- Data Collection of Primary Central Nervous System (CNS) Tumors

Содержание
- 2. Portions of this presentation are based on non-malignant CNS tumor data collection rules adopted by the
- 3. Part I Rationale History Definition of Reportable Cases Casefinding Anticipated Impact on Registries
- 4. Rationale for Non-malignant CNS Tumor Surveillance and Registration Non-malignant CNS tumors cause disruption in normal function
- 5. History 1992 -1996 1992 Central Brain Tumor Registry of the United States (CBTRUS) formed to report
- 6. History 1998 BTWG forwarded four recommendations to the NCCCS NCCCS Accepted recommendations 1 and 2 Deferred
- 7. BTWG Recommendations (1) The following standard definition is to be used for collecting precise data for
- 8. BTWG Recommendations (2) Develop a standard site and histology definition for tabulating estimates of CNS tumors
- 9. BTWG Recommendations (3) Develop training for reporting and tabulating primary intracranial and CNS tumors, and develop
- 10. History 2000 International Classification of Diseases for Oncology 3rd Edition (ICD-O-3) and World Health Organization (WHO)
- 11. History 2001-2002 2001 NCCCS Accepted Recommendations 1 and 2 as completed. Reconvened the BTWG to work
- 12. Reportable Brain-Related Tumors (1) Public Law 107-260 requires reporting of brain-related tumors. The term “brain-related tumor”
- 13. Reportable Brain-Related Tumors (2) Brain Cerebrum (C71.0) Frontal lobe (C71.1) Temporal lobe (C71.2) Parietal lobe (C71.3)
- 14. Reportable Brain-Related Tumors (3) Brain (continued) Ventricle (C71.5) Cerebellum (C71.6) Brain stem (C71.7) Overlapping lesion of
- 15. Reportable Brain-Related Tumors (4) Meninges Cerebral meninges (C70.0) Spinal meninges (C70.1) Meninges NOS (C70.9) Spinal cord
- 16. Reportable Brain-Related Tumors (5) Cranial nerves Olfactory nerve (C72.2) Optic nerve (C72.3) Acoustic nerve (C72.4) Cranial
- 17. Reportable Brain-Related Tumors (6) Other CNS (C72.8, C72.9) Pituitary gland (C75.1) Craniopharyngeal duct (C75.2) Pineal gland
- 18. History 2003 2003 SEER-supported registries and COC-approved hospital cancer registries will also report non-malignant CNS tumors
- 19. Impact of Collecting Data on Non-malignant CNS Tumors (1) Annual increase in number of cases estimated
- 20. Impact of Collecting Data on Non-malignant CNS Tumors (2) Central registry case load is estimated to
- 21. Impact of Collecting Data on Non-malignant CNS Tumors (3) Central registries adding non-malignant CNS tumors to
- 22. Impact of Collecting Data on Non-malignant CNS Tumors (4) All cancer registries must: Have the same
- 23. Case-finding (1) Additional or expanded case-finding mechanisms: Pathology Radiology Treatment facilities: Radiation oncology centers and departments
- 24. Case-finding (2) Disease indices Surgery logs Diagnostic imaging Radiation oncology Neurology clinics Medical oncology Autopsy reports.
- 25. Case-finding Sources Free-standing radiation therapy centers Free-standing Magnetic Resonance Imaging (MRI) centers Free-standing gamma or cyber
- 26. ICD-9-CM Codes for Case-finding
- 27. Unusual and Ambiguous Terminology If the final pathologic diagnosis is a CNS “neoplasm” or “mass”, an
- 28. Part II CNS Anatomy and Function Histologies and Primary Sites Grading Systems and Coding Grade
- 29. CNS Functional Anatomy Source: URL: www.solinas.com/solinas/brain.html accessed 7/18/03.
- 30. CNS Anatomy C71 C71.6 C71.7 C72.0 C71.0 C75.3 C75.1 C71.7 Source: URL: www.universalpeace.ca/principles.htm accessed 7/18/03.
- 31. Intracranial Sites C71.0 C71.6 C41.0 C71.7 C72.0 Source: URL: mscenter.ucsf.edu/faq.htm accessed 7/18/03. Parietal lobe Frontal lobe
- 32. Cerebrum C71.1 C71.2 C71.7 C71.3 C71.4 C71.6 C71.0 Source: URL: www.sciencebob.com/lab/bodyzone/brainprint.html Accessed 7/18/03.
- 33. Cerebellum and Brain Stem C71.0 C71.1 C71.2 C71.7 C71.3 C71.4 C71.6 URL: www.sciencebob.com/lab/bodyzone/brain.html 7/18/03
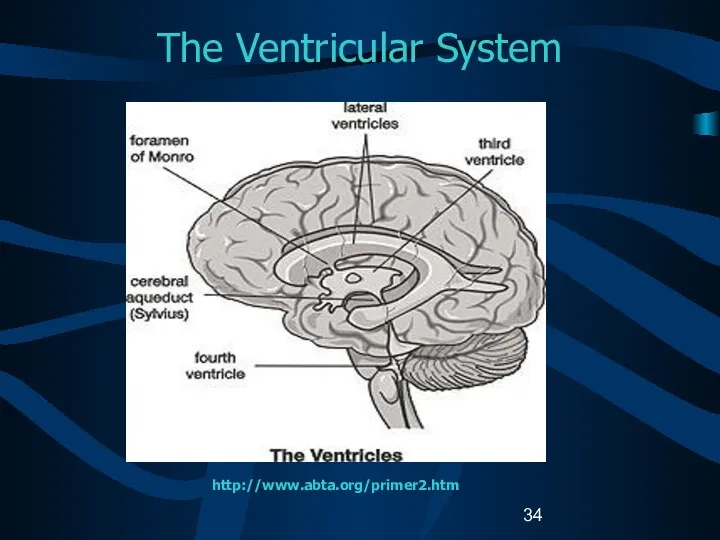
- 34. The Ventricular System http://www.abta.org/primer2.htm
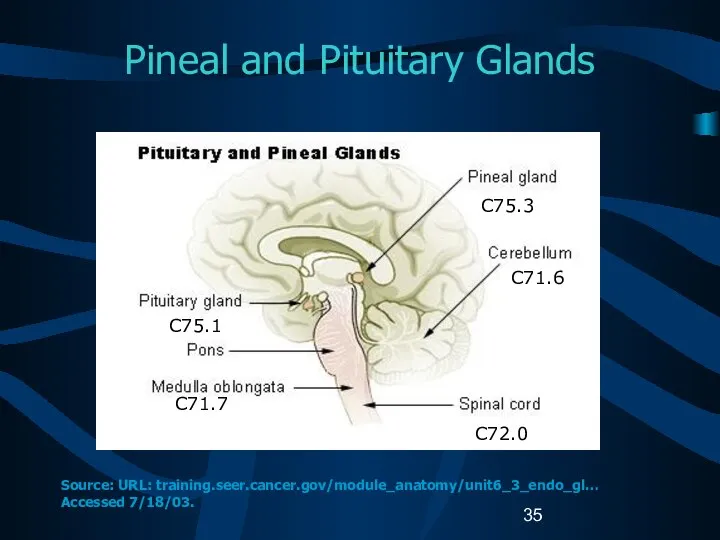
- 35. Pineal and Pituitary Glands C75.1 C71.7 C75.3 C71.6 C72.0 Source: URL: training.seer.cancer.gov/module_anatomy/unit6_3_endo_gl… Accessed 7/18/03.
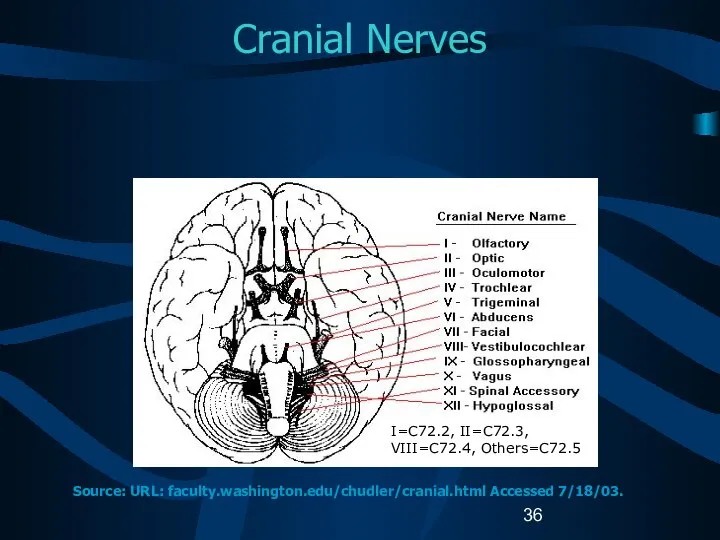
- 36. Cranial Nerves I=C72.2, II=C72.3, VIII=C72.4, Others=C72.5 Source: URL: faculty.washington.edu/chudler/cranial.html Accessed 7/18/03.
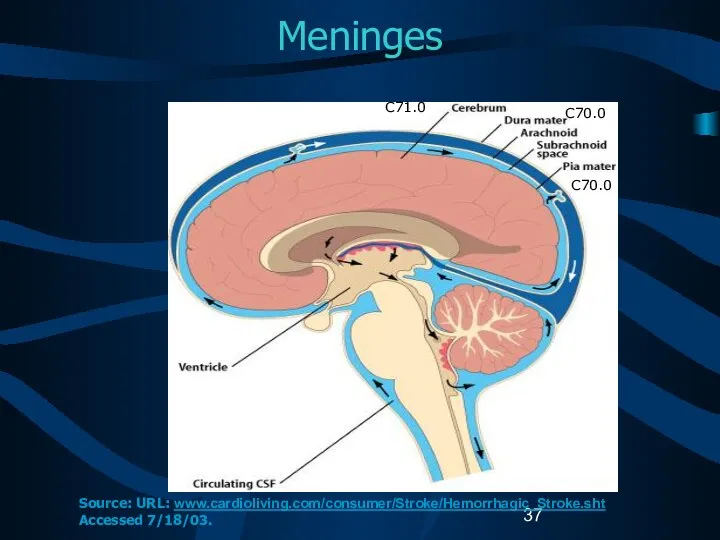
- 37. Meninges C71.0 C70.0 C70.0 Source: URL: www.cardioliving.com/consumer/Stroke/Hemorrhagic_Stroke.sht Accessed 7/18/03.
