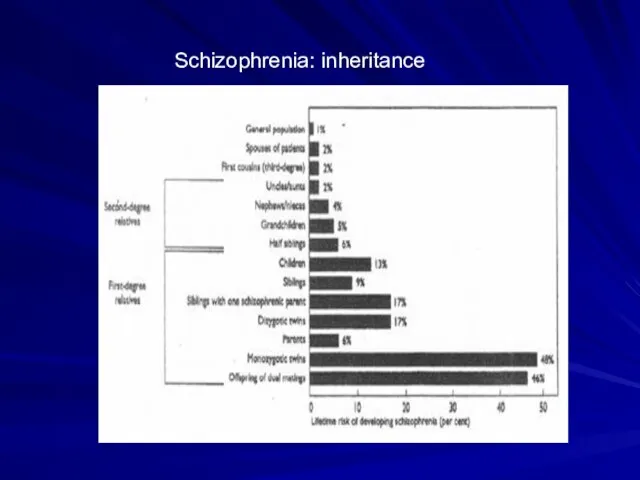
Schizophrenia: inheritance
Schizophrenia: inheritance
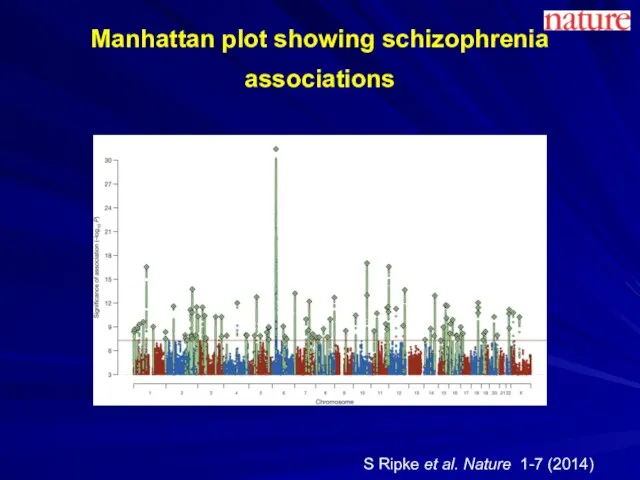
Manhattan plot showing schizophrenia associations
S Ripke et al. Nature 1-7
Manhattan plot showing schizophrenia associations
S Ripke et al. Nature 1-7
Subdivision of Symptoms into Three Dimensions
Psychotic
Delusions
Hallucinations
Disorganized
Disorganized speech
Disorganized behavior
Inappropriate affect
Negative
Poverty of speech
Avolition
Affective
Subdivision of Symptoms into Three Dimensions
Psychotic
Delusions
Hallucinations
Disorganized
Disorganized speech
Disorganized behavior
Inappropriate affect
Negative
Poverty of speech
Avolition
Affective

Types of Hallucinations
Auditory
Visual
Tactile
Olfactory
Types of Hallucinations
Auditory
Visual
Tactile
Olfactory

Types of Delusions
Persecutory
Grandiose
Religious
Jealous
Somatic
Types of Delusions
Persecutory
Grandiose
Religious
Jealous
Somatic
DSM-5 Criteria for Schizophrenia: The Basics
Characteristic symptoms for one month
Social/Occupational Dysfunction
Overall
DSM-5 Criteria for Schizophrenia: The Basics
Characteristic symptoms for one month
Social/Occupational Dysfunction
Overall
Differential Diagnosis
Mood Disorders
Nonpsychotic personality disorders
Substance-induced psychotic disorders
Psychotic disorders due to a
Differential Diagnosis
Mood Disorders
Nonpsychotic personality disorders
Substance-induced psychotic disorders
Psychotic disorders due to a

Drugs That May Induce Psychosis
Amphetamines
Marijuana
Hallucinogens
Cocaine
Cannabis
Drugs That May Induce Psychosis
Amphetamines
Marijuana
Hallucinogens
Cocaine
Cannabis
Medical Conditions That May Present with Psychosis
Temporal lobe epilepsy
Tumor
Stroke
Trauma
Endocrine/metabolic abnormalities
Infections
Multiple Sclerosis
Autoimmune
Medical Conditions That May Present with Psychosis
Temporal lobe epilepsy
Tumor
Stroke
Trauma
Endocrine/metabolic abnormalities
Infections
Multiple Sclerosis
Autoimmune
The Dopamine Hypothesis
Psychosis (schizophrenia?) is due to excessive dopaminergic tone
Psychotic symptoms
The Dopamine Hypothesis
Psychosis (schizophrenia?) is due to excessive dopaminergic tone
Psychotic symptoms

