- Aortic Stenosis

Содержание
- 2. Aortic Stenosis Etiology Physical Examination Assessing Severity Natural History Prognosis Timing of Surgery
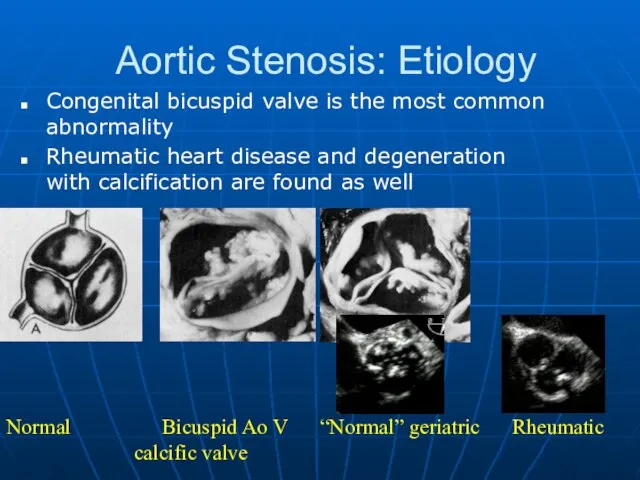
- 3. Aortic Stenosis: Etiology Congenital bicuspid valve is the most common abnormality Rheumatic heart disease and degeneration
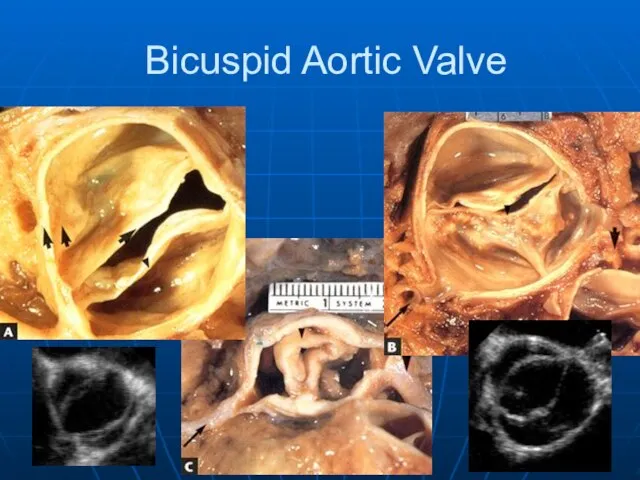
- 4. Bicuspid Aortic Valve
- 5. Aortic Stenosis - Etiology Young or middle-aged patient (4 & 5th decades) think congenital or rheumatic
- 6. Aortic Stenosis: Symptoms Cardinal Symptoms Chest pain (angina) Reduced coronary flow reserve Increased demand-high afterload Syncope/Dizziness
- 7. Aortic Stenosis: Physical Findings Intensity DOES NOT predict severity Presence of thrill DOES NOT predict severity
- 8. Aortic Stenosis: Physical Findings S1 S2 S1 S2 Mild-Moderate Severe
- 9. Severity of Stenosis Normal aortic valve area 2.5-3.5 cm2 Mild stenosis 1.5-2.5 cm2 Moderate stenosis 1.0-1.5
- 10. Diagnosis: Echocardiogram Etiology Valve gradient and area LVH Systolic LV function Diastolic LV function LA size
- 11. Echocardiogram
- 12. Doppler estimation of AVA
- 13. Cardiac catheteriztion Gorlin Method Simplified: Hakke’s formula AVA=CO/√(p-p gradient)
- 14. Low gradient AS Calculated AVA is AV gradient is Stenotic or not Stenotic?
