- Acute and glomerulonephritis. Nephrotic syndrome

Содержание
- 2. The concept of glomerulonephritis. Classification. Etiology. Diagnostics Analyzes Сontent
- 3. Acute glomerulonephritis is an acute diffuse immune-mediated inflammation that has developed after sensitization with an antigen
- 4. Acute glomerulonephritis
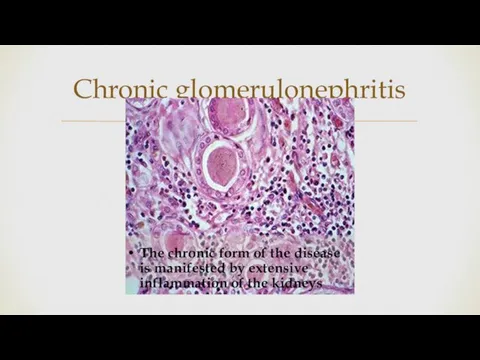
- 5. Chronic glomerulonephritis
- 6. Acute (10%): - with acute arthritis syndrome - with isolated urinary syndrome - with nephrotic syndrome
- 7. Glomerulonephritis develops from infections, poisonings, allergies, because of the complications of other diseases. getting into the
- 8. The acute form progresses rather quickly, after a couple of weeks the following symptoms are observed:
- 9. nephrotic (small admixtures of blood in the urine, problems with urination, in the analysis of blood
- 10. It happens quite difficult because of the absence of obvious symptoms (latent leakage), in contrast to
- 11. ANALYSIS
- 12. During the exacerbation of the nephrotic form of CG, an early manifestation is a decrease in
- 13. OAK leukocytosis, eosinophilia, elevated ESR, often thrombocytopenia BH blood - the total protein content is reduced.
- 14. Nephrotic range proteinuria, (>40mg/m2/hour), (> 50mg/kg/day), urine to protein creat ratio (>2mg/mg), +3-4 on dipstick Hypoalbumenia
- 15. Primary or idiopathic(MCD,FSGS,Membranous, Mesangial proliferation) 2. Secondary to infections,systemic diseases (HSP,SLE) ETIOLOGY
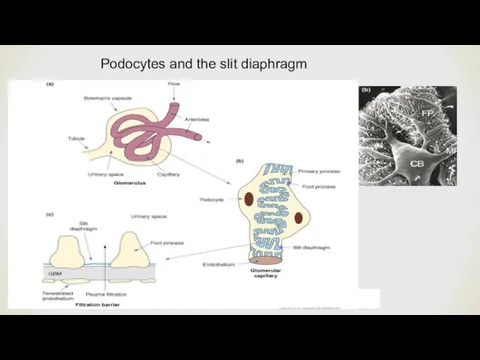
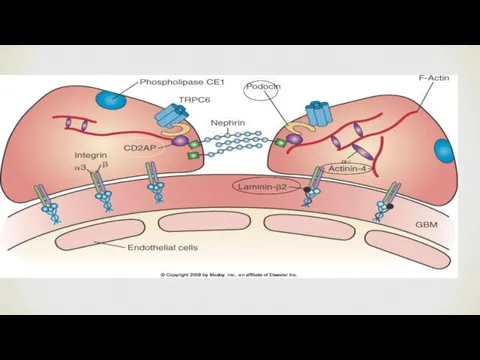
- 16. Podocytes and the slit diaphragm
- 20. Electrolytes: low Na,low albumin and calcium ANA,C3,C4,hepatitis B,C Hemoglobin high,platlet high Urine Na less than 10
- 21. First episode :Steriods 2mg/kg/day,60 mg/m2/day single daily dose for 4 weeks,followed by alternate dose for 3-6
- 22. Treatment of relapses:2mg/kg/day till remission for 3 days,then alternate days for 2-3m. Treatment of FR or
- 23. 1-Infections:losses of IgG in urine,abn T cell function,low factor B (C3 proactivator),steriod use,impaired opsonization Encapsulated bact
- 25. Скачать презентацию

