- Disorders of Calcium Metabolism

Содержание
- 2. Calcium An essential intracellular and extracellular cation Extracellular calcium is required to maintain normal biological function
- 3. calcium 40-45 % ionized 40-45 % albumin bound 10% complexed citrate, sulphate 8.5–10.5 mg/dl ECF Filtration
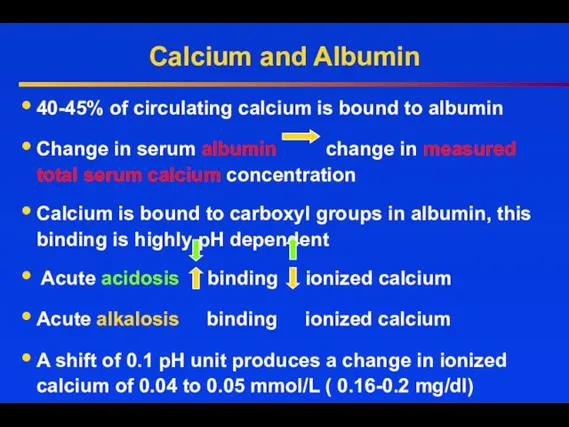
- 4. Calcium and Albumin 40-45% of circulating calcium is bound to albumin Change in serum albumin change
- 5. Calcium and Albumin At pH 7.4 each g/dl of serum albumin binds 0.8 mg/dl of calcium
- 6. Disorders of Calcium Metabolism Hypercalcemia Serum Calcium >10.4 mg/dl Hypocalcemia Serum Calcium
- 7. Causes of hypercalcemia PTH-mediated Primary hyperparathyroidism (sporadic) –solitary adenoma or hyperplasia Familial MEN1 and -2a FHH
- 8. Causes of hypercalcemia Vitamin D intoxication Chronic granulomatous disorders: Activation of extrarenal 1 alpha-hydroxylase (increased calcitriol)
- 9. Diagnosis of Hypercalcemia Serum Ca ⭡ Measure serum albumin or ionized calcium Albumin corrected calcium normal
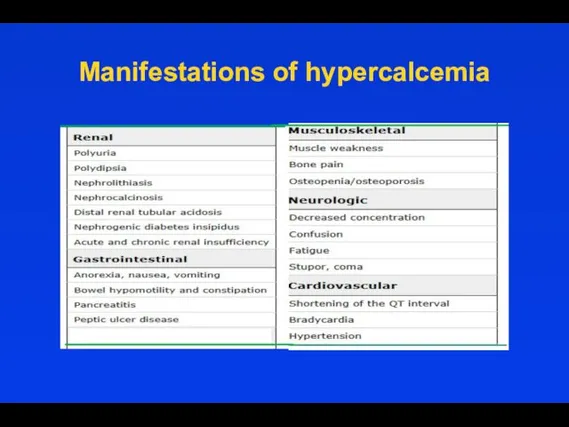
- 10. Manifestations of hypercalcemia
- 11. Renal manifestations The most important renal manifestations are polyuria, resulting from decreased concentrating ability in the
- 12. Renal manifestations Nephrolithiasis — When hypercalcemia is due to primary hyperparathyroidism or sarcoidosis, it is often
- 13. Gastrointestinal manifestations Nausea. Constipation may be related to decreased smooth muscle tone and/or abnormal autonomic function.
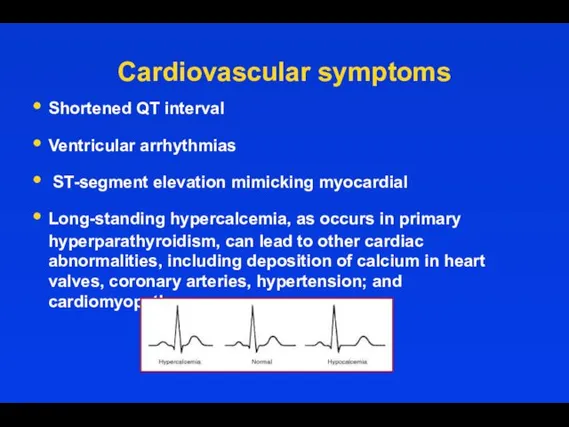
- 14. Cardiovascular symptoms Shortened QT interval Ventricular arrhythmias ST-segment elevation mimicking myocardial Long-standing hypercalcemia, as occurs in
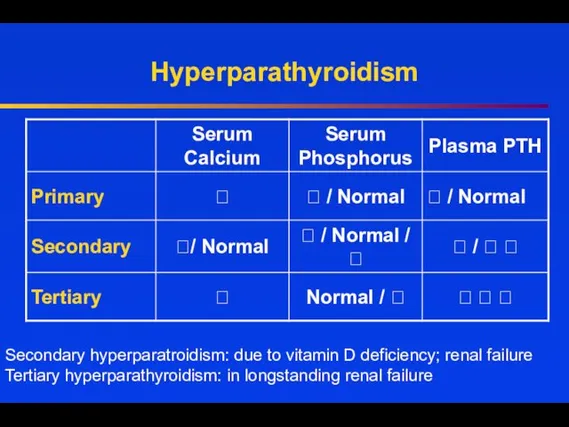
- 15. Hyperparathyroidism Secondary hyperparatroidism: due to vitamin D deficiency; renal failure Tertiary hyperparathyroidism: in longstanding renal failure
- 16. Primary Hyperparathyroidism Incidence 1/1000- 42/100 000 Postmenopausal women 1/200; ⭡ X 3.0 in women then in
- 17. or multiple adenomas, nearly 100% 15-20% up to 60% nearly 100% 30-100% 10-25%