- 15. Low gradient AS
- 16. Aortic Stenosis: Prognosis Therapy: Valve replacement for severe aortic stenosis Operative mortality (elderly) ~ 4%/Morbidity ~
- 17. Natural History of Aortic Stenosis Heart failure reduces life expectancy to less than 2 years Angina
- 19. Operative mortality of AVR in the elderly ~ 4-24%/year Risk factors for operative mortality Functional class
- 20. AVR is recommended in symptomatic patients with severe AS (stage D1) with : Decreased systolic opening
- 21. PARTNER Study Design N = 358 Inoperable Standard Therapy n = 179 ASSESSMENT: Transfemoral Access TF
- 22. All-Cause Mortality Landmark Analysis
- 24. Prosthetic Heart Valves
- 25. Caged-Ball Valve
- 26. Disc Valve
- 27. Bio-prosthetic Valve
- 28. Prosthetic Valves MECHANICAL Durable Large orifice High thromboembolic potential Best in Left Side Chronic warfarin therapy
- 30. Скачать презентацию
Aortic Stenosis
Etiology
Physical Examination
Assessing Severity
Natural History
Prognosis
Timing of Surgery
Aortic Stenosis
Etiology
Physical Examination
Assessing Severity
Natural History
Prognosis
Timing of Surgery
Aortic Stenosis: Etiology
Congenital bicuspid valve is the most common abnormality
Rheumatic heart
Aortic Stenosis: Etiology
Congenital bicuspid valve is the most common abnormality
Rheumatic heart
Bicuspid Aortic Valve
Bicuspid Aortic Valve
Aortic Stenosis - Etiology
Young or middle-aged patient (4 & 5th decades)
Aortic Stenosis - Etiology
Young or middle-aged patient (4 & 5th decades)
Aortic Stenosis: Symptoms
Cardinal Symptoms
Chest pain (angina)