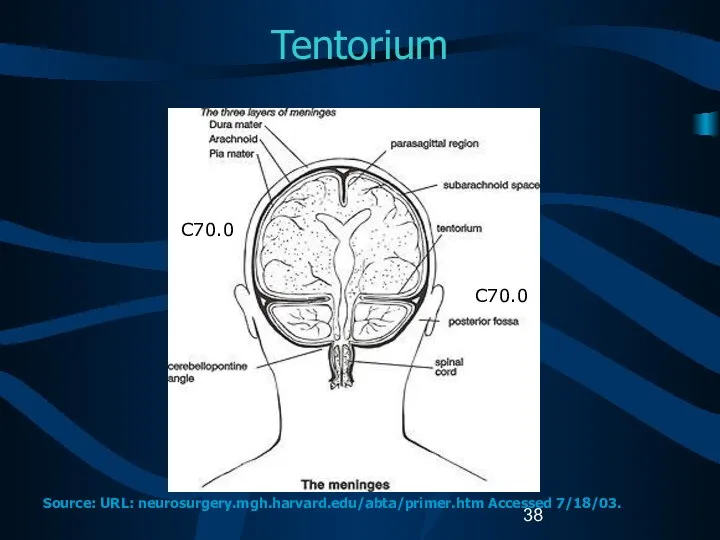
- 38. Tentorium C70.0 C70.0 Source: URL: neurosurgery.mgh.harvard.edu/abta/primer.htm Accessed 7/18/03.
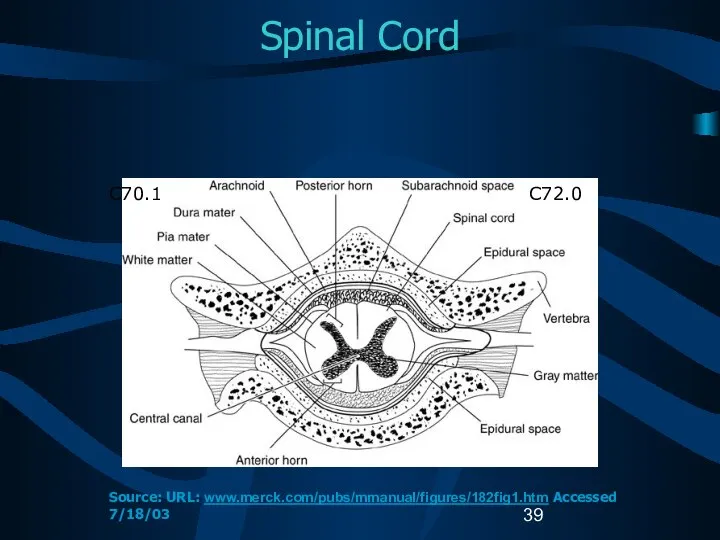
- 39. Spinal Cord C72.0 C70.1 Source: URL: www.merck.com/pubs/mmanual/figures/182fig1.htm Accessed 7/18/03
- 40. Cellular Classification Neuroepithelial tumors Astrocytomas Oligodendrogliomas Ependymomas Pineal parenchymal tumors Other CNS tumors Sellar tumors Hematopoetic
- 41. Glial Tumors (1) Glial tissue: supportive tissue of brain made up of astrocytes and oligodendrocytes Glial
- 42. Glial Tumors (2) Astrocytic tumors Noninfiltrating Juvenile pilocytic (M9421) Subependymal (M9383) Infiltrating Well-differentiated mildly and moderately
- 43. Glial Tumors (3) Ependymal tumors Myxopapillary and well-differentiated ependymomas (M9394) Anaplastic ependymomas (M9392) Ependymoblastomas (M9392) Oligodendroglial
- 44. Glial Tumors (4) Mixed tumors Mixed astrocytoma-ependymomas Mixed astrocytoma-oligodendrogliomas Mixed astrocytoma-ependymoma-oligodendrogliomas Other gliomas Ganglioneuromas (M9490) Optic
- 45. Non-Glial Tumors (1) Pineal region tumors Parenchymal tumors Pineocytomas (M9361) Pineoblastomas (M9362) Pineal astrocytomas (M9400) Germ
- 46. Non-Glial Tumors (2) Meningiomas Meningioma: Benign (M953_) Malignant meningiomas Anaplastic meningioma Hemangiopericytoma (M9150) Papillary meningioma (M9538)
- 47. Other CNS Tumors (1) Craniopharyngiomas (M9350) Rathke pouch tumors Chordomas (M9370) Schwannomas (M9560) Acoustic schwannomas/neuromas
- 48. Other CNS Tumors (2) Embryonal tumors Retinoblastomas (M9510) Primitive neuroectodermal tumors (PNETs) Meduloblastomas (M9470) Neuroblastomas (M9500)
- 49. Other CNS Tumors (3) Lymphomas (M9590) Arise from Indigenous brain histiocytes (microglia) Rare lymphocytes in meninges
- 50. Other CNS Tumors (4) Cysts and tumor-like lesions Reportable Dermoid cysts (M9084) Granular cell tumors (M9580)
- 51. Childhood versus Adult Tumors CNS tumor histology and location are different in adult and children. Tumor
- 52. Childhood Brain Tumors Meduloblastomas are the most common CNS histology in children. 50% are infratentorial. Common
- 53. Cellular Classification Childhood Brain Tumors (1) Supratentorial tumors in children Craniopharyngiomas Germ cell tumors Diencephalic and
- 54. Cellular Classification Childhood Brain Tumors (2) The histopathology of childhood spinal tumors is the same as
- 55. Cellular Classification Childhood CNS Tumors Cause of childhood CNS tumors remains unknown. American Academy of Pediatrics
- 56. ICD-O-3 Coding Issues (1) Some histologies may be difficult to determine if the primary site is
- 57. ICD-O-3 Coding Issues (2) Continue to assign histology code M9421/3 to pilocytic astrocytoma. When the primary
- 58. Grade for CNS Tumors Sixth digit of ICD-O-3 histology code Describes tumor differentiation or grade. Is
- 59. WHO Grade (1) WHO grade coded in Collaborative Stage data field: Site-specific factor 1 for Brain.
- 60. WHO Grade (2) Grade II Relatively slow growing Sometimes recur as higher grade tumors May be
- 61. Kernohan Grade Defines progressive malignancy for astrocytoma Grade 1: benign astrocytomas Grade 2: low-grade astrocytomas Grade
- 62. St. Anne-Mayo Grade (1) Used for astrocytomas. Uses four morphologic criteria: Nuclear atypia Mitosis Endothelial proliferation
- 63. St. Anne-Mayo Grade (2) Grade 1: No criteria Grade 2: One criterion, usually nuclear atypia Grade
- 64. Grade for CNS Tumors Do not record WHO grade, Kernohan grade, or St. Anne/Mayo grade in
- 65. Part III Laterality Multiple Primaries Malignant Transformation Sequence Numbers Date of Diagnosis
- 66. Determining Multiple Primaries: Laterality Brain is not a paired organ. Laterality collected on both non-malignant and
- 67. Coding Laterality (1) CNS sites to be coded with laterality: Cerebral meninges, NOS (C70.0) Cerebrum (C71.0)
- 68. Coding Laterality (2) CNS sites to be coded with laterality (continued): Olfactory nerve (C72.2) Optic nerve
- 69. Determining Multiple Primaries: Definitions Non-malignant tumor Tumor with ICD-O-3 behavior code 0 (benign) or 1 (borderline).
