- Otitis Externa

Содержание
- 3. Otitis Externa Inflammation of the external auditory canal Most common in children 7-14 years old Risk
- 4. Otitis Externa Diagnosis: clinical, otoscopy, culture (for refractory cases), imaging (mastoiditis) Treatment: Clean the ear canal
- 5. Malignant (necrotizing) Otitis Externa Infection of the temporal bone Most common in elderly, diabetics, immunocompromised patients
- 6. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
- 7. Acute otitis media Most common in children 3 month-3years Symptoms: blocked ear feeling, pain and fever.
- 9. Acute otitis media Treatment Analgesics to relieve pain Adequate rest in a warm room Nasal decongestants
- 10. Acute otitis media Complications: Conductive hearing loss Sensorineural hearing loss Tympanic membrane perforation Retraction pocket Mastoiditis
- 11. Mandy, a 4 year old girl, is due to accompany her parents on a flight to
- 12. A 8 year old boy with recurrent attacks of otitis media is suspected of developing a
- 13. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
- 14. Chronic otitis media Symptoms: deafness and discharge without pain Causes: Pseudomonas aeruginosa Staphylococcus aureus Proteus sp.
- 15. Chronic otitis media ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Safe Perforation Affects mucosa of the lower front part of
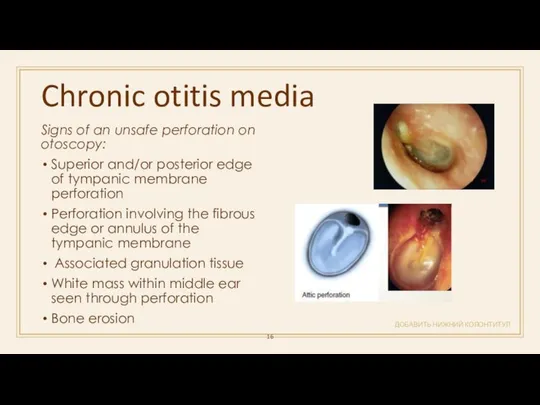
- 16. Chronic otitis media ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Signs of an unsafe perforation on otoscopy: Superior and/or posterior
- 17. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ A 14-year old teenager is diagnosed with a tympanic membrane perforation secondary to
- 18. Cholesteatoma ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Expanding lesions of the temporal bone composed of a stratified squamous outer
- 19. Cholesteatoma ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Complications: Hearing loss secondary to necrosis of the long process of the
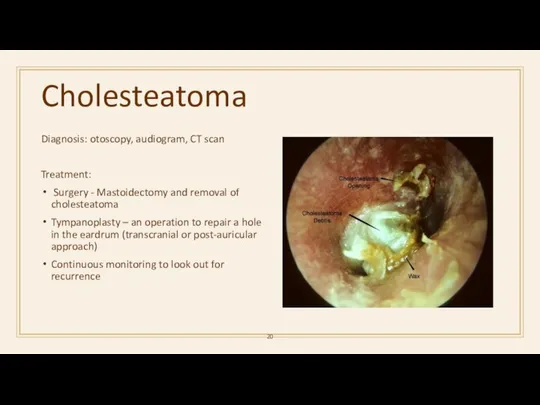
- 20. Cholesteatoma Diagnosis: otoscopy, audiogram, CT scan Treatment: Surgery - Mastoidectomy and removal of cholesteatoma Tympanoplasty –
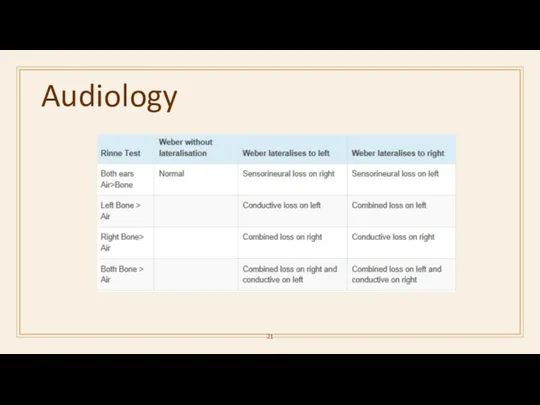