- 18. Clinical Manifestations of Prim Hyperparathyroidism CNS - Cognitive difficulties, apathy, drowsiness, obtundation or even coma GI
- 19. Bone and Joint Manifestations in Primary Hyperparathyroidism Osteoporosis Diffuse bone pain Osteitis fibrosa cystica Diffuse demineralization
- 22. Treatment When is surgery indicated in PHPT patients ?
- 23. Guidelines for Surgery
- 24. Other Considerations Neuropsychological disturbances Weakness and easy fatigability Depression Intellectual weariness Increased sleep requirements Improved by
- 25. US in the diagnosis of PTA
- 26. 99mTc- sestamibi Parathyroid Scan 20 min 3 hours 90% sensitivity in parathyroid tissue detection
- 27. What is 4D-CT? 4D-CT includes image sets in three planes (axial, coronal, sagittal) from the angle
- 28. 4D CT in diagnosis of PHPT Arterial phase images are acquired 25 seconds after the start
- 29. Patients who weren‘t operated- Monitoring guidelines
- 30. General Measures Hydration Adequate Mobility Diet neither restrictive nor excessive in calcium Adequate vitamin D status
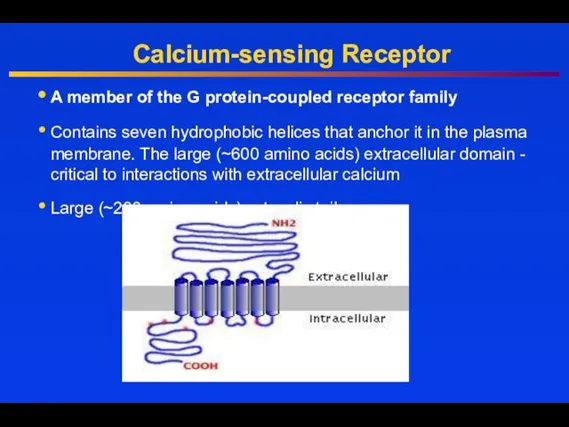
- 31. Calcium-sensing Receptor A member of the G protein-coupled receptor family Contains seven hydrophobic helices that anchor
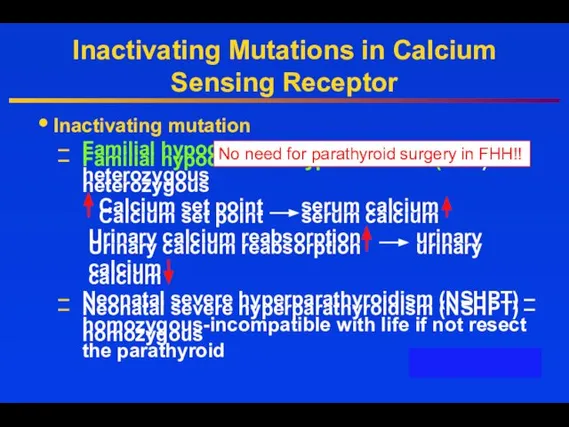
- 32. Inactivating Mutations in Calcium Sensing Receptor Inactivating mutation Familial hypocalciuric hypercalcemia (FHH) - heterozygous Calcium set
- 33. Hypercalcemia of Malignancy Lung, breast, and prostate cancer frequently invade skeleton and destroy bone tissue Damage
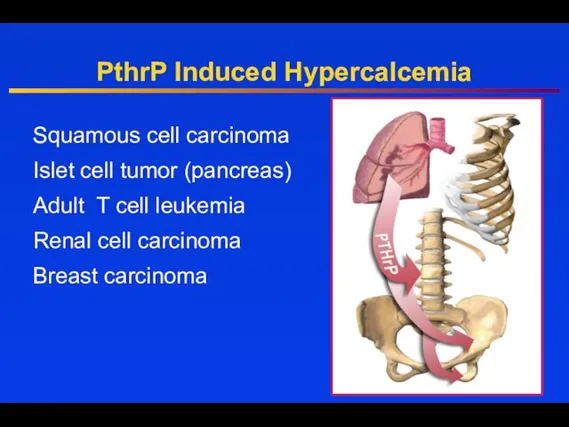
- 34. PthrP Induced Hypercalcemia Squamous cell carcinoma Islet cell tumor (pancreas) Adult T cell leukemia Renal cell
- 35. PTHrP-PTH related peptide Gen located on the chromosome 12 Gen is expressed in the embrional tissues:
- 36. Treatment Hydration Bisphosphonates IV, Denosumab Calcitonin Glucocorticoids Dialysis
- 37. Hydration First step in the management of severe hypercalcemia - Isotonic saline Usually ⭣ serum calcium
- 38. Loop Diuretics In the past intensive administration of furosemide was used (80 to 100 mg every
- 39. Calcitonin The efficacy of calcitonin (4 IU/kg every 6-12 hours) is limited to the first 48