- 70. Determining Multiple Primaries Malignant (1) NO CHANGES (at this time) Site Rule: Each category (first three
- 71. Determining Multiple Primaries: Malignant (2) Histology Rule: Differences in histologic type refer to differences in the
- 72. Determining Multiple Primaries Non-malignant (1) NEW RULES Site Rule: Each sub-site (fourth-digit level) as delineated in
- 73. Determining Multiple Primaries Non-malignant (2) Site (cont) EXCEPT NOS (C_ _.9) with specific four-digit site code
- 74. Determining Multiple Primaries Non-malignant (3) Site (cont) Laterality: For non-malignant cases only If multiple tumors of
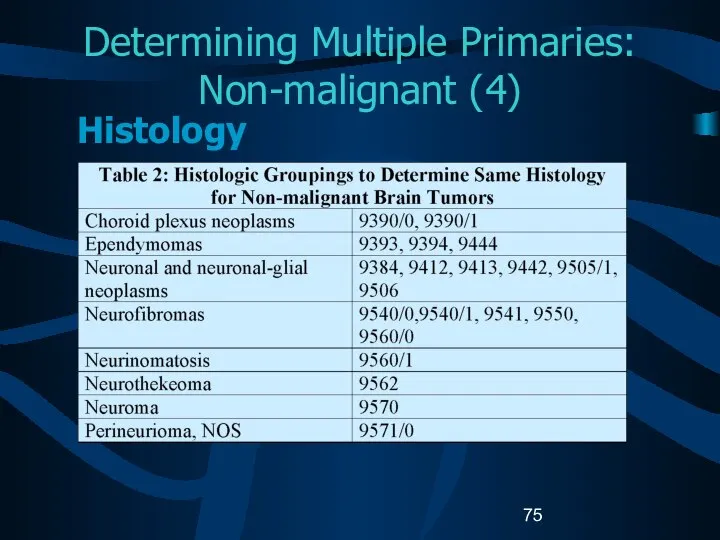
- 75. Determining Multiple Primaries: Non-malignant (4) Histology
- 76. Determining Multiple Primaries: Non-malignant (5) Histology If multiple tumors are in the same site, refer to
- 77. Determining Multiple Primaries: Non-malignant (6) Histology (cont.) B. If all histologies are listed in the same
- 78. Determining Multiple Primaries: Non-malignant (7) Histology (cont) C: If the first three digits are the same
- 79. Determining Multiple Primaries: Non-malignant (8) Histology (cont) D: If the first three digits are the same
- 80. Determining Multiple Primaries: Timing (1) Primary malignant CNS tumors NO CHANGE Malignant tumors of the same
- 81. Determining Multiple Primaries: Timing (2) Primary non-malignant CNS tumors NEW No timing rule If a new
- 82. General Rules for Determining Multiple Primaries of CNS Sites (1) Multiple lesions: all non-malignant If different
- 83. General Rules for Determining Multiple Primaries of CNS Sites (2) Multiple lesions: all non-malignant (cont.) If
- 84. General Rules for Determining Multiple Primaries of CNS Sites (3) Multiple tumors: One non-malignant and one
- 85. Histologic Transformation (1) Histologic transformation or progression to a higher grade: Determined by pathological review. Final
- 86. Histologic Transformation (2) If a malignant CNS tumor recurs (transforms) as a higher grade tumor, SAME
- 87. Histologic Transformation (3) Transformation of a non-malignant tumor to a malignant tumor is rare. Malignant transformations
- 88. Histologic Transformation (4) Sequence Numbers Non-malignant tumors: assigned sequence numbers from the reportable-by-agreement series. Malignant tumors:
- 89. Histologic Transformation (5) Date of Diagnosis Non-malignant tumors: First date that a medical practitioner diagnosed the
- 90. Coding Sequence Numbers (1) Indicates the sequence of all reportable neoplasms over the lifetime of the
- 91. Coding Sequence Numbers (2) Reportable-by-agreement neoplasms are defined by each facility and/or central cancer registry: Non-malignant
- 92. Coding Sequence Numbers (3) Sequence numbers for non-malignant CNS tumors are assigned over the lifetime of
- 93. Assigning Diagnosis Date Rules for assigning diagnosis date are the same for malignant and non-malignant tumors.
- 94. Part IV Staging Risk Factors Genetic Syndromes Diagnostic Tools Treatment Edits Data Analysis
- 95. Collaborative Stage (CS) A computer algorithm uses the collaborative stage (CS) data fields to calculate site-specific
- 96. Coding Collaborative Stage (1) Separate sets of extension codes for: Brain and cerebral meninges Other parts
- 97. Coding Collaborative Stage (2) Site-specific codes for lymph nodes Same for the Brain, cerebral meninges and
- 98. CS Extension: Brain and Meninges C70.0, C71.0 – C71.9 (1) 05 Benign or borderline brain tumors
- 99. CS Extension: Brain and Meninges C70.0, C71.0 – C71.9 (2) 12 Infratentorial tumor confined to BRAIN
- 100. CS Extension: Brain and Meninges C70.0, C71.0 – C71.9 (3) 40 Tumor crosses the midline: involves
- 101. CS Extension: Brain and Meninges C70.0, C71.0 – C71.9 (4) 70 Circulating cells in cerebral spinal
- 102. CS Extension: Other CNS C70.1-9, C72.0–C72.9 (1) Spinal meninges, meninges NOS Spinal cord Caudia equina Olfactory,
- 103. CS Extension: Other CNS C70.1-9, C72.0–C72.9 (2) 05 Benign or borderline tumors 10 Tumor confined to
- 104. CS Extension: Other CNS C70.1-9, C72.0–C72.9 (3) 70 Brain except for cranial nerve tumors; bone, other
- 105. CS Extension: Other Endocrine C75.1, C75.2, C75.3 00 In situ; non-invasive; intraepithelial 05 Benign or borderline
- 106. CS Lymph Nodes Describes tumor involvement of regional lymph nodes. Code for CS Lymph Nodes is
- 107. CS Metastasis at Diagnosis Brain and Meninges C70.0, C71.0-9 00 No; None 10 Distant metastases 85
- 108. CS Metastasis at Diagnosis Other CNS and Other Endocrine C70.1-9, C72.0—9, C75.1, C75,2, C75.3 00 No;
- 109. CS Site-specific Factor 1 (1) C70.0-C70.9, C71.0-C71.9, C72.0-C72.9 010 WHO Grade I 020 WHO Grade II
- 110. CS Site-specific Factor 1 (2) C70.0-C70.9, C71.0-C71.9, C72.0-C72.9 C75.1- C75.3 Code the WHO grade for CNS
- 111. Possible Risk Factors Genetic predispositions for the development of brain tumors have been identified. Population-based studies
- 112. Possible Risk Factors Epstein-Barr virus in the DNA of primary lymphoma suggests a viral etiology for
- 113. Genetic Syndromes Genetic syndromes associated with multiple CNS tumors are: Neurofibromatosis I (von Recklinghausen’s disease) Neurofibromatosis
- 114. Diagnostic Tools – Physical Exam Neurological examination Eye movements Vision Hearing Reflexes Balance and coordination Sense
- 115. Diagnostic Tools: Radiology Computerized tomography (CT) scan Magnetic resonance imaging (MRI) Positron emission tomography (PET) Single
- 116. Diagnostic Tools: Laboratory tests Audiometry Electroencephalogram (EEG) Endocrine evaluation Evoked potentials Lumbar puncture Myelogram Perimetry
- 117. Diagnostic Tools Needle biopsy Needle inserted through a burr hole and tissue extracted for tissue diagnosis.
- 118. College of American Pathologist (CAP) Protocols Site-specific checklists Required to be completed in the health record
- 119. Brain and Spinal Cord CAP Protocols (1) Macroscopic Specimen type Specimen size Tumor site Tumor size
- 120. Brain and Spinal Cord CAP Protocols Microscopic Histologic type Histologic grade Margins Additional studies* Additional pathologic
- 121. Treatment (1) Watchful waiting Surgery Radiation Chemotherapy Hormonal therapy Immunotherapy Hematologic Transplant and Endocrine procedures
- 122. Treatment (2) Inoperable or inaccessible tumors may be treated with primary radiation and other systemic therapy:
- 123. Surgical Procedure of Primary Site Brain: Site-specific surgery codes Meninges Brain Spinal cord, cranial nerves, other
- 124. Surgical Procedure of Primary Site C70-0-C70.9, C71.0-C71.9, C72.0-C72.9 (1) Code 10: Tumor destruction, NOS Laser surgery
- 125. Surgical Procedure of Primary Site C70-0-C70.9, C71.0-C71.9, C72.0-C72.9 (2) 20:Local Excision (biopsy) of tumor, lesion, or
- 126. Surgical Procedure of Primary Site C75.1, C75.2, C75.3 (1) Code 10: Local tumor destruction, NOS Code
- 127. Surgical Procedure of Primary Site C75.1, C75.2, C75.3 (2) Code 20: Local tumor excision, NOS Code
- 128. Surgical Procedure of Primary Site C75.1, C75.2, C75.3 (3) Code 25: Laser excision Specimen sent to
- 129. Surgical Procedure of Primary Site C75.1, C75.2, C75.3 (4) Code 40: Total surgical removal of primary
- 130. Surgical Margins of the Primary Site Code final status of surgical margins COC-required data item. Serves
- 131. Scope of Regional Lymph Node Surgery Identifies removal, biopsy, or aspiration of regional lymph node(s): NPCR-,
- 132. Radiation Therapy (1) Radiation codes indicate type of radiation therapy performed as part of the first
- 133. Radiation Therapy (2) Beam radiation Codes 20 – 29: Conventional radiation therapy: from an external beam
- 134. Radiation Therapy (3) Beam radiation Code 32: Conformal radiation Code 40: Particle or proton beam Code
- 135. Radiation Therapy (3) Tumors typically treated with stereotactic radiosurgery include: Acoustic neuroma Chordoma Pineal tumor Astrocytoma
- 136. Radiation Therapy (4) Radioactive implants Code 50: Brachytherapy, radiation implants, radiation seeding, radioactive implants, interstitial implants,
- 137. Radiation Therapy (5) Radioactive implants (continued) Code 52: Intracavitary radiation with high dose rate applicator Code
- 138. Chemotherapy (1) Record type of chemotherapy administered as first course of treatment: Code 01: Chemotherapy, NOS
- 139. Chemotherapy (2) Blood-brain barrier Protects the brain from foreign substances, including chemotherapy. May be disrupted by
- 140. Chemotherapy (3) Interstitial chemotherapy Administered directly to involved tissues. Polymer wafers soaked in a chemotherapeutic agent
- 141. Hormone Therapy Record systemic hormonal agents administered as first course of treatment. Tamoxifen and RU-486 (Mifepristone)
- 142. Immunotherapy (1) Record whether immunotherapeutic agents were administered as first course of treatment: Angiogenesis inhibitors block
- 143. Immunotherapy (2) Gene therapy replaces or repairs the gene responsible for tumor growth. Vaccine therapy allows
- 144. Hematologic Transplant and Endocrine Procedures Identify systemic therapeutic procedures administered as first course of treatment: Code
- 145. Technical Issues Edit Checks NAACCR Edits Committee is developing and modifying data edits to accommodate data
- 146. Technical Issues Data Analysis Recommendations Report and analyze data for non-malignant CNS tumors separately from malignant
- 147. References Manuals, Articles, Reports A Primer of Brain Tumors, 1998; American Brain Tumor Association, Des Plaines,
- 148. References Manuals, Articles, Reports (continued) Fritz A, Percy C, Jack V, Shanmugaratnam K, Sobin V, Parkin
- 149. References Websites American Brain Tumor Association www.abta.org American College of Surgeons, Commission on Cancer Information, Facility
- 150. References Websites (continued) Brain and Neurosurgery Information Center www.brain-surgery.com/index.html Brain and Spinal Cord Tumors: Hope through
- 151. References Websites (continued) College of American Pathologists (CAP), Protocol – Brain ftp://ftp.cap.org/cancerprotocols/Brain03_p.doc Illustrated Glossary of Radiology:
- 152. References Websites (continued) International RadioSurgery Association www.isra.org/index.html National Brain Tumor Radiosurgery Association www.braintumors.com/radiosurgery/radiosrugery.info#TWO NCI Brain Tumor
- 153. References Websites (continued) PDQ Cancer Information Summaries: Adult Treatment www.cancer.gov/cancerinfo/pdq/adulttreatment PDQ Cancer Information Summaries: Pediatric Treatment
- 154. Acknowledgments (1) Prepared by Shannon Vann, CTR for the North American Association of Central Cancer Registries
- 155. Acknowledgments (2) Sponsors Centers for Disease Control and Prevention National Program for Cancer Registries National Cancer
- 156. Acknowledgments (3) CDC National Program of Cancer Registries Planning Committee Kimberly Cantrell Gayle G. Clutter Faye
- 158. Скачать презентацию
Portions of this presentation are based on non-malignant CNS tumor data
Portions of this presentation are based on non-malignant CNS tumor data
Part I
Rationale
History
Definition of Reportable Cases
Casefinding
Anticipated Impact on Registries
Part I
Rationale
History
Definition of Reportable Cases
Casefinding
Anticipated Impact on Registries
Rationale for Non-malignant CNS Tumor Surveillance and Registration
Non-malignant CNS tumors cause
Rationale for Non-malignant CNS Tumor Surveillance and Registration
Non-malignant CNS tumors cause
History 1992 -1996
1992 Central Brain Tumor Registry of the United States
History 1992 -1996
1992 Central Brain Tumor Registry of the United States
History 1998
BTWG forwarded four recommendations to the NCCCS
NCCCS
Accepted recommendations 1
History 1998
BTWG forwarded four recommendations to the NCCCS
NCCCS
Accepted recommendations 1
BTWG Recommendations (1)
The following standard definition is to be used for
BTWG Recommendations (1)
The following standard definition is to be used for
BTWG Recommendations (2)
Develop a standard site and histology definition for tabulating
BTWG Recommendations (2)
Develop a standard site and histology definition for tabulating
BTWG Recommendations (3)
Develop training for reporting and tabulating primary intracranial and
BTWG Recommendations (3)
Develop training for reporting and tabulating primary intracranial and
History 2000
International Classification of Diseases for Oncology 3rd Edition (ICD-O-3) and
History 2000
International Classification of Diseases for Oncology 3rd Edition (ICD-O-3) and
History 2001-2002
2001 NCCCS
Accepted Recommendations 1 and 2 as completed.