- 21. Audiology
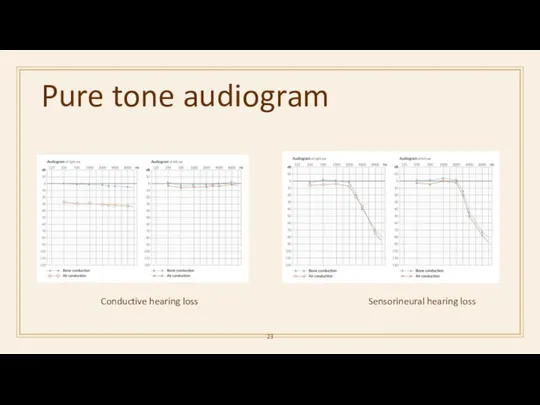
- 23. Pure tone audiogram Sensorineural hearing loss Conductive hearing loss
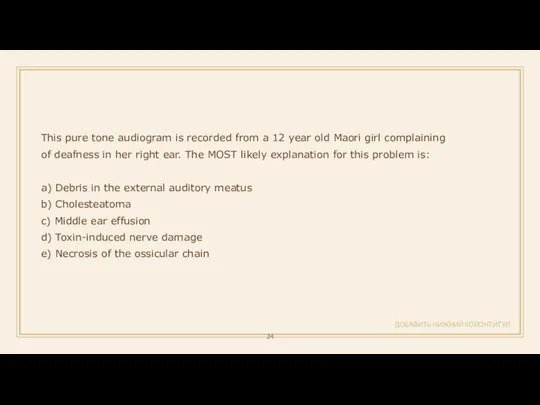
- 24. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ This pure tone audiogram is recorded from a 12 year old Maori girl
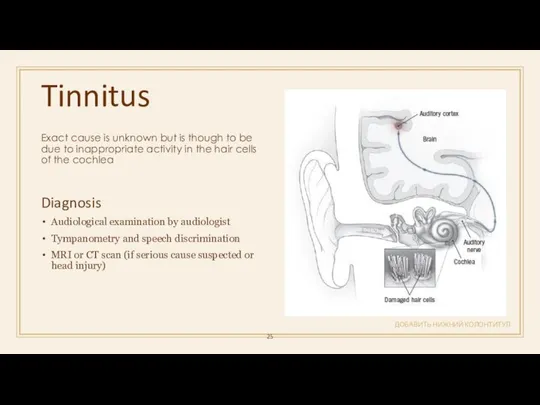
- 25. Tinnitus ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Exact cause is unknown but is though to be due to inappropriate
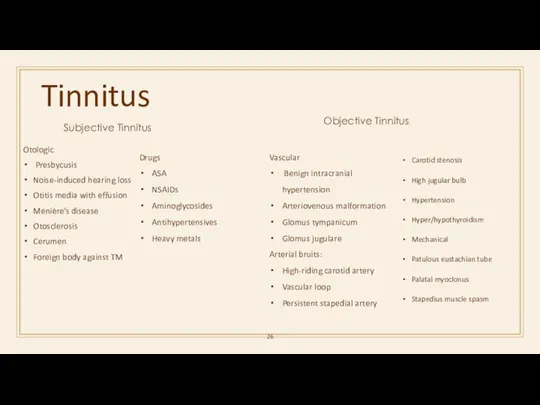
- 26. Tinnitus Subjective Tinnitus Otologic Presbycusis Noise-induced hearing loss Otitis media with effusion Menière’s disease Otosclerosis Cerumen
- 27. Tinnitus ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Holistic approach (options) Mainly based on acoustic de-sensitisation: • Relaxation techniques •
- 28. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ You review a 70-year-old woman who is on multiple medications. For the past
- 29. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
- 30. Benign paroxysmal positional vertigo ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Acute vertigo that is induced by changing head position
- 31. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ A 52-year-old woman presents with dizziness and vertigo when she moves her head
- 32. Vestibular neuritis Second most common disorder affecting the labyrinth Viral etiology with consequent inflammation of the
- 33. Vestibular neuritis ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Treatment: Bed rest, vestibular sedatives and anti-emetics in the first 24-72
- 35. Meniere’s disease ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ It is commonest in the 30–50 years age group Triggers: high
- 36. Meniere disease ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ DxT vertigo + vomiting + tinnitus + sensorineural deafenss → Ménière
- 37. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ An elderly patient has acute onset unilateral deafness, tinnitis & vertigo. What is
- 38. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ A 39-year-old woman arrives at the hospital after her third episode of dizziness.