Reduced coronary flow reserve
Increased demand-high afterload
Syncope/Dizziness
Aortic Stenosis: Symptoms
Cardinal Symptoms
Chest pain (angina)
Reduced coronary flow reserve
Increased demand-high afterload
Syncope/Dizziness
Aortic Stenosis: Physical Findings
Intensity DOES NOT predict severity
Presence of thrill DOES
Aortic Stenosis: Physical Findings
Intensity DOES NOT predict severity
Presence of thrill DOES
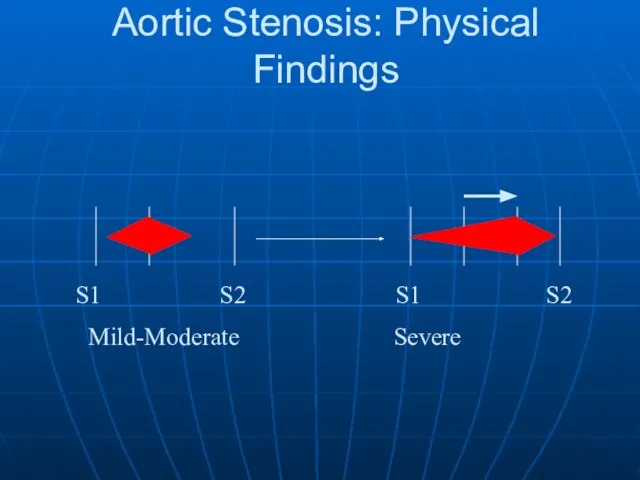
Aortic Stenosis: Physical Findings
S1 S2 S1 S2
Mild-Moderate Severe
Aortic Stenosis: Physical Findings
S1 S2 S1 S2
Mild-Moderate Severe
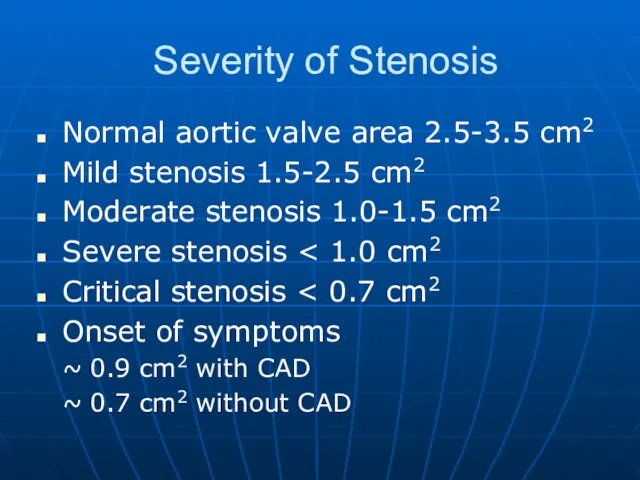
Severity of Stenosis
Normal aortic valve area 2.5-3.5 cm2
Mild stenosis 1.5-2.5 cm2
Moderate
Severity of Stenosis
Normal aortic valve area 2.5-3.5 cm2
Mild stenosis 1.5-2.5 cm2
Moderate
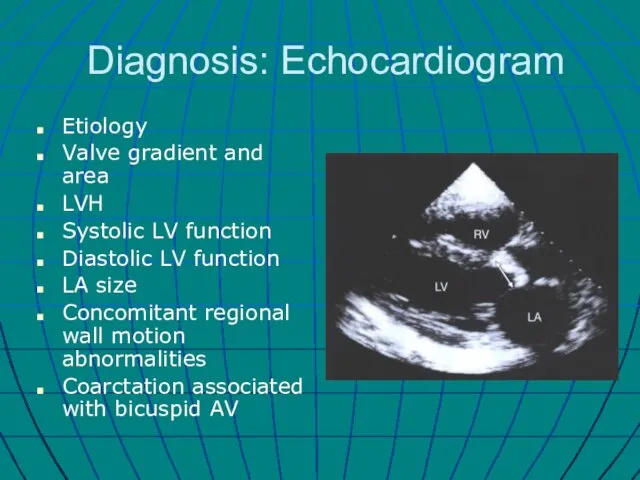
Diagnosis: Echocardiogram
Etiology
Valve gradient and area
LVH
Systolic LV function
Diastolic LV function
LA size
Concomitant regional
Diagnosis: Echocardiogram
Etiology
Valve gradient and area
LVH
Systolic LV function
Diastolic LV function
LA size
Concomitant regional

Echocardiogram
Echocardiogram
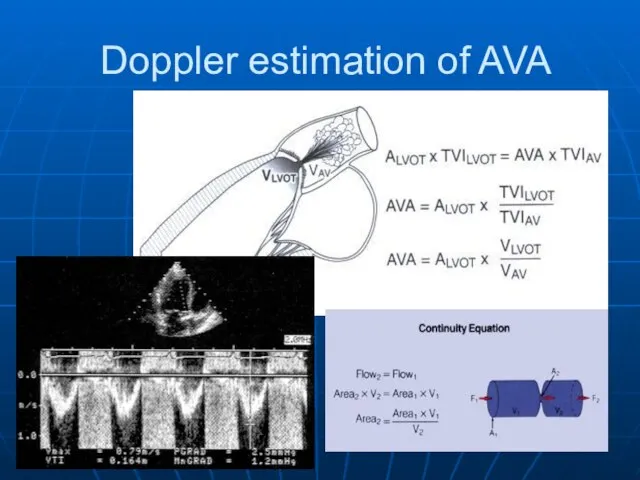
Doppler estimation of AVA
Doppler estimation of AVA
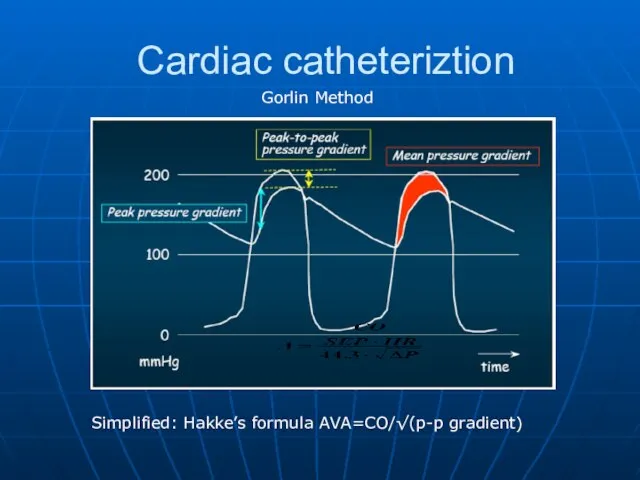
Cardiac catheteriztion
Gorlin Method
Simplified: Hakke’s formula AVA=CO/√(p-p gradient)
Cardiac catheteriztion
Gorlin Method
Simplified: Hakke’s formula AVA=CO/√(p-p gradient)
Low gradient AS
Calculated AVA is < 1.0 cm2 , But…
AV gradient
Low gradient AS