Reconvened the
History 2001-2002
2001 NCCCS
Accepted Recommendations 1 and 2 as completed.
Reconvened the
Reportable Brain-Related Tumors (1)
Public Law 107-260 requires reporting of brain-related tumors.
The
Reportable Brain-Related Tumors (1)
Public Law 107-260 requires reporting of brain-related tumors.
The
Reportable Brain-Related Tumors (2)
Brain
Cerebrum (C71.0)
Frontal lobe (C71.1)
Temporal lobe (C71.2)
Parietal lobe
Reportable Brain-Related Tumors (2)
Brain
Cerebrum (C71.0)
Frontal lobe (C71.1)
Temporal lobe (C71.2)
Parietal lobe
Reportable Brain-Related Tumors (3)
Brain (continued)
Ventricle (C71.5)
Cerebellum (C71.6)
Brain stem (C71.7)
Overlapping lesion of
Reportable Brain-Related Tumors (3)
Brain (continued)
Ventricle (C71.5)
Cerebellum (C71.6)
Brain stem (C71.7)
Overlapping lesion of
Reportable Brain-Related Tumors (4)
Meninges
Cerebral meninges (C70.0)
Spinal meninges (C70.1)
Meninges NOS (C70.9)
Spinal
Reportable Brain-Related Tumors (4)
Meninges
Cerebral meninges (C70.0)
Spinal meninges (C70.1)
Meninges NOS (C70.9)
Spinal
Reportable Brain-Related Tumors (5)
Cranial nerves
Olfactory nerve (C72.2)
Optic nerve (C72.3)
Acoustic nerve (C72.4)
Cranial
Reportable Brain-Related Tumors (5)
Cranial nerves
Olfactory nerve (C72.2)
Optic nerve (C72.3)
Acoustic nerve (C72.4)
Cranial
Reportable Brain-Related Tumors (6)
Other CNS (C72.8, C72.9)
Pituitary gland (C75.1)
Craniopharyngeal duct (C75.2)
Pineal
Reportable Brain-Related Tumors (6)
Other CNS (C72.8, C72.9)
Pituitary gland (C75.1)
Craniopharyngeal duct (C75.2)
Pineal
History 2003
2003 SEER-supported registries and COC-approved hospital cancer registries will also
History 2003
2003 SEER-supported registries and COC-approved hospital cancer registries will also
Impact of Collecting Data on Non-malignant CNS Tumors (1)
Annual increase in
Impact of Collecting Data on Non-malignant CNS Tumors (1)
Annual increase in
Impact of Collecting Data on Non-malignant CNS Tumors (2)
Central registry case
Impact of Collecting Data on Non-malignant CNS Tumors (2)
Central registry case
Impact of Collecting Data on Non-malignant CNS Tumors (3)
Central registries adding
Impact of Collecting Data on Non-malignant CNS Tumors (3)
Central registries adding
Impact of Collecting Data on Non-malignant CNS Tumors (4)
All cancer registries
Impact of Collecting Data on Non-malignant CNS Tumors (4)
All cancer registries
Case-finding (1)
Additional or expanded case-finding mechanisms:
Pathology
Radiology
Treatment facilities:
Radiation oncology centers and
Case-finding (1)
Additional or expanded case-finding mechanisms:
Pathology
Radiology
Treatment facilities:
Radiation oncology centers and
Case-finding (2)
Disease indices
Surgery logs
Diagnostic imaging
Radiation oncology
Neurology clinics
Medical oncology
Autopsy reports.
Case-finding (2)
Disease indices
Surgery logs
Diagnostic imaging
Radiation oncology
Neurology clinics
Medical oncology
Autopsy reports.
Case-finding Sources
Free-standing radiation therapy centers
Free-standing Magnetic Resonance Imaging (MRI) centers
Free-standing gamma
Case-finding Sources
Free-standing radiation therapy centers
Free-standing Magnetic Resonance Imaging (MRI) centers
Free-standing gamma
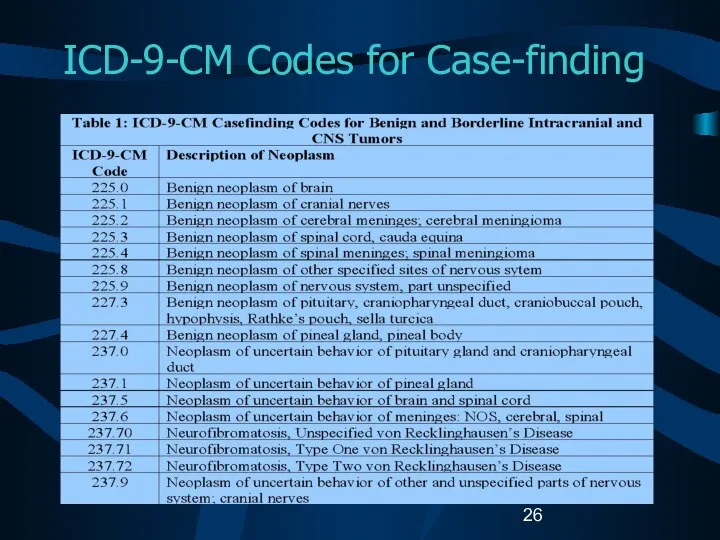
ICD-9-CM Codes for Case-finding
ICD-9-CM Codes for Case-finding
Unusual and Ambiguous Terminology
If the final pathologic diagnosis is a CNS
Unusual and Ambiguous Terminology
If the final pathologic diagnosis is a CNS
Part II
CNS Anatomy and Function
Histologies and Primary Sites
Grading Systems and Coding
Part II
CNS Anatomy and Function
Histologies and Primary Sites
Grading Systems and Coding
CNS Functional Anatomy
Source: URL: www.solinas.com/solinas/brain.html accessed 7/18/03.
CNS Functional Anatomy
Source: URL: www.solinas.com/solinas/brain.html accessed 7/18/03.
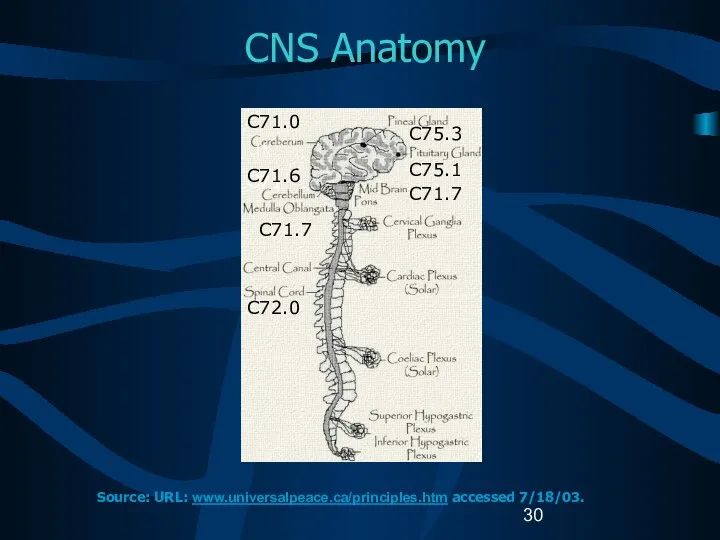
CNS Anatomy
C71
C71.6
C71.7
C72.0
C71.0
C75.3
C75.1
C71.7
Source: URL: www.universalpeace.ca/principles.htm accessed 7/18/03.