The concept of glomerulonephritis.
Classification.
Etiology.
Diagnostics
Analyzes
Сontent
The concept of glomerulonephritis.
Classification.
Etiology.
Diagnostics
Analyzes
Сontent
Acute glomerulonephritis is an acute diffuse immune-mediated inflammation that has developed
Acute glomerulonephritis is an acute diffuse immune-mediated inflammation that has developed
Acute glomerulonephritis
Acute glomerulonephritis
Chronic glomerulonephritis
Chronic glomerulonephritis
Acute (10%): - with acute arthritis syndrome
- with isolated urinary
- with isolated urinary
Glomerulonephritis develops from infections, poisonings, allergies, because of the complications of
Glomerulonephritis develops from infections, poisonings, allergies, because of the complications of
The acute form progresses rather quickly, after a couple of weeks
The acute form progresses rather quickly, after a couple of weeks
nephrotic (small admixtures of blood in the urine, problems with urination,
nephrotic (small admixtures of blood in the urine, problems with urination,
It happens quite difficult because of the absence of obvious symptoms
It happens quite difficult because of the absence of obvious symptoms

ANALYSIS
ANALYSIS

During the exacerbation of the nephrotic form of CG, an early
During the exacerbation of the nephrotic form of CG, an early
OAK leukocytosis, eosinophilia, elevated ESR, often thrombocytopenia
BH blood - the total
OAK leukocytosis, eosinophilia, elevated ESR, often thrombocytopenia BH blood - the total
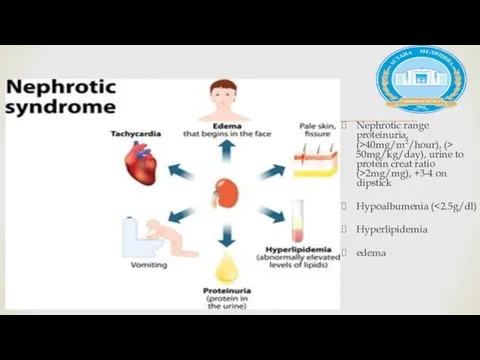
Nephrotic range proteinuria, (>40mg/m2/hour), (> 50mg/kg/day), urine to protein creat ratio
Nephrotic range proteinuria, (>40mg/m2/hour), (> 50mg/kg/day), urine to protein creat ratio
Primary or idiopathic(MCD,FSGS,Membranous,
Mesangial proliferation)
2. Secondary to infections,systemic diseases (HSP,SLE)
ETIOLOGY
Primary or idiopathic(MCD,FSGS,Membranous,
Mesangial proliferation)
2. Secondary to infections,systemic diseases (HSP,SLE)
ETIOLOGY
Podocytes and the slit diaphragm
Podocytes and the slit diaphragm

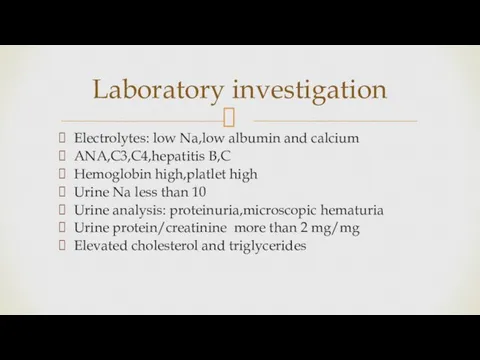
Electrolytes: low Na,low albumin and calcium
ANA,C3,C4,hepatitis B,C
Hemoglobin high,platlet high
Urine Na less
Electrolytes: low Na,low albumin and calcium
ANA,C3,C4,hepatitis B,C
Hemoglobin high,platlet high
Urine Na less
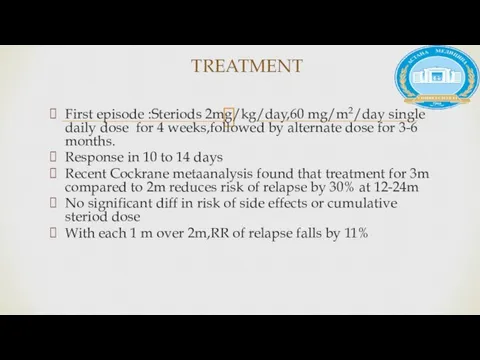
First episode :Steriods 2mg/kg/day,60 mg/m2/day single daily dose for 4 weeks,followed
First episode :Steriods 2mg/kg/day,60 mg/m2/day single daily dose for 4 weeks,followed
Treatment of relapses:2mg/kg/day till remission for 3 days,then alternate days for
Treatment of relapses:2mg/kg/day till remission for 3 days,then alternate days for