Copyright restrictions may apply.
Howes, O. D. et al. Arch Gen Psychiatry
Copyright restrictions may apply.
Howes, O. D. et al. Arch Gen Psychiatry



Brain Regions Showing Replicable Neuropathological Abnormalities
Temporolimbic regions
Thalamus
Prefrontal cortex
Brain Regions Showing Replicable Neuropathological Abnormalities
Temporolimbic regions
Thalamus
Prefrontal cortex

Neuropil in Frontal Cortex
Neuropil in Frontal Cortex
Criterion A: Characteristic Symptoms
At least two of the following, each present
Criterion A: Characteristic Symptoms
At least two of the following, each present

Gender Differences
Males have an earlier age at onset, a poorer premorbid
Gender Differences
Males have an earlier age at onset, a poorer premorbid
Important Epidemiolgical Observations
Prevalence is not highly variable over time or over
Important Epidemiolgical Observations
Prevalence is not highly variable over time or over
Bleuler’s Fundamental Symptoms
Associations
Affective Blunting
Avolition
Autism
Ambivalence
Attention
Bleuler’s Fundamental Symptoms
Associations
Affective Blunting
Avolition
Autism
Ambivalence
Attention

Schneider: The Psychotic Experience
Interested in pathognomonic symptoms
“First Rank Symptoms” (FRS)
E.g., voices
Schneider: The Psychotic Experience
Interested in pathognomonic symptoms
“First Rank Symptoms” (FRS)
E.g., voices
Characteristic Symptoms
Schneider: specific types of delusions and hallucinations
Bleuler: fragmented thinking, inability
Characteristic Symptoms
Schneider: specific types of delusions and hallucinations
Bleuler: fragmented thinking, inability

Criterion B: Social/Occupational Dysfunction
For a significant portion of the time since
Criterion B: Social/Occupational Dysfunction
For a significant portion of the time since

Criterion C: Overall Duration
Continuous signs of the disturbance persist for at
Criterion C: Overall Duration
Continuous signs of the disturbance persist for at
Criterion D: Schizoaffective and Mood Disorder Exclusion
Schizoaffective Disorder and Mood Disorder
Criterion D: Schizoaffective and Mood Disorder Exclusion
Schizoaffective Disorder and Mood Disorder

Criterion E: Substance / General Medical Condition Exclusion
The disturbance is not
Criterion E: Substance / General Medical Condition Exclusion
The disturbance is not

DSM 5: Categories of Psychosis
Schizophreniform Disorder
Schizophrenia
Brief Psychotic Disorder
Schizoaffective Disorder
Delusional Disorder
Shared Psychotic
DSM 5: Categories of Psychosis
Schizophreniform Disorder
Schizophrenia
Brief Psychotic Disorder
Schizoaffective Disorder
Delusional Disorder
Shared Psychotic

Poor Outcome: Predictors
Prominent negative symptoms
Early age of onset
Insidious onset
Poor premorbid adjustment
Low
Poor Outcome: Predictors
Prominent negative symptoms
Early age of onset
Insidious onset
Poor premorbid adjustment
Low


Lower Social Class in Schizophrenia
Consistently observed in patients
Lower social class is
Lower Social Class in Schizophrenia
Consistently observed in patients
Lower social class is
Genetic Questions
Is the disorder familial?
Relative contributions of genes and environment
Mode of
Genetic Questions
Is the disorder familial?
Relative contributions of genes and environment
Mode of
Genetic Methods
Family history studies
Family studies
Twin studies
Adoption studies
Linkage and association studies, candidate
Genetic Methods
Family history studies
Family studies
Twin studies
Adoption studies
Linkage and association studies, candidate

Manhattan plot showing schizophrenia associations
S Ripke et al. Nature 1-7
Manhattan plot showing schizophrenia associations
S Ripke et al. Nature 1-7