CNS Anatomy
C71
C71.6
C71.7
C72.0
C71.0
C75.3
C75.1
C71.7
Source: URL: www.universalpeace.ca/principles.htm accessed 7/18/03.
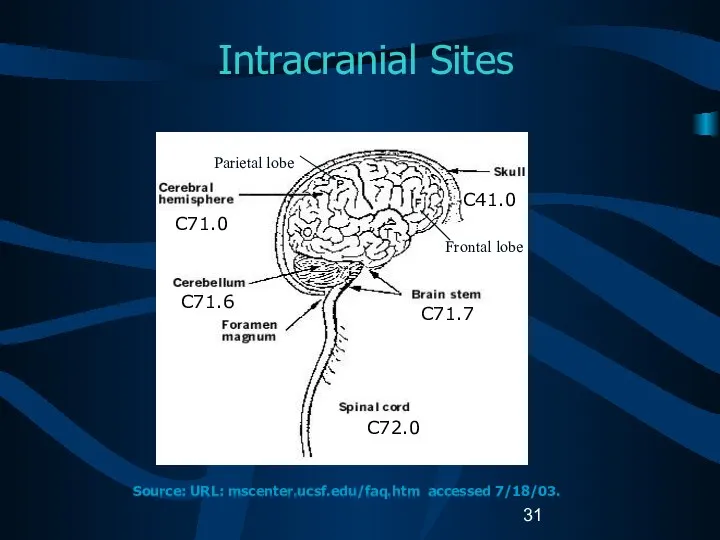
Intracranial Sites
C71.0
C71.6
C41.0
C71.7
C72.0
Source: URL: mscenter.ucsf.edu/faq.htm accessed 7/18/03.
Parietal lobe
Frontal lobe
Intracranial Sites
C71.0
C71.6
C41.0
C71.7
C72.0
Source: URL: mscenter.ucsf.edu/faq.htm accessed 7/18/03.
Parietal lobe
Frontal lobe
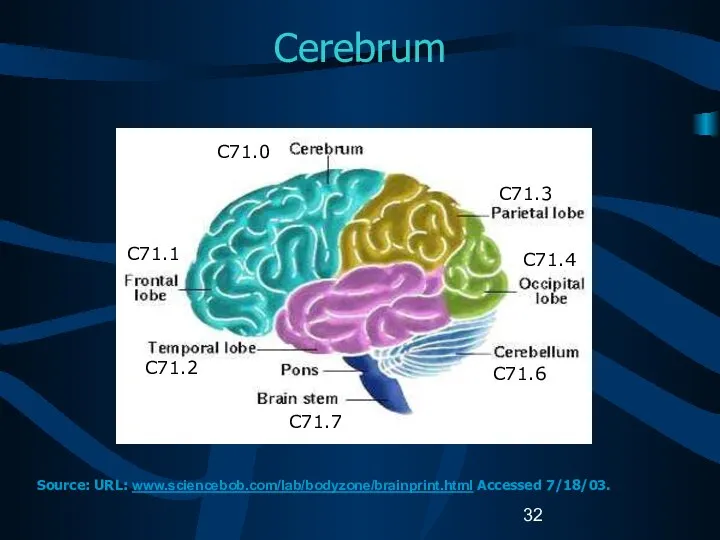
Cerebrum
C71.1
C71.2
C71.7
C71.3
C71.4
C71.6
C71.0
Source: URL: www.sciencebob.com/lab/bodyzone/brainprint.html Accessed 7/18/03.
Cerebrum
C71.1
C71.2
C71.7
C71.3
C71.4
C71.6
C71.0
Source: URL: www.sciencebob.com/lab/bodyzone/brainprint.html Accessed 7/18/03.
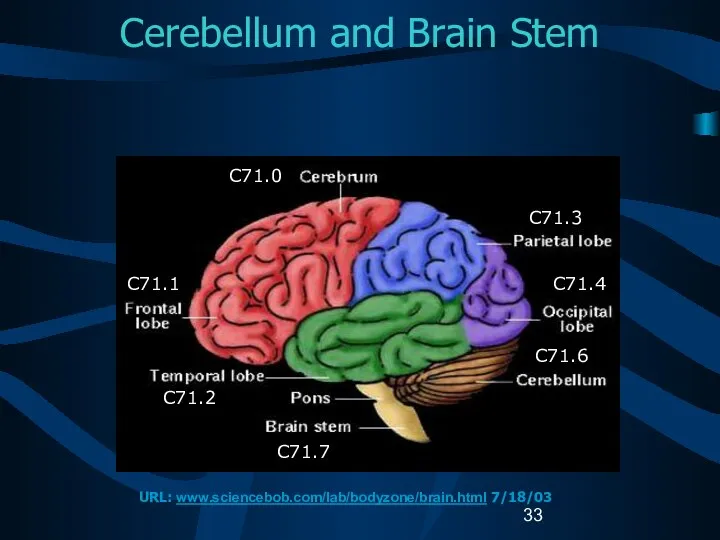
Cerebellum and Brain Stem
C71.0
C71.1
C71.2
C71.7
C71.3
C71.4
C71.6
URL: www.sciencebob.com/lab/bodyzone/brain.html 7/18/03
Cerebellum and Brain Stem
C71.0
C71.1
C71.2
C71.7
C71.3
C71.4
C71.6
URL: www.sciencebob.com/lab/bodyzone/brain.html 7/18/03
The Ventricular System
http://www.abta.org/primer2.htm
The Ventricular System
http://www.abta.org/primer2.htm
Pineal and Pituitary Glands
C75.1
C71.7
C75.3
C71.6
C72.0
Source: URL: training.seer.cancer.gov/module_anatomy/unit6_3_endo_gl… Accessed 7/18/03.
Pineal and Pituitary Glands
C75.1
C71.7
C75.3
C71.6
C72.0
Source: URL: training.seer.cancer.gov/module_anatomy/unit6_3_endo_gl… Accessed 7/18/03.
Cranial Nerves
I=C72.2, II=C72.3, VIII=C72.4, Others=C72.5
Source: URL: faculty.washington.edu/chudler/cranial.html Accessed 7/18/03.
Cranial Nerves
I=C72.2, II=C72.3, VIII=C72.4, Others=C72.5
Source: URL: faculty.washington.edu/chudler/cranial.html Accessed 7/18/03.
Meninges
C71.0
C70.0
C70.0
Source: URL: www.cardioliving.com/consumer/Stroke/Hemorrhagic_Stroke.sht Accessed 7/18/03.
Meninges
C71.0
C70.0
C70.0
Source: URL: www.cardioliving.com/consumer/Stroke/Hemorrhagic_Stroke.sht Accessed 7/18/03.
Tentorium
C70.0
C70.0
Source: URL: neurosurgery.mgh.harvard.edu/abta/primer.htm Accessed 7/18/03.
Tentorium
C70.0
C70.0
Source: URL: neurosurgery.mgh.harvard.edu/abta/primer.htm Accessed 7/18/03.
Spinal Cord
C72.0
C70.1
Source: URL: www.merck.com/pubs/mmanual/figures/182fig1.htm Accessed 7/18/03
Spinal Cord
C72.0
C70.1
Source: URL: www.merck.com/pubs/mmanual/figures/182fig1.htm Accessed 7/18/03
Cellular Classification
Neuroepithelial tumors
Astrocytomas
Oligodendrogliomas
Ependymomas
Pineal parenchymal tumors
Other CNS tumors
Sellar tumors
Hematopoetic tumors
Germ
Cellular Classification
Neuroepithelial tumors
Astrocytomas
Oligodendrogliomas
Ependymomas
Pineal parenchymal tumors
Other CNS tumors
Sellar tumors
Hematopoetic tumors
Germ
Glial Tumors (1)
Glial tissue: supportive tissue of brain made up
Glial Tumors (1)
Glial tissue: supportive tissue of brain made up
Glial Tumors (2)
Astrocytic tumors
Noninfiltrating
Juvenile pilocytic (M9421)
Subependymal (M9383)
Infiltrating
Well-differentiated mildly
Glial Tumors (2)
Astrocytic tumors
Noninfiltrating
Juvenile pilocytic (M9421)
Subependymal (M9383)
Infiltrating
Well-differentiated mildly
Glial Tumors (3)
Ependymal tumors
Myxopapillary and well-differentiated ependymomas (M9394)
Anaplastic ependymomas (M9392)
Ependymoblastomas
Glial Tumors (3)
Ependymal tumors
Myxopapillary and well-differentiated ependymomas (M9394)
Anaplastic ependymomas (M9392)
Ependymoblastomas
Glial Tumors (4)
Mixed tumors
Mixed astrocytoma-ependymomas
Mixed astrocytoma-oligodendrogliomas
Mixed astrocytoma-ependymoma-oligodendrogliomas
Other gliomas
Ganglioneuromas
Glial Tumors (4)
Mixed tumors
Mixed astrocytoma-ependymomas
Mixed astrocytoma-oligodendrogliomas
Mixed astrocytoma-ependymoma-oligodendrogliomas
Other gliomas
Ganglioneuromas
Non-Glial Tumors (1)
Pineal region tumors
Parenchymal tumors
Pineocytomas (M9361)
Pineoblastomas (M9362)
Pineal astrocytomas (M9400)
Germ
Non-Glial Tumors (1)
Pineal region tumors
Parenchymal tumors
Pineocytomas (M9361)
Pineoblastomas (M9362)
Pineal astrocytomas (M9400)
Germ

Non-Glial Tumors (2)
Meningiomas
Meningioma: Benign (M953_)
Malignant meningiomas
Anaplastic meningioma
Hemangiopericytoma (M9150)
Papillary meningioma (M9538)
Choroid plexus
Non-Glial Tumors (2)
Meningiomas
Meningioma: Benign (M953_)
Malignant meningiomas
Anaplastic meningioma
Hemangiopericytoma (M9150)
Papillary meningioma (M9538)
Choroid plexus
Other CNS Tumors (1)
Craniopharyngiomas (M9350)
Rathke pouch tumors
Chordomas (M9370)
Schwannomas (M9560)
Acoustic schwannomas/neuromas
Other CNS Tumors (1)
Craniopharyngiomas (M9350)
Rathke pouch tumors
Chordomas (M9370)
Schwannomas (M9560)
Acoustic schwannomas/neuromas
Other CNS Tumors (2)
Embryonal tumors
Retinoblastomas (M9510)
Primitive neuroectodermal tumors (PNETs)
Meduloblastomas (M9470)
Neuroblastomas
Other CNS Tumors (2)
Embryonal tumors
Retinoblastomas (M9510)
Primitive neuroectodermal tumors (PNETs)
Meduloblastomas (M9470)
Neuroblastomas
Other CNS Tumors (3)
Lymphomas (M9590)
Arise from
Indigenous brain histiocytes (microglia)
Rare lymphocytes in
Other CNS Tumors (3)
Lymphomas (M9590)
Arise from
Indigenous brain histiocytes (microglia)
Rare lymphocytes in
Other CNS Tumors (4)
Cysts and tumor-like lesions
Reportable
Dermoid cysts (M9084)
Granular
Other CNS Tumors (4)
Cysts and tumor-like lesions
Reportable
Dermoid cysts (M9084)
Granular
Childhood versus Adult Tumors
CNS tumor histology and location are different in
Childhood versus Adult Tumors
CNS tumor histology and location are different in
Childhood Brain Tumors
Meduloblastomas are the most common CNS histology in children.