Calculated AVA is < 1.0 cm2 , But…
AV gradient
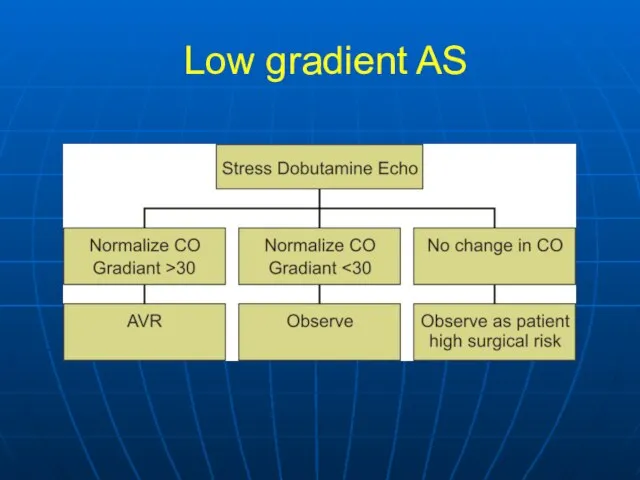
Low gradient AS
Low gradient AS
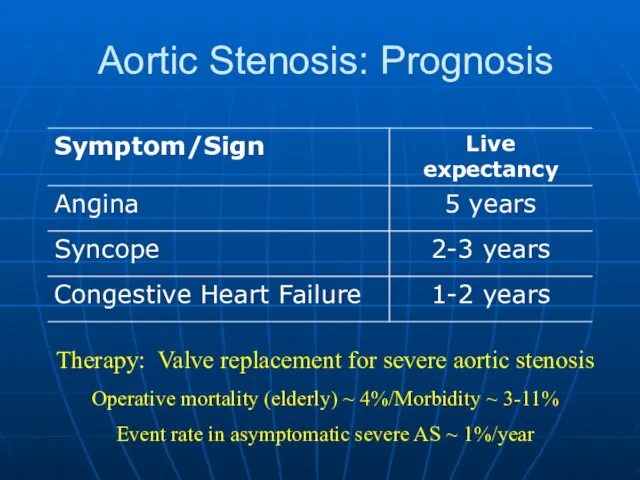
Aortic Stenosis: Prognosis
Therapy: Valve replacement for severe aortic stenosis
Operative mortality (elderly)
Aortic Stenosis: Prognosis
Therapy: Valve replacement for severe aortic stenosis
Operative mortality (elderly)
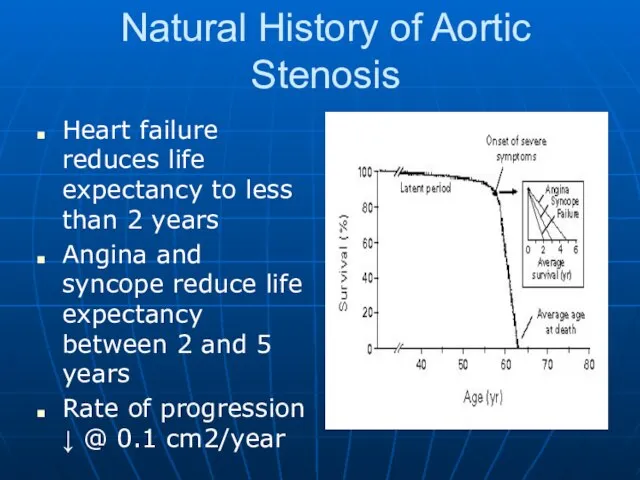
Natural History of Aortic Stenosis
Heart failure reduces life expectancy to less
Natural History of Aortic Stenosis
Heart failure reduces life expectancy to less

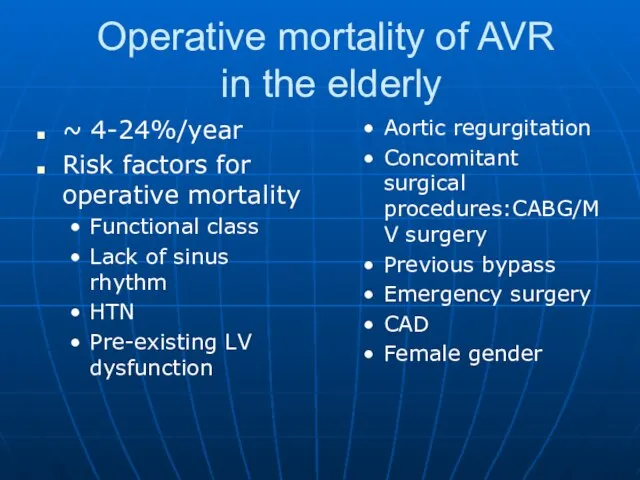
Operative mortality of AVR
in the elderly
~ 4-24%/year
Risk factors for operative
Operative mortality of AVR
in the elderly
~ 4-24%/year
Risk factors for operative
AVR is recommended in symptomatic
patients with severe AS (stage D1)
AVR is recommended in symptomatic patients with severe AS (stage D1)
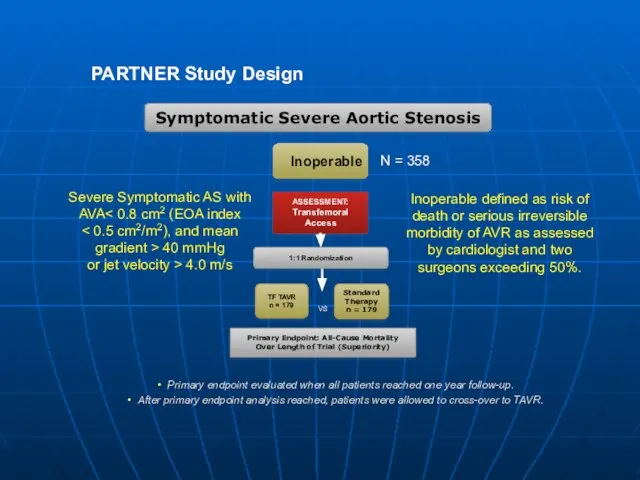
PARTNER Study Design
N = 358
Inoperable
Standard
Therapy
n = 179
ASSESSMENT: Transfemoral Access
TF TAVR
n =
PARTNER Study Design
N = 358
Inoperable
Standard
Therapy
n = 179
ASSESSMENT: Transfemoral Access
TF TAVR
n =
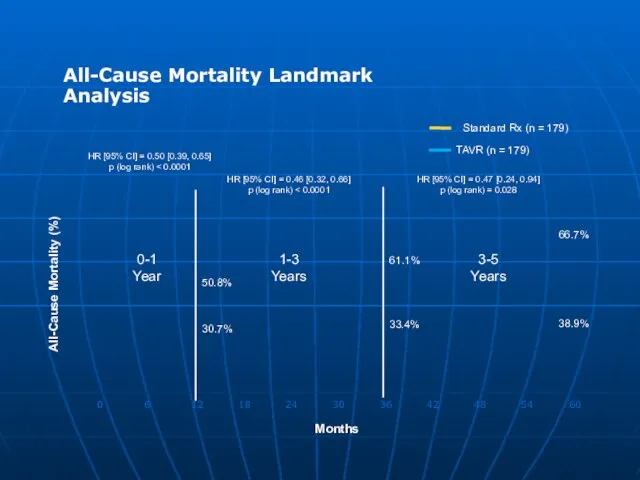
All-Cause Mortality Landmark Analysis
All-Cause Mortality Landmark Analysis


Prosthetic Heart Valves
Prosthetic Heart Valves

Caged-Ball Valve
Caged-Ball Valve
Disc Valve
Disc Valve
Bio-prosthetic Valve
Bio-prosthetic Valve
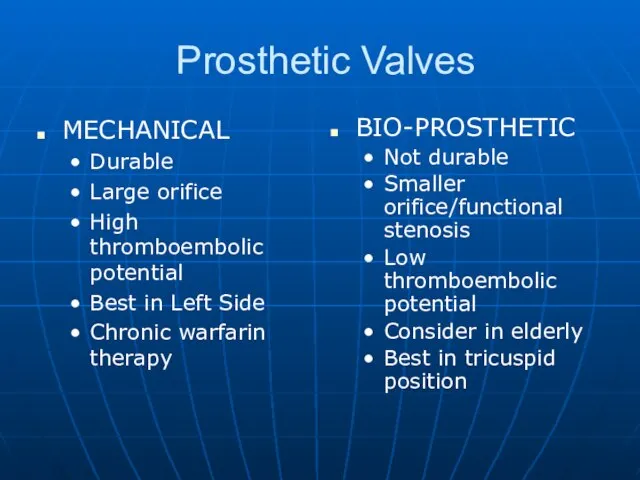
Prosthetic Valves
MECHANICAL
Durable
Large orifice
High thromboembolic potential