Family History and Family Studies
Provide evidence for a modest level of
Family History and Family Studies
Provide evidence for a modest level of
Possible Reasons for Lack of Measurable Abnormalities
Problems in defining the
Possible Reasons for Lack of Measurable Abnormalities
Problems in defining the
Hippocampal Atrophy in Schizophrenia
Patients
Controls
Hippocampal Atrophy in Schizophrenia
Patients
Controls

Thalamic Nuclei
Thalamic Nuclei
A Neurodevelopmental Disorder: Supporting Evidence from Neuropathology
Absence of gliosis
Abnormal cytoarchitecture
Visible markers
A Neurodevelopmental Disorder: Supporting Evidence from Neuropathology
Absence of gliosis
Abnormal cytoarchitecture
Visible markers

Classified Images
Continuous
Discrete
Classified Images
Continuous
Discrete

MR Studies: Brain Abnormalities
Decreased temporal lobe size
Decreased frontal lobe size
Decreased hippocampal
MR Studies: Brain Abnormalities
Decreased temporal lobe size
Decreased frontal lobe size
Decreased hippocampal

A Neurodevelopmental Brain Disease
Most brain abnormalities are present at onset: e.g.,
A Neurodevelopmental Brain Disease
Most brain abnormalities are present at onset: e.g.,

Increased Blood Flow in Striatum due to Chronic Dopamine Blockade by
Increased Blood Flow in Striatum due to Chronic Dopamine Blockade by

Functional Imaging Tools
Single Photon Emission Computed Tomography (SPECT)
Positron Emission Tomography (PET)
Functional
Functional Imaging Tools
Single Photon Emission Computed Tomography (SPECT)
Positron Emission Tomography (PET)
Functional
Conclusions from PET Studies
Schizophrenia is not a disease of a single
Conclusions from PET Studies
Schizophrenia is not a disease of a single

The fMR Blood Flow Signal
The fMR Blood Flow Signal

Verbal Fluency
Patients
Controls
Verbal Fluency
Patients
Controls
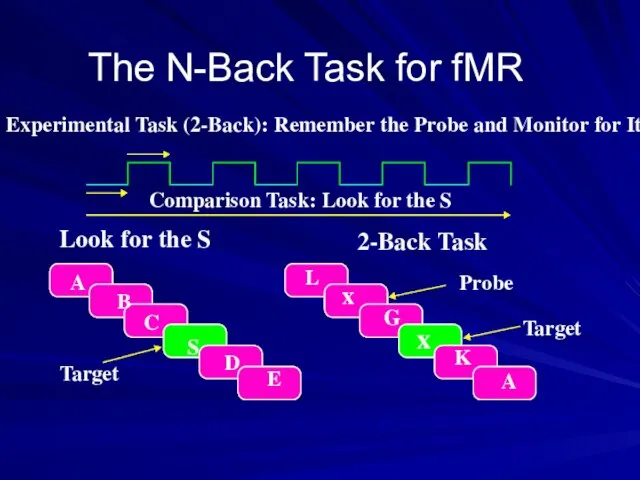
The N-Back Task for fMR
Probe
x
x
Target
Experimental Task (2-Back): Remember the Probe and
The N-Back Task for fMR
Probe
x
x
Target
Experimental Task (2-Back): Remember the Probe and

2-Back Task in Normals
Bilateral dorsolateral frontal
Bilateral parietal
Anterior cingulate
2-Back Task in Normals
Bilateral dorsolateral frontal
Bilateral parietal
Anterior cingulate

2-Back Task in Schizophrenia (unmedicated)
Blood flow markedly decreased or absent in
2-Back Task in Schizophrenia (unmedicated)
Blood flow markedly decreased or absent in
Sensory Gating
A problem in filtering or gating information
Leads to the subject
Sensory Gating
A problem in filtering or gating information
Leads to the subject

Cognitive Dysmetria
A defect in coordinating mental activity
Due to disturbed functional connectivity
Cognitive Dysmetria
A defect in coordinating mental activity
Due to disturbed functional connectivity


Simplified Summary of Various Anatomical Refinements of the Dopamine Hypotheses of
Simplified Summary of Various Anatomical Refinements of the Dopamine Hypotheses of