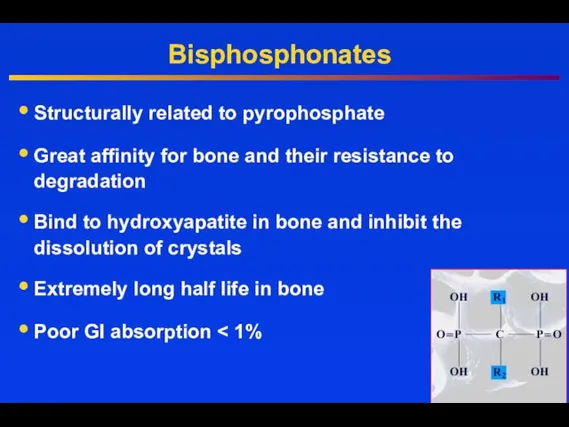
- 40. Bisphosphonates Structurally related to pyrophosphate Great affinity for bone and their resistance to degradation Bind to
- 41. Zoledronic Acid (ZOMERA) Zoledronic acid belongs to a new class of highly potent bisphosphonates Heterocyclic, nitrogen-containing
- 42. Denosumab Mechanism of Action © 2007 Amgen. All rights reserved. RANKL RANK OPG Denosumab Bone Formation
- 43. Inhibit the growth of neoplastic lymphoid tissue Counteract the effects of vitamin D Glucocorticoids
- 44. Low PTH Hypocalcemia
- 45. Hypocalcemia Low PTH (hypoparathyroidism) Genetic disorders: Abnormal parathyroid gland development Abnormal PTH synthesis; Activating mutations of
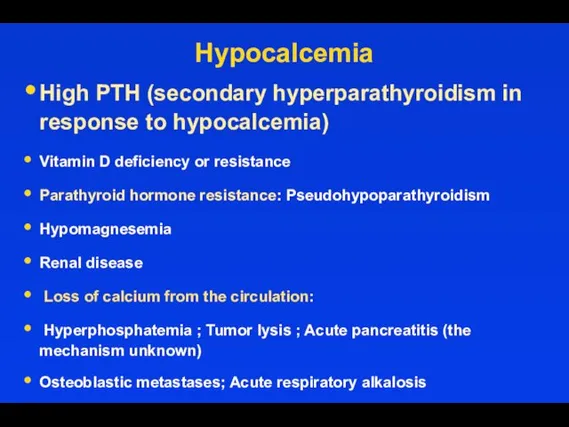
- 46. Hypocalcemia High PTH (secondary hyperparathyroidism in response to hypocalcemia) Vitamin D deficiency or resistance Parathyroid hormone
- 47. Drugs induced hypocalcemia Inhibitors of bone resorption (bisphosphonates, calcitonin, denosumab), especially in vitamin D deficiency Cinacalcet
- 48. Trousseau's sign is the induction of carpopedal spasm by inflation of a sphygmomanometer above systolic blood
- 49. Hypocalcemia: Carpopedal spasm and ECG changes Carpopedal Spasm Sinus rhythm with diffuse T wave inversion QT
- 50. Treatment of Acute Hypocalcemia Promptly correct symptomatic or severe hypocalcemia with cardiac arrhythmias or tetany with
- 51. Treatment of Acute Hypocalcemia For those with milder symptoms of neuromuscular irritability (paresthesias) and corrected serum
- 52. To prevent Hypocalcemia due to Hungry bone syndrome Start oral calcium and vitamin D treatment early.
- 53. Primary hypoparathyroidism
- 58. Natpara Natpara- for use in patients who can’t be normalized on regular oral therapy, or have
- 59. Causes of magnesium depletion Causes of magnesium depletion Renal losses Gasro-intestinal losses
- 60. Treatment of Hypomagnesemia If the serum magnesium concentration is low, 2 g (16 mEq) of magnesium
- 61. Treatment of Hypomagnesemia Oral repletion- if available and tolerable. A typical daily dose in a patient
- 63. Скачать презентацию