Best in Left Side
Chronic warfarin therapy
BIO-PROSTHETIC
Not durable
Smaller
Prosthetic Valves
MECHANICAL
Durable
Large orifice
High thromboembolic potential
Best in Left Side
Chronic warfarin therapy
BIO-PROSTHETIC
Not durable
Smaller
 Нарушения углеводного обмена. Сахарный диабет: определение, этиология, патогенез, классификация, клинические проявления
Нарушения углеводного обмена. Сахарный диабет: определение, этиология, патогенез, классификация, клинические проявления Факторные теории темперамента
Факторные теории темперамента Основы гигиены и физиологии труда
Основы гигиены и физиологии труда Родовая травма
Родовая травма Отчет специализации по нейрохирургии . Пусанский национальный университетский госпиталь. Южная Корея
Отчет специализации по нейрохирургии . Пусанский национальный университетский госпиталь. Южная Корея Дәрігер тәжірибесіндегі дәлелдемелі медицина. (Курс 3)
Дәрігер тәжірибесіндегі дәлелдемелі медицина. (Курс 3) Созылмалы лимфолейкоз
Созылмалы лимфолейкоз Детская анестезиология
Детская анестезиология Защита от кариеса
Защита от кариеса Десмургия 2
Десмургия 2 Дети и спорт
Дети и спорт Возможности лечения пенополиуретановым медицинским покрытием "ЛОКУС" ран различной этиологии
Возможности лечения пенополиуретановым медицинским покрытием "ЛОКУС" ран различной этиологии Топография таза и операции на органах таза
Топография таза и операции на органах таза Пельвиоперитонит
Пельвиоперитонит Менструальды циклдің бұзылысы
Менструальды циклдің бұзылысы Avoir une alimentation saine
Avoir une alimentation saine Врачебная этика Гиппократа
