- Puerperal Sepsis

Содержание
- 2. An infection of the genital tract which occurs as a complication of delivery is termed puerperal
- 3. Predisposing factors of puerperal sepsis: The pathogenicity of the vaginal flora may be influenced by certain
- 4. Antepartum risk factors: (1) Malnutrition and anemia, (2) Preterm labor, (3) Premature rupture of the membranes,
- 5. Microorganisms responsible for puerperal sepsis and the major pathology; Aerobic—Group A beta-hemolytic Streptococcus (GAS)—Toxic shock
- 6. Mode of Infection: Puerperal sepsis is essentially a wound infection. Placental site (being a raw surface),
- 7. PATHOGENESIS Endometrium (placental implantation site), cervical lacerated wound, vaginal wound or perineal lacerated wound are the
- 8. Clinical Features Local infection Uterine infection Spreading infection Local infection (Wound infection): (1)
- 9. Spreading infection (extrauterine spread) is evident by presence of pelvic tenderness (pelvic peritonitis), tenderness on the
- 10. Investigation of Puerperal Pyrexia The underlying principles in investigations are: To locate the site of infection,
- 11. Investigations include: High vaginal and endocervical swabs for culture in aerobic and anaerobic media and sensitivity
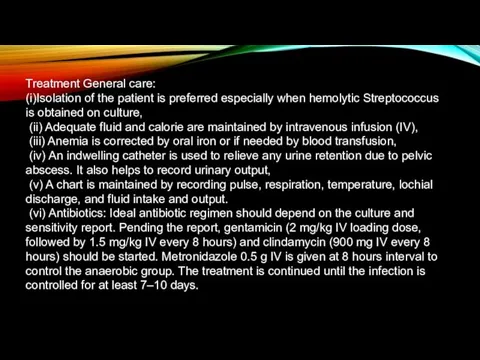
- 12. Treatment General care: (i)Isolation of the patient is preferred especially when hemolytic Streptococcus is obtained on
- 13. Surgical treatment: There is little role of major surgery in the treatment of puerperal sepsis.
- 15. Скачать презентацию
An infection of the genital tract which occurs as a
An infection of the genital tract which occurs as a
Predisposing factors of puerperal sepsis:
The pathogenicity of the vaginal flora
Predisposing factors of puerperal sepsis:
The pathogenicity of the vaginal flora
Antepartum risk factors: (1) Malnutrition and anemia, (2) Preterm labor, (3)
Antepartum risk factors: (1) Malnutrition and anemia, (2) Preterm labor, (3)

Microorganisms responsible for puerperal sepsis and the major pathology;
Aerobic—Group
Microorganisms responsible for puerperal sepsis and the major pathology;
Aerobic—Group
Mode of Infection:
Puerperal sepsis is essentially a wound infection. Placental
Mode of Infection:
Puerperal sepsis is essentially a wound infection. Placental
PATHOGENESIS Endometrium (placental implantation site), cervical lacerated wound, vaginal wound or
PATHOGENESIS Endometrium (placental implantation site), cervical lacerated wound, vaginal wound or

Clinical Features
Local infection
Uterine infection
Spreading infection
Clinical Features
Local infection
Uterine infection
Spreading infection
Spreading infection (extrauterine spread) is evident by presence of pelvic tenderness
Spreading infection (extrauterine spread) is evident by presence of pelvic tenderness
Investigation of Puerperal Pyrexia The underlying principles in investigations are:
To
Investigation of Puerperal Pyrexia The underlying principles in investigations are:
To
Investigations include:
High vaginal and endocervical swabs for culture in aerobic
Investigations include:
High vaginal and endocervical swabs for culture in aerobic
Treatment General care:
(i)Isolation of the patient is preferred especially when hemolytic
Treatment General care:
(i)Isolation of the patient is preferred especially when hemolytic
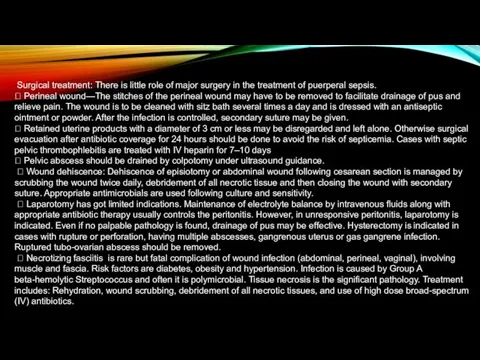
Surgical treatment: There is little role of major surgery in
Surgical treatment: There is little role of major surgery in
 Микроклимат сипаттамасы
Микроклимат сипаттамасы Использование виртуальной реальности у детей с нарушениями осанки при синдроме гипермобильности суставов
Использование виртуальной реальности у детей с нарушениями осанки при синдроме гипермобильности суставов Комплексное обследование при дислалии. Лекция 2
Комплексное обследование при дислалии. Лекция 2 Аффективные расстройства
Аффективные расстройства Хронический гастрит. Язвенная болезнь
Хронический гастрит. Язвенная болезнь Коррекционный маршрут в дооперационный период ребенка с открытой ринолалией
Коррекционный маршрут в дооперационный период ребенка с открытой ринолалией Лучевая диагностика заболеваний сердечно-сосудистой системы
Лучевая диагностика заболеваний сердечно-сосудистой системы Психологические условия полноценного психофизической развития ребенка в период новорождённости
Психологические условия полноценного психофизической развития ребенка в период новорождённости Психомоторное развитие ребенка и его оценка. Теории психического и духовного развития. Поведение детей
Психомоторное развитие ребенка и его оценка. Теории психического и духовного развития. Поведение детей Душевное здоровье детей и подростков: неврозы и неврозоподобные расстройства
Душевное здоровье детей и подростков: неврозы и неврозоподобные расстройства Черепно-мозговая травма. Основные патологические процессы
Черепно-мозговая травма. Основные патологические процессы Проблема ВИЧ/СПИД в Забайкальском крае
Проблема ВИЧ/СПИД в Забайкальском крае Ожирение
Ожирение Общая семиотика моногенных и многофакторных болезней
Общая семиотика моногенных и многофакторных болезней Жизнь современного ребенка. Интенсивный рост. Школьные нагрузки. Стрессы
Жизнь современного ребенка. Интенсивный рост. Школьные нагрузки. Стрессы Особенности гигиены полости рта у пациентов с несъемными ортопедическими конструкциями и дентальными имплантатами
Особенности гигиены полости рта у пациентов с несъемными ортопедическими конструкциями и дентальными имплантатами Гигиена лечебно-профилактических учреждений
Гигиена лечебно-профилактических учреждений Острый холецистит – неспецифическое воспаление желчного пузыря
Острый холецистит – неспецифическое воспаление желчного пузыря Мотивация теориясы. Мотивация процесі
Мотивация теориясы. Мотивация процесі Биохимия печени
Биохимия печени Акушерлік іс және гинекология
Акушерлік іс және гинекология Остеоартрит, остеоартроз. Новый взгляд на старую проблему
Остеоартрит, остеоартроз. Новый взгляд на старую проблему Неспецифический язвенный колит и болезнь Крона
Неспецифический язвенный колит и болезнь Крона Гигиена полости рта
Гигиена полости рта Бір жасқа дейінгі дені сау балалардың диспансерлік бақылау, патронаж
Бір жасқа дейінгі дені сау балалардың диспансерлік бақылау, патронаж Sweet proteins
Sweet proteins Фізична реабілітація дітей з рахітом
Фізична реабілітація дітей з рахітом Трансанальная слизисто-подслизистая резекция по методу Лонго
Трансанальная слизисто-подслизистая резекция по методу Лонго