Calcium
An essential intracellular and extracellular cation
Extracellular calcium is required to maintain
Calcium
An essential intracellular and extracellular cation
Extracellular calcium is required to maintain

calcium
40-45 %
ionized
40-45 %
albumin
bound
10%
complexed
citrate, sulphate
8.5–10.5 mg/dl
ECF
Filtration
5-7gr
Reabsorption
4.9-6.7gr
98%
Diet 0.5-1.5 gr
Absorption
0.25-0.5gr
Secretion
0.1-0.2gr
Feces
0.35-0.6gr
Resorption
0.3-0.5 g
Formation
0.3-0.5 g
Bone
1000
calcium
40-45 %
ionized
40-45 %
albumin
bound
10%
complexed
citrate, sulphate
8.5–10.5 mg/dl
ECF
Filtration
5-7gr
Reabsorption
4.9-6.7gr
98%
Diet 0.5-1.5 gr
Absorption
0.25-0.5gr
Secretion
0.1-0.2gr
Feces
0.35-0.6gr
Resorption
0.3-0.5 g
Formation
0.3-0.5 g
Bone
1000
Calcium and Albumin
40-45% of circulating calcium is bound to albumin
Change
Calcium and Albumin
40-45% of circulating calcium is bound to albumin
Change

Calcium and Albumin
At pH 7.4 each g/dl of serum albumin binds
Calcium and Albumin
At pH 7.4 each g/dl of serum albumin binds
Disorders of Calcium Metabolism
Hypercalcemia Serum Calcium >10.4 mg/dl
Hypocalcemia Serum Calcium <
Disorders of Calcium Metabolism
Hypercalcemia Serum Calcium >10.4 mg/dl
Hypocalcemia Serum Calcium <