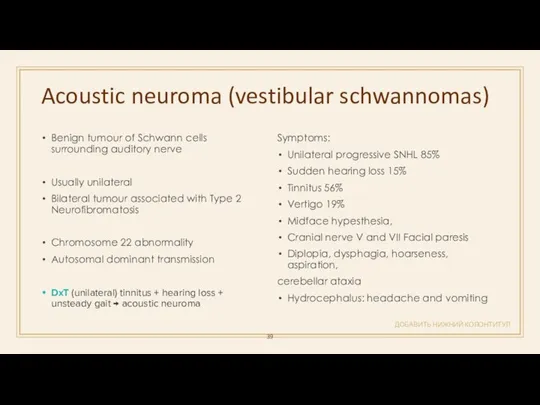
- 39. Acoustic neuroma (vestibular schwannomas) ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Benign tumour of Schwann cells surrounding auditory nerve Usually
- 40. Acoustic neuroma ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Diagnosis: audiometry (SNHL), MRI, CT Treatment: Conservative: monitoring Surgical resection Translabyrinthine,
- 41. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Which of the following is least likely to cause facial nerve palsy? a)
- 42. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
- 43. Otosclerosis ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Disease of the bone surrounding the inner ear and is the most
- 44. Otosclerosis ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Treatment Referral to an ENT consultant Stapedectomy (approximately 90% effective) Hearing aid
- 45. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Which of the following is most likely to be associated with otosclerosis? a)
- 46. ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
- 47. Head and neck masses ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
- 48. Cystic lesions of the neck ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
- 49. Cystic hygroma ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Commonly involves the posterior cervical space May be macrocystic or
- 50. Branchial deft cyst ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ located inferior to the external auditory meatus or anterior to
- 51. Thyroglossal duct cyst ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ the most common childhood midline neck swelling It moves with
- 52. Carotid body tumor ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ Carotid body tumors (CBTs) present most commonly as an asymptomatic
- 54. Скачать презентацию
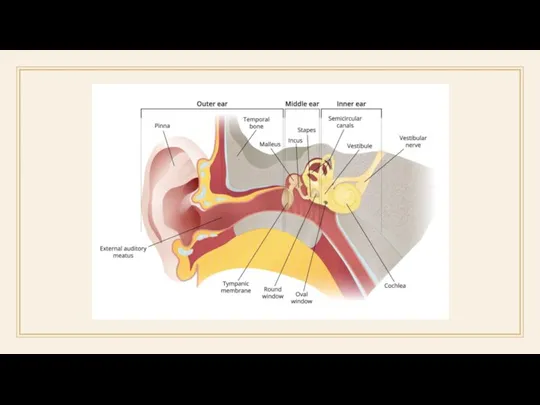
Otitis Externa
Inflammation of the external auditory canal
Most common in children 7-14
Otitis Externa
Inflammation of the external auditory canal
Most common in children 7-14
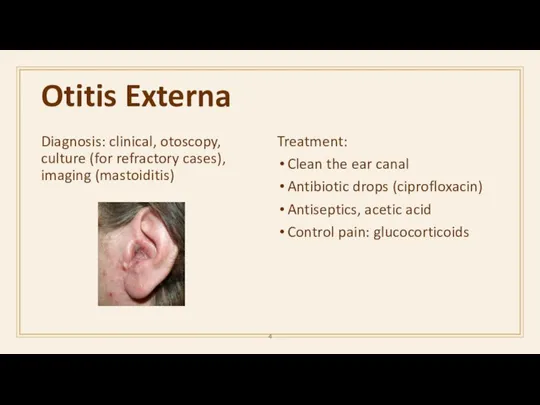
Otitis Externa
Diagnosis: clinical, otoscopy, culture (for refractory cases), imaging (mastoiditis)
Treatment:
Clean the
Otitis Externa
Diagnosis: clinical, otoscopy, culture (for refractory cases), imaging (mastoiditis)
Treatment:
Clean the
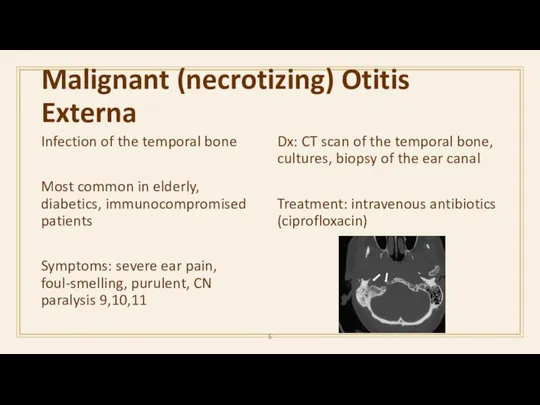
Malignant (necrotizing) Otitis Externa
Infection of the temporal bone
Most common in elderly,
Malignant (necrotizing) Otitis Externa
Infection of the temporal bone
Most common in elderly,

ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
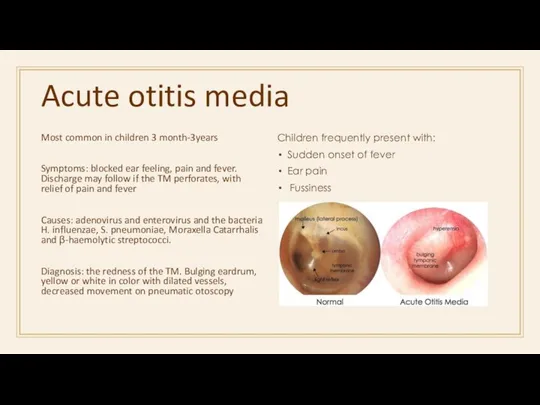
Acute otitis media
Most common in children 3 month-3years
Symptoms: blocked ear feeling,
Acute otitis media
Most common in children 3 month-3years
Symptoms: blocked ear feeling,
Acute otitis media
Treatment
Analgesics to relieve pain
Adequate rest in a warm room