50%
Childhood Brain Tumors
Meduloblastomas are the most common CNS histology in children.
50%
Cellular Classification
Childhood Brain Tumors (1)
Supratentorial tumors in children
Craniopharyngiomas
Germ cell tumors
Diencephalic
Cellular Classification
Childhood Brain Tumors (1)
Supratentorial tumors in children
Craniopharyngiomas
Germ cell tumors
Diencephalic
Cellular Classification
Childhood Brain Tumors (2)
The histopathology of childhood spinal tumors
Cellular Classification
Childhood Brain Tumors (2)
The histopathology of childhood spinal tumors
Cellular Classification
Childhood CNS Tumors
Cause of childhood CNS tumors remains unknown.
American
Cellular Classification
Childhood CNS Tumors
Cause of childhood CNS tumors remains unknown.
American
ICD-O-3 Coding Issues (1)
Some histologies may be difficult to determine if
ICD-O-3 Coding Issues (1)
Some histologies may be difficult to determine if
ICD-O-3 Coding Issues (2)
Continue to assign histology code M9421/3 to pilocytic
ICD-O-3 Coding Issues (2)
Continue to assign histology code M9421/3 to pilocytic
Grade for CNS Tumors
Sixth digit of ICD-O-3 histology code
Describes tumor
Grade for CNS Tumors
Sixth digit of ICD-O-3 histology code
Describes tumor
WHO Grade (1)
WHO grade coded in Collaborative Stage data field:
Site-specific
WHO Grade (1)
WHO grade coded in Collaborative Stage data field:
Site-specific
WHO Grade (2)
Grade II
Relatively slow growing
Sometimes recur as higher grade
WHO Grade (2)
Grade II
Relatively slow growing
Sometimes recur as higher grade
Kernohan Grade
Defines progressive malignancy for astrocytoma
Grade 1: benign astrocytomas
Grade 2: low-grade
Kernohan Grade
Defines progressive malignancy for astrocytoma
Grade 1: benign astrocytomas
Grade 2: low-grade
St. Anne-Mayo Grade (1)
Used for astrocytomas.
Uses four morphologic criteria:
Nuclear atypia
Mitosis
Endothelial
St. Anne-Mayo Grade (1)
Used for astrocytomas.
Uses four morphologic criteria:
Nuclear atypia
Mitosis
Endothelial
St. Anne-Mayo Grade (2)
Grade 1: No criteria
Grade 2: One criterion, usually
St. Anne-Mayo Grade (2)
Grade 1: No criteria
Grade 2: One criterion, usually
Grade for CNS Tumors
Do not record WHO grade, Kernohan grade, or
Grade for CNS Tumors
Do not record WHO grade, Kernohan grade, or
Part III
Laterality
Multiple Primaries
Malignant Transformation
Sequence Numbers
Date of Diagnosis
Part III
Laterality
Multiple Primaries
Malignant Transformation
Sequence Numbers
Date of Diagnosis
Determining Multiple Primaries:
Laterality
Brain is not a paired organ.
Laterality collected on
Determining Multiple Primaries:
Laterality
Brain is not a paired organ.
Laterality collected on
Coding Laterality (1)
CNS sites to be coded with laterality:
Cerebral meninges, NOS
Coding Laterality (1)
CNS sites to be coded with laterality:
Cerebral meninges, NOS
Coding Laterality (2)
CNS sites to be coded with laterality (continued):
Olfactory nerve
Coding Laterality (2)
CNS sites to be coded with laterality (continued):
Olfactory nerve
Determining Multiple Primaries:
Definitions
Non-malignant tumor
Tumor with ICD-O-3 behavior code
0 (benign) or
Determining Multiple Primaries:
Definitions
Non-malignant tumor
Tumor with ICD-O-3 behavior code
0 (benign) or
Determining Multiple Primaries
Malignant (1)
NO CHANGES (at this time)
Site
Rule: Each category
Determining Multiple Primaries
Malignant (1)
NO CHANGES (at this time)
Site
Rule: Each category
Determining Multiple Primaries:
Malignant (2)
Histology
Rule: Differences in histologic type refer
Determining Multiple Primaries:
Malignant (2)
Histology
Rule: Differences in histologic type refer
Determining Multiple Primaries
Non-malignant (1)
NEW RULES
Site
Rule: Each sub-site (fourth-digit level) as
Determining Multiple Primaries
Non-malignant (1)
NEW RULES
Site
Rule: Each sub-site (fourth-digit level) as
Determining Multiple Primaries
Non-malignant (2)
Site (cont)
EXCEPT NOS (C_ _.9) with specific
Determining Multiple Primaries
Non-malignant (2)
Site (cont)
EXCEPT NOS (C_ _.9) with specific
Determining Multiple Primaries
Non-malignant (3)
Site (cont)
Laterality: For non-malignant cases only
If multiple
Determining Multiple Primaries
Non-malignant (3)
Site (cont)
Laterality: For non-malignant cases only
If multiple
Determining Multiple Primaries:
Non-malignant (4)
Histology
Determining Multiple Primaries:
Non-malignant (4)
Histology
Determining Multiple Primaries:
Non-malignant (5)
Histology
If multiple tumors are in the same
Determining Multiple Primaries:
Non-malignant (5)
Histology
If multiple tumors are in the same
Determining Multiple Primaries:
Non-malignant (6)
Histology (cont.)
B. If all histologies are listed
Determining Multiple Primaries:
Non-malignant (6)
Histology (cont.)