Causes of hypercalcemia
PTH-mediated
Primary hyperparathyroidism (sporadic) –solitary adenoma or hyperplasia
Familial MEN1
Causes of hypercalcemia
PTH-mediated
Primary hyperparathyroidism (sporadic) –solitary adenoma or hyperplasia
Familial MEN1

Causes of hypercalcemia
Vitamin D intoxication
Chronic granulomatous disorders: Activation of extrarenal 1
Causes of hypercalcemia
Vitamin D intoxication
Chronic granulomatous disorders: Activation of extrarenal 1
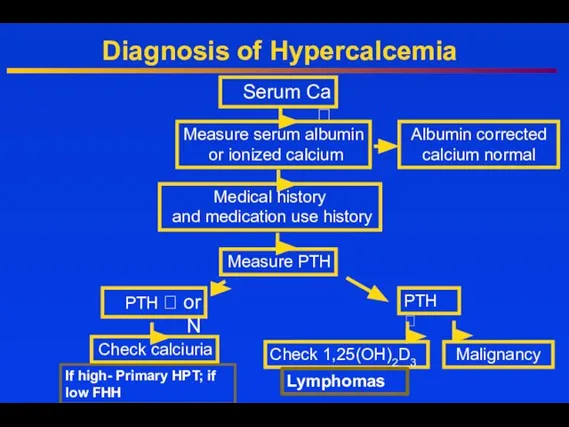
Diagnosis of Hypercalcemia
Serum Ca ⭡
Measure serum albumin
or ionized calcium
Albumin corrected
Diagnosis of Hypercalcemia
Serum Ca ⭡
Measure serum albumin
or ionized calcium
Albumin corrected
Manifestations of hypercalcemia
Manifestations of hypercalcemia
Renal manifestations
The most important renal manifestations are polyuria, resulting from decreased
Renal manifestations
The most important renal manifestations are polyuria, resulting from decreased

Renal manifestations
Nephrolithiasis — When hypercalcemia is due to primary hyperparathyroidism or
Renal manifestations
Nephrolithiasis — When hypercalcemia is due to primary hyperparathyroidism or
Gastrointestinal manifestations
Nausea.
Constipation may be related to decreased smooth muscle tone
Gastrointestinal manifestations
Nausea.
Constipation may be related to decreased smooth muscle tone
Cardiovascular symptoms
Shortened QT interval
Ventricular arrhythmias
ST-segment elevation mimicking myocardial
Long-standing hypercalcemia,
Cardiovascular symptoms
Shortened QT interval
Ventricular arrhythmias
ST-segment elevation mimicking myocardial
Long-standing hypercalcemia,
Hyperparathyroidism
Secondary hyperparatroidism: due to vitamin D deficiency; renal failure Tertiary hyperparathyroidism:
Hyperparathyroidism
Secondary hyperparatroidism: due to vitamin D deficiency; renal failure Tertiary hyperparathyroidism:

Primary Hyperparathyroidism
Incidence 1/1000- 42/100 000
Postmenopausal women 1/200;
⭡ X 3.0 in
Primary Hyperparathyroidism
Incidence 1/1000- 42/100 000
Postmenopausal women 1/200;
⭡ X 3.0 in

or multiple adenomas, nearly 100%
15-20%
up to 60%
nearly 100%
30-100%
10-25%
or multiple adenomas, nearly 100%
15-20%
up to 60%
nearly 100%
30-100%
10-25%
Clinical Manifestations of Prim Hyperparathyroidism
CNS - Cognitive difficulties, apathy, drowsiness, obtundation
Clinical Manifestations of Prim Hyperparathyroidism
CNS - Cognitive difficulties, apathy, drowsiness, obtundation

Bone and Joint Manifestations in Primary Hyperparathyroidism
Osteoporosis
Diffuse bone pain
Osteitis fibrosa cystica
Diffuse
Bone and Joint Manifestations in Primary Hyperparathyroidism
Osteoporosis
Diffuse bone pain
Osteitis fibrosa cystica
Diffuse



Treatment
When is surgery indicated in PHPT patients
?
Treatment
When is surgery indicated in PHPT patients
?