Врачебная этика Гиппократа Близнецы.Максутова С-106
Близнецы.Максутова С-106 Идиопатическая (иммунная) тромбоцито - пеническая пурпура у детей
Идиопатическая (иммунная) тромбоцито - пеническая пурпура у детей Электроимпедансный метод в современной диагностике (кардиография, томография, маммография)
Электроимпедансный метод в современной диагностике (кардиография, томография, маммография) Изменения метаболизма при гипофункции и гиперфункции коры надпочечников. Синдром Иценко-Кушинга
Изменения метаболизма при гипофункции и гиперфункции коры надпочечников. Синдром Иценко-Кушинга Послеродовые заболевания. Основные качественные показатели работы акушерского стационара
Послеродовые заболевания. Основные качественные показатели работы акушерского стационара Смешанные дистрофии
Смешанные дистрофии Особенности оказания медико-психологической и реабилитационной помощи комбатантам в Российской Федерации
Особенности оказания медико-психологической и реабилитационной помощи комбатантам в Российской Федерации Сухожильный шов
Сухожильный шов Водно-электролитные нарушения у хирургических больных, инфузионная терапия
Водно-электролитные нарушения у хирургических больных, инфузионная терапия Анафилактический шок. Роль медицинской сестры в профилактике и оказании первой доврачебной помощи
Анафилактический шок. Роль медицинской сестры в профилактике и оказании первой доврачебной помощи Пищеварительная система. Передний отдел жкт. Пищеварение в ротовой полости
Пищеварительная система. Передний отдел жкт. Пищеварение в ротовой полости