Nasal
Acute otitis media
Treatment
Analgesics to relieve pain
Adequate rest in a warm room
Nasal
Acute otitis media
Complications:
Conductive hearing loss
Sensorineural hearing loss
Tympanic membrane perforation
Retraction pocket
Mastoiditis
Petrositis
Labyrinthitis
Perilymphatic fistula
Cholesteatoma
Tympanosclerosis
Cholesterol
Acute otitis media
Complications:
Conductive hearing loss
Sensorineural hearing loss
Tympanic membrane perforation
Retraction pocket
Mastoiditis
Petrositis
Labyrinthitis
Perilymphatic fistula
Cholesteatoma
Tympanosclerosis
Cholesterol
Mandy, a 4 year old girl, is due to accompany her
Mandy, a 4 year old girl, is due to accompany her
A 8 year old boy with recurrent attacks of otitis media
A 8 year old boy with recurrent attacks of otitis media
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
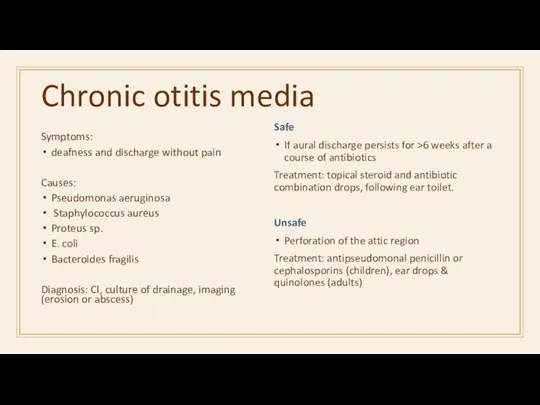
Chronic otitis media
Symptoms:
deafness and discharge without pain
Causes:
Pseudomonas aeruginosa
Staphylococcus aureus
Proteus
Chronic otitis media
Symptoms:
deafness and discharge without pain
Causes:
Pseudomonas aeruginosa
Staphylococcus aureus
Proteus
Chronic otitis media
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Safe Perforation
Affects mucosa of the lower front
Chronic otitis media
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Safe Perforation
Affects mucosa of the lower front
Chronic otitis media
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Signs of an unsafe perforation on otoscopy:
Superior
Chronic otitis media
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Signs of an unsafe perforation on otoscopy:
Superior
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
A 14-year old teenager is diagnosed with a tympanic
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
A 14-year old teenager is diagnosed with a tympanic
Cholesteatoma
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Expanding lesions of the temporal bone composed of a
Cholesteatoma
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Expanding lesions of the temporal bone composed of a
Cholesteatoma
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Complications:
Hearing loss secondary to necrosis of the long process
Cholesteatoma
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Complications:
Hearing loss secondary to necrosis of the long process
Cholesteatoma
Diagnosis: otoscopy, audiogram, CT scan
Treatment:
Surgery - Mastoidectomy and removal of
Cholesteatoma
Diagnosis: otoscopy, audiogram, CT scan
Treatment:
Surgery - Mastoidectomy and removal of
Audiology
Audiology
Pure tone audiogram
Sensorineural hearing loss
Conductive hearing loss
Pure tone audiogram
Sensorineural hearing loss
Conductive hearing loss
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
This pure tone audiogram is recorded from a 12
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
This pure tone audiogram is recorded from a 12