B. If all histologies are listed
Determining Multiple Primaries:
Non-malignant (7)
Histology (cont)
C: If the first three digits
Determining Multiple Primaries:
Non-malignant (7)
Histology (cont)
C: If the first three digits
Determining Multiple Primaries:
Non-malignant (8)
Histology (cont)
D: If the first three digits
Determining Multiple Primaries:
Non-malignant (8)
Histology (cont)
D: If the first three digits
Determining Multiple Primaries:
Timing (1)
Primary malignant CNS tumors
NO CHANGE
Malignant tumors of
Determining Multiple Primaries:
Timing (1)
Primary malignant CNS tumors
NO CHANGE
Malignant tumors of
Determining Multiple Primaries:
Timing (2)
Primary non-malignant CNS tumors
NEW
No timing rule
If a new
Determining Multiple Primaries:
Timing (2)
Primary non-malignant CNS tumors
NEW
No timing rule
If a new
General Rules for Determining Multiple Primaries of CNS Sites (1)
Multiple lesions:
General Rules for Determining Multiple Primaries of CNS Sites (1)
Multiple lesions:
General Rules for Determining Multiple Primaries of CNS Sites (2)
Multiple lesions:
General Rules for Determining Multiple Primaries of CNS Sites (2)
Multiple lesions:
General Rules for Determining Multiple Primaries of CNS Sites (3)
Multiple tumors:
General Rules for Determining Multiple Primaries of CNS Sites (3)
Multiple tumors:
Histologic Transformation (1)
Histologic transformation or progression to a higher grade:
Determined by
Histologic Transformation (1)
Histologic transformation or progression to a higher grade:
Determined by
Histologic Transformation (2)
If a malignant CNS tumor recurs (transforms) as a
Histologic Transformation (2)
If a malignant CNS tumor recurs (transforms) as a
Histologic Transformation (3)
Transformation of a non-malignant tumor to a malignant tumor
Histologic Transformation (3)
Transformation of a non-malignant tumor to a malignant tumor
Histologic Transformation (4)
Sequence Numbers
Non-malignant tumors: assigned sequence numbers from the reportable-by-agreement
Histologic Transformation (4)
Sequence Numbers
Non-malignant tumors: assigned sequence numbers from the reportable-by-agreement
Histologic Transformation (5)
Date of Diagnosis
Non-malignant tumors: First date that a medical
Histologic Transformation (5)
Date of Diagnosis
Non-malignant tumors: First date that a medical
Coding Sequence Numbers (1)
Indicates the sequence of all reportable neoplasms over
Coding Sequence Numbers (1)
Indicates the sequence of all reportable neoplasms over
Coding Sequence Numbers (2)
Reportable-by-agreement neoplasms are defined by each facility and/or
Coding Sequence Numbers (2)
Reportable-by-agreement neoplasms are defined by each facility and/or
Coding Sequence Numbers (3)
Sequence numbers for non-malignant CNS tumors are assigned
Coding Sequence Numbers (3)
Sequence numbers for non-malignant CNS tumors are assigned
Assigning Diagnosis Date
Rules for assigning diagnosis date are the same for
Assigning Diagnosis Date
Rules for assigning diagnosis date are the same for
Part IV
Staging
Risk Factors
Genetic Syndromes
Diagnostic Tools
Treatment
Edits
Data Analysis
Part IV
Staging
Risk Factors
Genetic Syndromes
Diagnostic Tools
Treatment
Edits
Data Analysis
Collaborative Stage (CS)
A computer algorithm uses the collaborative stage (CS) data
Collaborative Stage (CS)
A computer algorithm uses the collaborative stage (CS) data
Coding Collaborative Stage (1)
Separate sets of extension codes for:
Brain and cerebral
Coding Collaborative Stage (1)
Separate sets of extension codes for:
Brain and cerebral
Coding Collaborative Stage (2)
Site-specific codes for lymph nodes
Same for the
Coding Collaborative Stage (2)
Site-specific codes for lymph nodes
Same for the
CS Extension: Brain and Meninges
C70.0, C71.0 – C71.9 (1)
05 Benign or borderline
CS Extension: Brain and Meninges
C70.0, C71.0 – C71.9 (1)
05 Benign or borderline
CS Extension: Brain and Meninges
C70.0, C71.0 – C71.9 (2)
12 Infratentorial tumor
CS Extension: Brain and Meninges
C70.0, C71.0 – C71.9 (2)
12 Infratentorial tumor
CS Extension: Brain and Meninges
C70.0, C71.0 – C71.9 (3)
40 Tumor crosses the
CS Extension: Brain and Meninges
C70.0, C71.0 – C71.9 (3)
40 Tumor crosses the
CS Extension: Brain and Meninges
C70.0, C71.0 – C71.9 (4)
70 Circulating cells in
CS Extension: Brain and Meninges
C70.0, C71.0 – C71.9 (4)
70 Circulating cells in
CS Extension: Other CNS
C70.1-9, C72.0–C72.9 (1)
Spinal meninges, meninges NOS
Spinal cord
Caudia
CS Extension: Other CNS
C70.1-9, C72.0–C72.9 (1)
Spinal meninges, meninges NOS
Spinal cord
Caudia
CS Extension: Other CNS
C70.1-9, C72.0–C72.9 (2)
05 Benign or borderline tumors
10 Tumor confined to
CS Extension: Other CNS
C70.1-9, C72.0–C72.9 (2)
05 Benign or borderline tumors
10 Tumor confined to
CS Extension: Other CNS
C70.1-9, C72.0–C72.9 (3)
70 Brain except for cranial nerve
CS Extension: Other CNS
C70.1-9, C72.0–C72.9 (3)
70 Brain except for cranial nerve
CS Extension: Other Endocrine
C75.1, C75.2, C75.3
00 In situ; non-invasive; intraepithelial
05 Benign or
CS Extension: Other Endocrine
C75.1, C75.2, C75.3
00 In situ; non-invasive; intraepithelial
05 Benign or
CS Lymph Nodes
Describes tumor involvement of regional lymph nodes.
Code for CS
CS Lymph Nodes
Describes tumor involvement of regional lymph nodes.
Code for CS
CS Metastasis at Diagnosis
Brain and Meninges
C70.0, C71.0-9
00 No; None
10 Distant metastases
85 “Drop” metastases
99 Unknown;
CS Metastasis at Diagnosis
Brain and Meninges
C70.0, C71.0-9
00 No; None
10 Distant metastases
85 “Drop” metastases
99 Unknown;
CS Metastasis at Diagnosis
Other CNS and Other Endocrine C70.1-9, C72.0—9, C75.1,
CS Metastasis at Diagnosis Other CNS and Other Endocrine C70.1-9, C72.0—9, C75.1,
CS Site-specific Factor 1 (1)
C70.0-C70.9, C71.0-C71.9, C72.0-C72.9
010 WHO Grade I
020 WHO Grade
CS Site-specific Factor 1 (1)
C70.0-C70.9, C71.0-C71.9, C72.0-C72.9
010 WHO Grade I
020 WHO Grade
CS Site-specific Factor 1 (2)
C70.0-C70.9, C71.0-C71.9, C72.0-C72.9
C75.1- C75.3
Code the WHO grade
CS Site-specific Factor 1 (2)
C70.0-C70.9, C71.0-C71.9, C72.0-C72.9
C75.1- C75.3
Code the WHO grade
Possible Risk Factors
Genetic predispositions for the development of brain tumors have
Possible Risk Factors
Genetic predispositions for the development of brain tumors have
Possible Risk Factors
Epstein-Barr virus in the DNA of primary lymphoma suggests
Possible Risk Factors
Epstein-Barr virus in the DNA of primary lymphoma suggests
Genetic Syndromes
Genetic syndromes associated with multiple CNS tumors are:
Neurofibromatosis I (von
Genetic Syndromes
Genetic syndromes associated with multiple CNS tumors are:
Neurofibromatosis I (von
Diagnostic Tools – Physical Exam
Neurological examination
Eye movements
Vision
Hearing
Reflexes
Balance and coordination
Sense of
Diagnostic Tools – Physical Exam
Neurological examination
Eye movements
Vision
Hearing
Reflexes
Balance and coordination
Sense of
Diagnostic Tools: Radiology
Computerized tomography (CT) scan
Magnetic resonance imaging (MRI)
Positron emission
Diagnostic Tools: Radiology
Computerized tomography (CT) scan
Magnetic resonance imaging (MRI)
Positron emission
Diagnostic Tools: Laboratory tests
Audiometry
Electroencephalogram (EEG)
Endocrine evaluation
Evoked potentials
Lumbar puncture
Myelogram
Perimetry
Diagnostic Tools: Laboratory tests
Audiometry
Electroencephalogram (EEG)
Endocrine evaluation
Evoked potentials
Lumbar puncture
Myelogram
Perimetry
Diagnostic Tools
Needle biopsy
Needle inserted through a burr hole and tissue extracted
Diagnostic Tools
Needle biopsy
Needle inserted through a burr hole and tissue extracted
College of American Pathologist (CAP) Protocols
Site-specific checklists
Required to be completed in
College of American Pathologist (CAP) Protocols
Site-specific checklists
Required to be completed in
Brain and Spinal Cord
CAP Protocols (1)
Macroscopic
Specimen type
Specimen size
Tumor site
Tumor size
Brain and Spinal Cord
CAP Protocols (1)
Macroscopic
Specimen type
Specimen size
Tumor site
Tumor size
Brain and Spinal Cord
CAP Protocols
Microscopic
Histologic type
Histologic grade
Margins
Additional studies*
Additional pathologic findings*
Comments*
*Not required
Brain and Spinal Cord
CAP Protocols
Microscopic
Histologic type
Histologic grade
Margins
Additional studies*
Additional pathologic findings*
Comments*
*Not required
Treatment (1)
Watchful waiting
Surgery
Radiation
Chemotherapy
Hormonal therapy
Immunotherapy
Hematologic Transplant
and Endocrine procedures
Treatment (1)
Watchful waiting
Surgery
Radiation
Chemotherapy
Hormonal therapy
Immunotherapy
Hematologic Transplant
and Endocrine procedures
Treatment (2)
Inoperable or inaccessible tumors may be treated with primary radiation
Treatment (2)
Inoperable or inaccessible tumors may be treated with primary radiation
Surgical Procedure of Primary Site
Brain: Site-specific surgery codes
Meninges
Brain
Spinal cord, cranial nerves,
Surgical Procedure of Primary Site
Brain: Site-specific surgery codes
Meninges
Brain
Spinal cord, cranial nerves,
Surgical Procedure of Primary Site
C70-0-C70.9, C71.0-C71.9, C72.0-C72.9 (1)
Code 10: Tumor destruction,
Surgical Procedure of Primary Site
C70-0-C70.9, C71.0-C71.9, C72.0-C72.9 (1)
Code 10: Tumor destruction,
Surgical Procedure of Primary Site
C70-0-C70.9, C71.0-C71.9, C72.0-C72.9 (2)
20:Local Excision (biopsy) of
Surgical Procedure of Primary Site
C70-0-C70.9, C71.0-C71.9, C72.0-C72.9 (2)
20:Local Excision (biopsy) of
Surgical Procedure of Primary Site
C75.1, C75.2, C75.3 (1)
Code 10: Local tumor
Surgical Procedure of Primary Site
C75.1, C75.2, C75.3 (1)
Code 10: Local tumor
Surgical Procedure of Primary Site
C75.1, C75.2, C75.3 (2)
Code 20: Local tumor
Surgical Procedure of Primary Site
C75.1, C75.2, C75.3 (2)
Code 20: Local tumor
Surgical Procedure of Primary Site
C75.1, C75.2, C75.3 (3)
Code 25: Laser excision
Specimen
Surgical Procedure of Primary Site
C75.1, C75.2, C75.3 (3)
Code 25: Laser excision
Specimen
Surgical Procedure of Primary Site
C75.1, C75.2, C75.3 (4)
Code 40: Total surgical
Surgical Procedure of Primary Site
C75.1, C75.2, C75.3 (4)
Code 40: Total surgical
Surgical Margins of the Primary Site
Code final status of surgical margins
COC-required
Surgical Margins of the Primary Site
Code final status of surgical margins
COC-required
Scope of Regional Lymph Node Surgery
Identifies removal, biopsy, or aspiration of
Scope of Regional Lymph Node Surgery
Identifies removal, biopsy, or aspiration of
Radiation Therapy (1)
Radiation codes indicate type of radiation therapy performed
Radiation Therapy (1)
Radiation codes indicate type of radiation therapy performed
Radiation Therapy (2)
Beam radiation
Codes 20 – 29:
Conventional radiation therapy: from
Radiation Therapy (2)
Beam radiation
Codes 20 – 29:
Conventional radiation therapy: from
Radiation Therapy (3)
Beam radiation
Code 32: Conformal radiation
Code 40: Particle or
Radiation Therapy (3)
Beam radiation
Code 32: Conformal radiation
Code 40: Particle or
Radiation Therapy (3)
Tumors typically treated with stereotactic radiosurgery include:
Acoustic neuroma
Chordoma
Pineal
Radiation Therapy (3)
Tumors typically treated with stereotactic radiosurgery include:
Acoustic neuroma
Chordoma
Pineal
Radiation Therapy (4)
Radioactive implants
Code 50: Brachytherapy, radiation implants, radiation seeding, radioactive
Radiation Therapy (4)
Radioactive implants
Code 50: Brachytherapy, radiation implants, radiation seeding, radioactive
Radiation Therapy (5)
Radioactive implants (continued)
Code 52: Intracavitary radiation with high dose
Radiation Therapy (5)
Radioactive implants (continued)
Code 52: Intracavitary radiation with high dose
Chemotherapy (1)
Record type of chemotherapy administered as first course of treatment:
Code
Chemotherapy (1)
Record type of chemotherapy administered as first course of treatment:
Code
Chemotherapy (2)
Blood-brain barrier
Protects the brain from foreign substances, including chemotherapy.