1-Infections:losses of IgG in urine,abn T cell function,low factor B (C3
1-Infections:losses of IgG in urine,abn T cell function,low factor B (C3
 Вариативная анатомия сосудов головы и шеи
Вариативная анатомия сосудов головы и шеи Травлення в ротовій порожнині
Травлення в ротовій порожнині Диабетическая нейропатия
Диабетическая нейропатия Конфліктні ситуації та способи запобігання конфліктів
Конфліктні ситуації та способи запобігання конфліктів Особенности репрезентации боевой стрессовой реакции у курсантов военных учебных заведений
Особенности репрезентации боевой стрессовой реакции у курсантов военных учебных заведений Проблемное поведение: как реагировать, что делать?
Проблемное поведение: как реагировать, что делать? Опухоли пищевода
Опухоли пищевода Төменгі температура көмегімен консервілеу
Төменгі температура көмегімен консервілеу Техника забора анализов, правила хранения и транспортировки
Техника забора анализов, правила хранения и транспортировки Основы противоопухолевой химиотерапии
Основы противоопухолевой химиотерапии Врожденная кишечная непроходимость
Врожденная кишечная непроходимость Шет Елдердегі стандартты емдеу комплаенсы
Шет Елдердегі стандартты емдеу комплаенсы Тренинг. Домашнее задание
Тренинг. Домашнее задание Абьюзивные отношения
Абьюзивные отношения Тұрғындарда наркомания мен токсикоманияның қауіп-қатер топтарының арасында алдын алуды жүргізу
Тұрғындарда наркомания мен токсикоманияның қауіп-қатер топтарының арасында алдын алуды жүргізу Анестезия и интенсивная терапия в травматологии и ортопедии
Анестезия и интенсивная терапия в травматологии и ортопедии Газовая гангрена
Газовая гангрена Что такое ремоделирование и как этот процесс влияет на приживление имплантов
Что такое ремоделирование и как этот процесс влияет на приживление имплантов Методы искусственного прерывания беременности в ранние и поздние сроки. Безопасный аборт
Методы искусственного прерывания беременности в ранние и поздние сроки. Безопасный аборт Рубец на матке. Перспективы самостоятельных родов
Рубец на матке. Перспективы самостоятельных родов Сердечно-легочная реанимация с автоматической наружной дефибрилляцией
Сердечно-легочная реанимация с автоматической наружной дефибрилляцией Направление и основные ветви лучевого нерва
Направление и основные ветви лучевого нерва Развитие психики в филогенезе. Инстинктивные и индивидуально приобретаемые формы поведения
Развитие психики в филогенезе. Инстинктивные и индивидуально приобретаемые формы поведения Трофобластическая болезнь
Трофобластическая болезнь Патогенные микроорганизмы, пищевые инфекции и отравления, и их профилактика
Патогенные микроорганизмы, пищевые инфекции и отравления, и их профилактика Жасанды мүше туралы жалпы түсінік
Жасанды мүше туралы жалпы түсінік АНЕМИИ
АНЕМИИ Қарым-қатынас әдістері
Қарым-қатынас әдістері