Tinnitus
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Exact cause is unknown but is though to be
Tinnitus
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Exact cause is unknown but is though to be
Tinnitus
Subjective Tinnitus
Otologic
Presbycusis
Noise-induced hearing loss
Otitis media with effusion
Menière’s disease
Otosclerosis
Cerumen
Foreign body against
Tinnitus
Subjective Tinnitus
Otologic
Presbycusis
Noise-induced hearing loss
Otitis media with effusion
Menière’s disease
Otosclerosis
Cerumen
Foreign body against
Tinnitus
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Holistic approach (options)
Mainly based on acoustic de-sensitisation:
• Relaxation techniques
•
Tinnitus
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Holistic approach (options)
Mainly based on acoustic de-sensitisation:
• Relaxation techniques
•
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
You review a 70-year-old woman who is on multiple
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
You review a 70-year-old woman who is on multiple
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Benign paroxysmal positional vertigo
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Acute vertigo that is induced by
Benign paroxysmal positional vertigo
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Acute vertigo that is induced by
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
A 52-year-old woman presents with dizziness and vertigo when
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
A 52-year-old woman presents with dizziness and vertigo when
Vestibular neuritis
Second most common disorder affecting the labyrinth
Viral etiology with consequent
Vestibular neuritis
Second most common disorder affecting the labyrinth
Viral etiology with consequent
Vestibular neuritis
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Treatment:
Bed rest, vestibular sedatives and anti-emetics in the
Vestibular neuritis
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Treatment:
Bed rest, vestibular sedatives and anti-emetics in the
Meniere’s disease
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
It is commonest in the 30–50 years age
Meniere’s disease
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
It is commonest in the 30–50 years age
Meniere disease
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
DxT vertigo + vomiting + tinnitus + sensorineural
Meniere disease
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
DxT vertigo + vomiting + tinnitus + sensorineural
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
An elderly patient has acute onset unilateral deafness, tinnitis
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
An elderly patient has acute onset unilateral deafness, tinnitis
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
A 39-year-old woman arrives at the hospital after her
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