May
Chemotherapy (2)
Blood-brain barrier
Protects the brain from foreign substances, including chemotherapy.
May
Chemotherapy (3)
Interstitial chemotherapy
Administered directly to involved tissues.
Polymer wafers soaked in a
Chemotherapy (3)
Interstitial chemotherapy
Administered directly to involved tissues.
Polymer wafers soaked in a
Hormone Therapy
Record systemic hormonal agents administered as first course of treatment.
Tamoxifen
Hormone Therapy
Record systemic hormonal agents administered as first course of treatment.
Tamoxifen
Immunotherapy (1)
Record whether immunotherapeutic agents were administered as first course of
Immunotherapy (1)
Record whether immunotherapeutic agents were administered as first course of
Immunotherapy (2)
Gene therapy replaces or repairs the gene responsible for tumor
Immunotherapy (2)
Gene therapy replaces or repairs the gene responsible for tumor
Hematologic Transplant and Endocrine Procedures
Identify systemic therapeutic procedures administered as first
Hematologic Transplant and Endocrine Procedures
Identify systemic therapeutic procedures administered as first
Technical Issues
Edit Checks
NAACCR Edits Committee is developing and modifying data edits
Technical Issues
Edit Checks
NAACCR Edits Committee is developing and modifying data edits
Technical Issues
Data Analysis Recommendations
Report and analyze data for non-malignant CNS tumors
Technical Issues
Data Analysis Recommendations
Report and analyze data for non-malignant CNS tumors
References
Manuals, Articles, Reports
A Primer of Brain Tumors, 1998; American Brain Tumor
References
Manuals, Articles, Reports
A Primer of Brain Tumors, 1998; American Brain Tumor
References
Manuals, Articles, Reports (continued)
Fritz A, Percy C, Jack V, Shanmugaratnam K,
References
Manuals, Articles, Reports (continued)
Fritz A, Percy C, Jack V, Shanmugaratnam K,
References
Websites
American Brain Tumor Association www.abta.org
American College of Surgeons, Commission on Cancer
References
Websites
American Brain Tumor Association www.abta.org
American College of Surgeons, Commission on Cancer
References
Websites (continued)
Brain and Neurosurgery Information Center www.brain-surgery.com/index.html
Brain and Spinal Cord Tumors:
References
Websites (continued)
Brain and Neurosurgery Information Center www.brain-surgery.com/index.html
Brain and Spinal Cord Tumors:
References
Websites (continued)
College of American Pathologists (CAP), Protocol – Brain ftp://ftp.cap.org/cancerprotocols/Brain03_p.doc
Illustrated Glossary
References
Websites (continued)
College of American Pathologists (CAP), Protocol – Brain ftp://ftp.cap.org/cancerprotocols/Brain03_p.doc
Illustrated Glossary
References
Websites (continued)
International RadioSurgery Association www.isra.org/index.html
National Brain Tumor Radiosurgery Association www.braintumors.com/radiosurgery/radiosrugery.info#TWO
NCI Brain
References
Websites (continued)
International RadioSurgery Association www.isra.org/index.html
National Brain Tumor Radiosurgery Association www.braintumors.com/radiosurgery/radiosrugery.info#TWO
NCI Brain
References
Websites (continued)
PDQ Cancer Information Summaries: Adult Treatment www.cancer.gov/cancerinfo/pdq/adulttreatment
PDQ Cancer Information Summaries:
References
Websites (continued)
PDQ Cancer Information Summaries: Adult Treatment www.cancer.gov/cancerinfo/pdq/adulttreatment
PDQ Cancer Information Summaries:
Acknowledgments (1)
Prepared by
Shannon Vann, CTR
for the
North American Association of Central Cancer
Acknowledgments (1)
Prepared by
Shannon Vann, CTR
for the
North American Association of Central Cancer
Acknowledgments (2)
Sponsors
Centers for Disease Control and Prevention
National Program for Cancer Registries
National
Acknowledgments (2)
Sponsors
Centers for Disease Control and Prevention
National Program for Cancer Registries
National
Acknowledgments (3)
CDC National Program of Cancer Registries Planning Committee
Kimberly Cantrell
Gayle G.
Acknowledgments (3)
CDC National Program of Cancer Registries Planning Committee
Kimberly Cantrell
Gayle G.
 Многозональные вытяжные вентиляторы
Многозональные вытяжные вентиляторы 11 класс
11 класс  Формы государства. Политика
Формы государства. Политика Богослужения суббот Великого поста
Богослужения суббот Великого поста Аполлон и Дафна
Аполлон и Дафна Культура и информатизация
Культура и информатизация  Бетон
Бетон Декоративно – прикладное искусство в жизни человека. Лоскутное шитье. (5 класс) Учитель – технологии Лисичкина Зинаида Алекс
Декоративно – прикладное искусство в жизни человека. Лоскутное шитье. (5 класс) Учитель – технологии Лисичкина Зинаида Алекс Деловая культура Кореи
Деловая культура Кореи (з†бвм-ѓа®ЂЃ¶•≠®•)-КРУГИ ЭЙЛЕРА
(з†бвм-ѓа®ЂЃ¶•≠®•)-КРУГИ ЭЙЛЕРА Презентация на тему "Семинар Методы и формы организации контроля усвоения учащимися учебного материала" - скачать презентаци
Презентация на тему "Семинар Методы и формы организации контроля усвоения учащимися учебного материала" - скачать презентаци лек9структур05прогр
лек9структур05прогр  Международные отношения на современном этапе
Международные отношения на современном этапе Зона комфорта
Зона комфорта  Виктор Михайлович Васнецов
Виктор Михайлович Васнецов Формирование современной городской среды. Город Глазов 2018-2022 годы. Общественная территория «Сквер у музыкальной школы»
Формирование современной городской среды. Город Глазов 2018-2022 годы. Общественная территория «Сквер у музыкальной школы» Теория культур Эдварда Холла
Теория культур Эдварда Холла Parallel programming technologies on hybrid architectures
Parallel programming technologies on hybrid architectures Марченко Мария, 8 «В»
Марченко Мария, 8 «В»  Презентация на тему "Технология проблемного обучения. Метапредметный подход" - скачать презентации по Педагогике
Презентация на тему "Технология проблемного обучения. Метапредметный подход" - скачать презентации по Педагогике Психические познавательные процессы
Психические познавательные процессы Жостовская роспись
Жостовская роспись О маркетинге. О книгах. О принципах. Игорь Манн
О маркетинге. О книгах. О принципах. Игорь Манн Теория и практика решения кейсов по корпоративному праву
Теория и практика решения кейсов по корпоративному праву Политическое сознание
Политическое сознание Государственные и заказы на муниципальном уровне
Государственные и заказы на муниципальном уровне Первый день творения
Первый день творения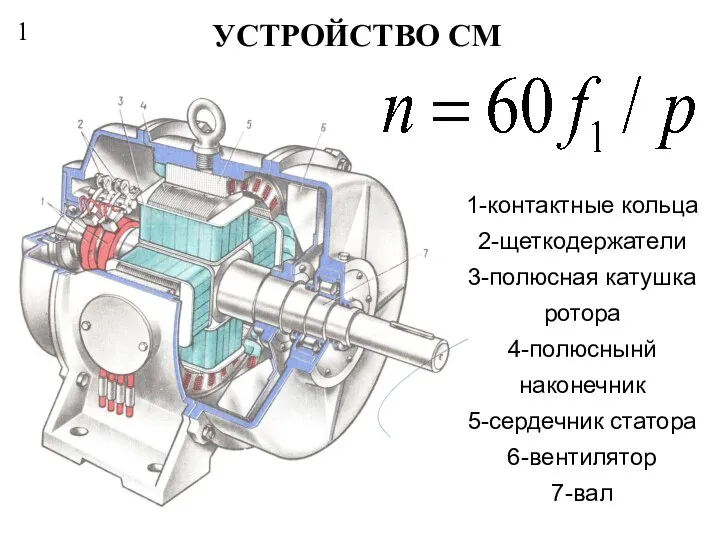 Устройство СМ
Устройство СМ