Guidelines for Surgery
Guidelines for Surgery

Other Considerations
Neuropsychological disturbances
Weakness and easy fatigability
Depression
Intellectual weariness
Increased sleep requirements
Improved by surgery
Onset
Other Considerations
Neuropsychological disturbances
Weakness and easy fatigability
Depression
Intellectual weariness
Increased sleep requirements
Improved by surgery
Onset

US in the diagnosis of PTA
US in the diagnosis of PTA

99mTc- sestamibi Parathyroid Scan
20 min
3 hours
90% sensitivity in parathyroid
tissue detection
99mTc- sestamibi Parathyroid Scan
20 min
3 hours
90% sensitivity in parathyroid
tissue detection
What is 4D-CT?
4D-CT includes image sets in three planes (axial, coronal,
What is 4D-CT?
4D-CT includes image sets in three planes (axial, coronal,

4D CT in diagnosis of PHPT
Arterial phase images are acquired 25
4D CT in diagnosis of PHPT
Arterial phase images are acquired 25

Patients who weren‘t operated- Monitoring guidelines
Patients who weren‘t operated- Monitoring guidelines

General Measures
Hydration
Adequate Mobility
Diet neither restrictive nor excessive in calcium
Adequate vitamin D
General Measures
Hydration
Adequate Mobility
Diet neither restrictive nor excessive in calcium
Adequate vitamin D
Calcium-sensing Receptor
A member of the G protein-coupled receptor family
Contains seven
Calcium-sensing Receptor
A member of the G protein-coupled receptor family
Contains seven
Inactivating Mutations in Calcium Sensing Receptor
Inactivating mutation
Familial hypocalciuric hypercalcemia (FHH) -
Inactivating Mutations in Calcium Sensing Receptor
Inactivating mutation
Familial hypocalciuric hypercalcemia (FHH) -
Hypercalcemia of Malignancy
Lung, breast, and prostate cancer frequently invade skeleton and
Hypercalcemia of Malignancy
Lung, breast, and prostate cancer frequently invade skeleton and
PthrP Induced Hypercalcemia
Squamous cell carcinoma
Islet cell tumor (pancreas)
Adult T cell leukemia
Renal
PthrP Induced Hypercalcemia
Squamous cell carcinoma
Islet cell tumor (pancreas)
Adult T cell leukemia
Renal

PTHrP-PTH related peptide
Gen located on the chromosome 12
Gen is expressed in
PTHrP-PTH related peptide
Gen located on the chromosome 12
Gen is expressed in
Treatment
Hydration
Bisphosphonates IV, Denosumab
Calcitonin
Glucocorticoids
Dialysis
Treatment
Hydration
Bisphosphonates IV, Denosumab
Calcitonin
Glucocorticoids
Dialysis
Hydration
First step in the management of severe hypercalcemia - Isotonic saline
Usually
Hydration
First step in the management of severe hypercalcemia - Isotonic saline
Usually

Loop Diuretics
In the past intensive administration of furosemide was used (80
Loop Diuretics
In the past intensive administration of furosemide was used (80
Calcitonin
The efficacy of calcitonin (4 IU/kg every 6-12 hours) is limited
Calcitonin
The efficacy of calcitonin (4 IU/kg every 6-12 hours) is limited
Bisphosphonates
Structurally related to pyrophosphate
Great affinity for bone and their resistance to
Bisphosphonates
Structurally related to pyrophosphate
Great affinity for bone and their resistance to

Zoledronic Acid (ZOMERA)
Zoledronic acid belongs to a new class of highly
Zoledronic Acid (ZOMERA)
Zoledronic acid belongs to a new class of highly

Denosumab Mechanism of Action
© 2007 Amgen. All rights reserved.
RANKL
RANK
OPG
Denosumab
Bone Formation
Hormones
Growth factors
Cytokines
Bone
Denosumab Mechanism of Action
© 2007 Amgen. All rights reserved.
RANKL
RANK
OPG
Denosumab
Bone Formation
Hormones
Growth factors
Cytokines
Bone

Inhibit the growth of neoplastic lymphoid tissue
Counteract the effects of vitamin
Inhibit the growth of neoplastic lymphoid tissue
Counteract the effects of vitamin