A 39-year-old woman arrives at the hospital after her
Acoustic neuroma (vestibular schwannomas)
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Benign tumour of Schwann cells surrounding
Acoustic neuroma (vestibular schwannomas)
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Benign tumour of Schwann cells surrounding
Acoustic neuroma
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Diagnosis: audiometry (SNHL), MRI, CT
Treatment:
Conservative: monitoring
Surgical resection
Translabyrinthine, middle
Acoustic neuroma
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Diagnosis: audiometry (SNHL), MRI, CT
Treatment:
Conservative: monitoring
Surgical resection
Translabyrinthine, middle
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Which of the following is least likely to cause
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Which of the following is least likely to cause
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Otosclerosis
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Disease of the bone surrounding the inner ear and
Otosclerosis
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Disease of the bone surrounding the inner ear and
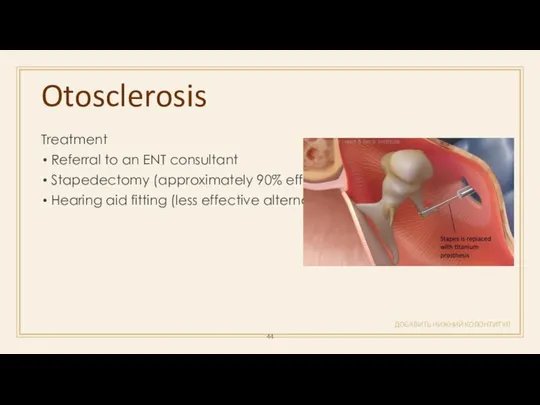
Otosclerosis
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Treatment
Referral to an ENT consultant
Stapedectomy (approximately 90% effective)
Hearing aid
Otosclerosis
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Treatment
Referral to an ENT consultant
Stapedectomy (approximately 90% effective)
Hearing aid
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Which of the following is most likely to be
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Which of the following is most likely to be

ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
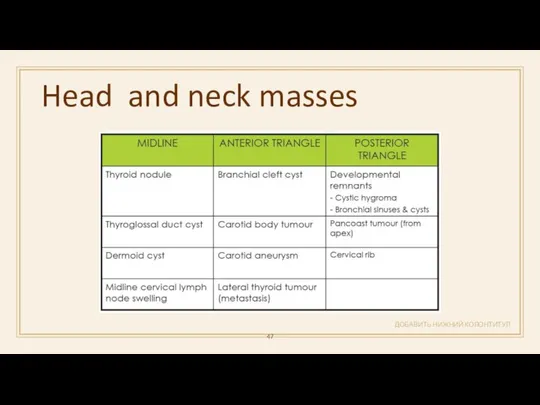
Head and neck masses
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Head and neck masses
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
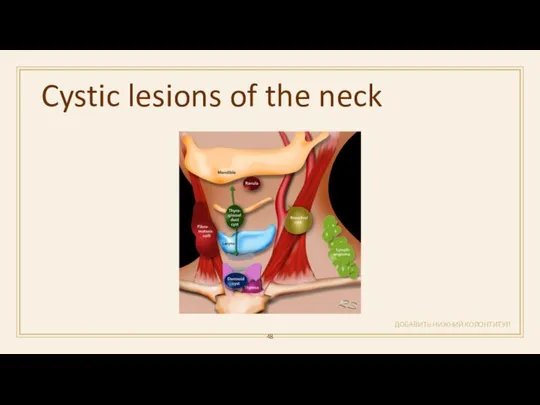
Cystic lesions of the neck
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Cystic lesions of the neck
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Cystic hygroma
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Commonly involves the posterior cervical space
May be
Cystic hygroma
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Commonly involves the posterior cervical space
May be
Branchial deft cyst
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
located inferior to the external auditory meatus
Branchial deft cyst
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
located inferior to the external auditory meatus
Thyroglossal duct cyst
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
the most common childhood midline neck swelling
It
Thyroglossal duct cyst
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
the most common childhood midline neck swelling