Copyright restrictions may apply.
Howes, O. D. et al. Arch Gen Psychiatry
Copyright restrictions may apply.
Howes, O. D. et al. Arch Gen Psychiatry

Multiple hits interact to result in (1) striatal dopamine dysregulation to
Multiple hits interact to result in (1) striatal dopamine dysregulation to

The Essence of Schizophrenia
Originally called “dementia praecox”
Produces severe incapacity – “dementia”
Typically
The Essence of Schizophrenia
Originally called “dementia praecox”
Produces severe incapacity – “dementia”
Typically

Kraepelin: Course and Outcome
Split “dementia praecox” from manic-depressive illness
Early onset
Marked deterioration
Chronic
Kraepelin: Course and Outcome
Split “dementia praecox” from manic-depressive illness
Early onset
Marked deterioration
Chronic
Fundamental Questions about Schizophrenia
What are the characteristic symptoms?
What are the boundaries
Fundamental Questions about Schizophrenia
What are the characteristic symptoms?
What are the boundaries

Lifetime Prevalence
What proportion of the population will develop the disorder at
Lifetime Prevalence
What proportion of the population will develop the disorder at






 Бронхіти у дітей
Бронхіти у дітей Амбулаторное лечение. Снижение гинекологических заболевании
Амбулаторное лечение. Снижение гинекологических заболевании Туберкулёз и его последствия
Туберкулёз и его последствия Болезнь Штрюмпеля. Семейный спастический паралич
Болезнь Штрюмпеля. Семейный спастический паралич Коффердам оптидам, жидкий коффердам
Коффердам оптидам, жидкий коффердам Иммунитет
Иммунитет Радиопротекторы. Радиопротекторы кратковременного, одномоментного действия
Радиопротекторы. Радиопротекторы кратковременного, одномоментного действия Синдром поликистозных яичников
Синдром поликистозных яичников Мышцы шеи и головы
Мышцы шеи и головы Гострі кишкові інфекції. Черевний тиф. Шигельоз. Харчові токсикоінфекції. Сальмонельоз. Ботулізм
Гострі кишкові інфекції. Черевний тиф. Шигельоз. Харчові токсикоінфекції. Сальмонельоз. Ботулізм Рентгеновское излучение
Рентгеновское излучение Миокард негізгі функцияларына әсер ететін. Дәрілік заттардың клиникалық фармакологиясы
Миокард негізгі функцияларына әсер ететін. Дәрілік заттардың клиникалық фармакологиясы Лечебно-профилактические мероприятия при микроспории кошек
Лечебно-профилактические мероприятия при микроспории кошек Панникулит. Предрасполагающими факторами к его развитию
Панникулит. Предрасполагающими факторами к его развитию Миокардиты
Миокардиты Нагноительные заболевания легких. Абсцесс и гангрена легкого
Нагноительные заболевания легких. Абсцесс и гангрена легкого Антибактериальная терапия пневмоний у лиц с иммунодефицитом
Антибактериальная терапия пневмоний у лиц с иммунодефицитом Меры правовой ответственности педагогического работника. Тема №1
Меры правовой ответственности педагогического работника. Тема №1 Паразиты
Паразиты Тұқым қуалайтын ауруларды емдеудің негізгі принциптері
Тұқым қуалайтын ауруларды емдеудің негізгі принциптері Изменение физических свойств при почечной патологии
Изменение физических свойств при почечной патологии Методы анализа белка в биологическом материале
Методы анализа белка в биологическом материале Визначення туберкульозу, як наукової та практичної проблеми. Історія розвитку фтизіатрії. (Лекція 1)
Визначення туберкульозу, як наукової та практичної проблеми. Історія розвитку фтизіатрії. (Лекція 1) Учение об эпидемическом процессе
Учение об эпидемическом процессе Анальгетики
Анальгетики Употребление и зависимость от препаратов конопли
Употребление и зависимость от препаратов конопли Ирригоскопия - жуан ішек препараттының ішіне ретроградты енгізумен ішектің рентгенологиялық зерттеу
Ирригоскопия - жуан ішек препараттының ішіне ретроградты енгізумен ішектің рентгенологиялық зерттеу Рак молочной железы
Рак молочной железы