Low PTH Hypocalcemia
Low PTH Hypocalcemia

Hypocalcemia
Low PTH (hypoparathyroidism)
Genetic disorders: Abnormal parathyroid gland development
Abnormal PTH
Hypocalcemia
Low PTH (hypoparathyroidism)
Genetic disorders: Abnormal parathyroid gland development
Abnormal PTH
Hypocalcemia
High PTH (secondary hyperparathyroidism in response to hypocalcemia)
Vitamin D deficiency
Hypocalcemia
High PTH (secondary hyperparathyroidism in response to hypocalcemia)
Vitamin D deficiency
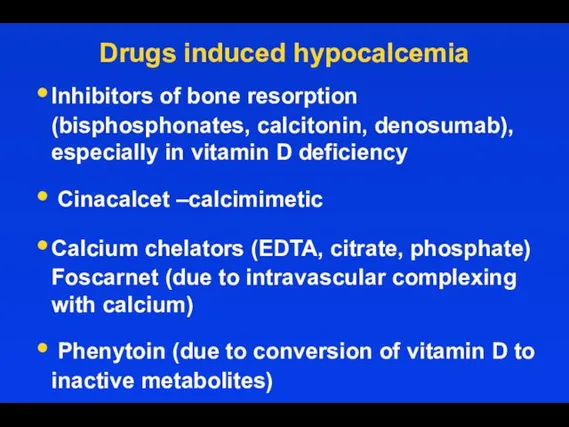
Drugs induced hypocalcemia
Inhibitors of bone resorption (bisphosphonates, calcitonin, denosumab), especially in
Drugs induced hypocalcemia
Inhibitors of bone resorption (bisphosphonates, calcitonin, denosumab), especially in

Trousseau's sign is the induction of carpopedal spasm by inflation of
Trousseau's sign is the induction of carpopedal spasm by inflation of
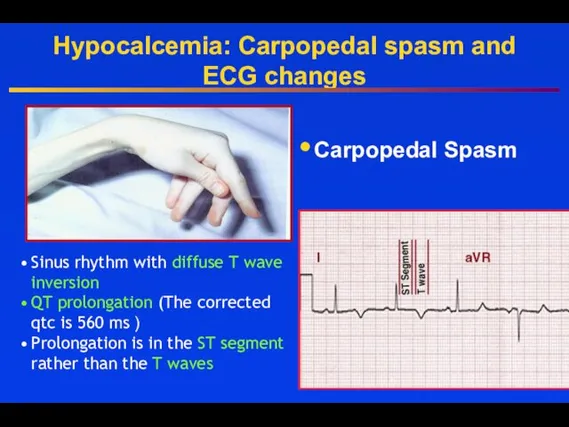
Hypocalcemia: Carpopedal spasm and ECG changes
Carpopedal Spasm
Sinus rhythm with diffuse T
Hypocalcemia: Carpopedal spasm and ECG changes
Carpopedal Spasm
Sinus rhythm with diffuse T
Treatment of Acute Hypocalcemia
Promptly correct symptomatic or severe hypocalcemia with cardiac
Treatment of Acute Hypocalcemia
Promptly correct symptomatic or severe hypocalcemia with cardiac

Treatment of Acute Hypocalcemia
For those with milder symptoms of neuromuscular irritability
Treatment of Acute Hypocalcemia
For those with milder symptoms of neuromuscular irritability
To prevent Hypocalcemia due to Hungry bone syndrome
Start oral calcium and
To prevent Hypocalcemia due to Hungry bone syndrome
Start oral calcium and