It
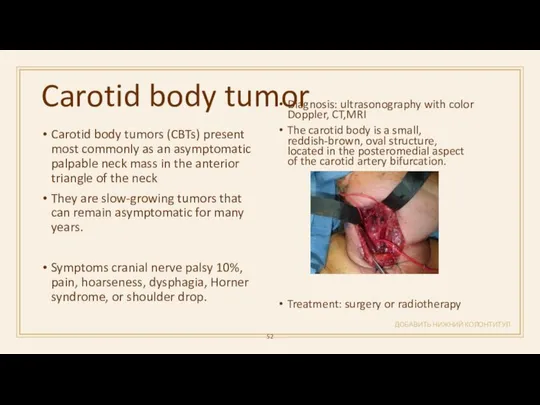
Carotid body tumor
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Carotid body tumors (CBTs) present most commonly
Carotid body tumor
ДОБАВИТЬ НИЖНИЙ КОЛОНТИТУЛ
Carotid body tumors (CBTs) present most commonly
 Вирусология - наука изменившая жизнь
Вирусология - наука изменившая жизнь Uşaqlığın mioması
Uşaqlığın mioması Переломы и вывихи
Переломы и вывихи Фетоплаценталық жүйенің физиологиясы мен патологиясы
Фетоплаценталық жүйенің физиологиясы мен патологиясы Өкпе қатерлі ісігі
Өкпе қатерлі ісігі Дифтерия. Инфекционные заболевания у детей
Дифтерия. Инфекционные заболевания у детей худойдотов 2
худойдотов 2 Патология иммунной системы. Иммунодефицит
Патология иммунной системы. Иммунодефицит Организация трансфузионной помощи. Донорство
Организация трансфузионной помощи. Донорство Применение металлоконструкций и биодеградируемых материалов при переломах дистального отдела плечевой кости у детей
Применение металлоконструкций и биодеградируемых материалов при переломах дистального отдела плечевой кости у детей Обов’язковий склад інструкції до лікарських препаратів
Обов’язковий склад інструкції до лікарських препаратів Жедел бүйрек жетіспеушілігінің клиникалық көріністері
Жедел бүйрек жетіспеушілігінің клиникалық көріністері Медицинская помощь больным с менингитами на госпитальном этапе
Медицинская помощь больным с менингитами на госпитальном этапе TRALI. Минимизация риска
TRALI. Минимизация риска Гистология
Гистология Доказательная профилактика. Основные виды, проблемы внедрения и анализа результатов скрининговых программ
Доказательная профилактика. Основные виды, проблемы внедрения и анализа результатов скрининговых программ Кровотечі, їх класифікація. Перша допомога при кровотечах
Кровотечі, їх класифікація. Перша допомога при кровотечах Метод использования виртуальной реальности у детей с синдромом гипермобильности суставов
Метод использования виртуальной реальности у детей с синдромом гипермобильности суставов Туберкулинодиагностика
Туберкулинодиагностика Расстройства интеллекта
Расстройства интеллекта Гериатрическая фармакотерапия
Гериатрическая фармакотерапия Дополнительные методы обследования в клинике ортопедической стоматологии. Диагноз, дифференциальный диагноз
Дополнительные методы обследования в клинике ортопедической стоматологии. Диагноз, дифференциальный диагноз Рак предстательной железы
Рак предстательной железы Секреты правильного питания. Овощи и фрукты – полезные продукты
Секреты правильного питания. Овощи и фрукты – полезные продукты Механическая асфиксия
Механическая асфиксия Генитальный пролапс у женщин с дисплазией соединительной ткани
Генитальный пролапс у женщин с дисплазией соединительной ткани Статус участника проекта Сколково
Статус участника проекта Сколково Организация работы специализированных (БИТ) и линейных бригад скорой помощи
Организация работы специализированных (БИТ) и линейных бригад скорой помощи