Primary hypoparathyroidism
Primary hypoparathyroidism




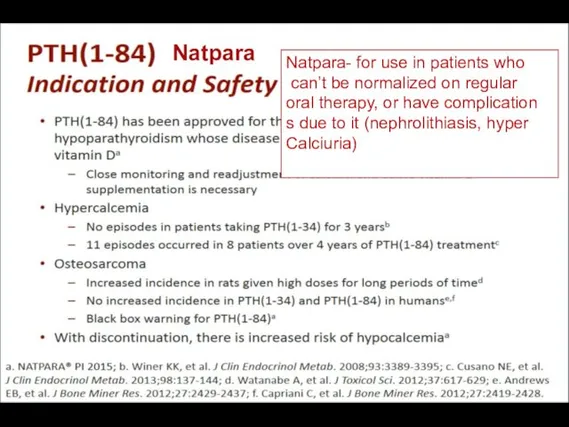
Natpara
Natpara- for use in patients who
can’t be normalized on regular
Natpara
Natpara- for use in patients who
can’t be normalized on regular

Causes of magnesium depletion
Causes of magnesium depletion
Renal losses
Gasro-intestinal losses
Causes of magnesium depletion
Causes of magnesium depletion
Renal losses
Gasro-intestinal losses

Treatment of Hypomagnesemia
If the serum magnesium concentration is low, 2 g
Treatment of Hypomagnesemia
If the serum magnesium concentration is low, 2 g

Treatment of Hypomagnesemia
Oral repletion- if available and tolerable.
A typical daily
Treatment of Hypomagnesemia
Oral repletion- if available and tolerable.
A typical daily
 Окклюзионные нарушения мезентериального кровообращения
Окклюзионные нарушения мезентериального кровообращения Роль взрослого в развитии общения ребенка
Роль взрослого в развитии общения ребенка философия и медицина
философия и медицина Исследование маркеров эффективности трансляции в постуральной мышце человека в условиях 3 - суточной женской иммерсии
Исследование маркеров эффективности трансляции в постуральной мышце человека в условиях 3 - суточной женской иммерсии Венозное полнокровие. Кровоизлияния
Венозное полнокровие. Кровоизлияния Анатомо-физиологические особенности недоношенных детей
Анатомо-физиологические особенности недоношенных детей Методология консультирования женщин, идущих на прерывание беременности
Методология консультирования женщин, идущих на прерывание беременности Зудящие дерматозы
Зудящие дерматозы Биологический метод лечения пульпита. Показания, противопоказания, методика
Биологический метод лечения пульпита. Показания, противопоказания, методика Снотворные, противосудорожные (противоэпилептические, противопаркинсонические), обезболивающие ЛС
Снотворные, противосудорожные (противоэпилептические, противопаркинсонические), обезболивающие ЛС Воронкообразная деформация грудины у котёнка
Воронкообразная деформация грудины у котёнка Острая почечная недостаточность
Острая почечная недостаточность Современный подросток. Физическое здоровье (Методическое пособие)
Современный подросток. Физическое здоровье (Методическое пособие) Инфекционные заболевания
Инфекционные заболевания Проблемы защиты персональных данных в медицине
Проблемы защиты персональных данных в медицине Новорожденные щенки. Содержание, болезни, документы
Новорожденные щенки. Содержание, болезни, документы Медицинская реабилитация в гинекологии
Медицинская реабилитация в гинекологии Клиническая иммунология детского возраста
Клиническая иммунология детского возраста Проблемы нечистоплотности кошек и собак. Поведенческий и клинический аспекты
Проблемы нечистоплотности кошек и собак. Поведенческий и клинический аспекты Йогатерапия дисменореи в сочетании с варикозной болезнью нижних конечностей и малого таза
Йогатерапия дисменореи в сочетании с варикозной болезнью нижних конечностей и малого таза Учения об иммунитете
Учения об иммунитете Септический шок в акушерско-гинекологической практике
Септический шок в акушерско-гинекологической практике Современные методы хирургического лечения варикозной болезни нижних конечностей
Современные методы хирургического лечения варикозной болезни нижних конечностей Снижение смертности от болезней системы кровообращения
Снижение смертности от болезней системы кровообращения Гнойные заболевания пальцев и кисти
Гнойные заболевания пальцев и кисти ЛФК при заболеваниях дыхательной системы
ЛФК при заболеваниях дыхательной системы Эндокринология. Физиология половой дисфункции
Эндокринология. Физиология половой дисфункции Основы лечебно - эвакуационного обеспечения пораженных
Основы лечебно - эвакуационного обеспечения пораженных