- Rheumatic Fever

Содержание
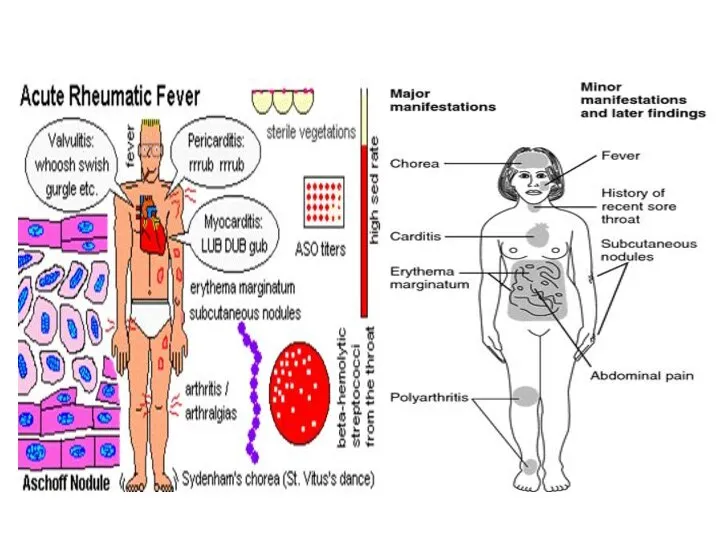
- 2. Rheumatic fever is an inflammatory disease involving the joints, the heart, the CNS, the skin and
- 3. Etiology Non-suppurative complications of upper respiratory infections by group A-β hemolytic streptococcal (GAS) Skin infections by
- 4. Pathogenesis *Autoimmune theory, abnormal immune response by human host to some component of GAS. * The
- 5. Epidemiology Rheumatic fever occurs at all ages peaks between 5-15 ys A high incidence in tropical
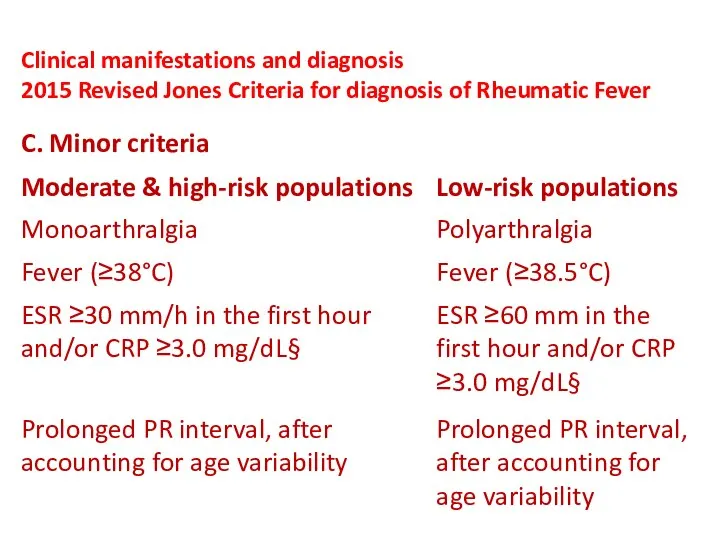
- 6. Epidemiology Low-Risk populations: Those with incidence ≤2 per 100,000 school-age children per year or all-age rheumatic
- 7. Epidemiology High-Risk populations: Those with incidence >2 per 100,000 school-age children per year or all-age rheumatic
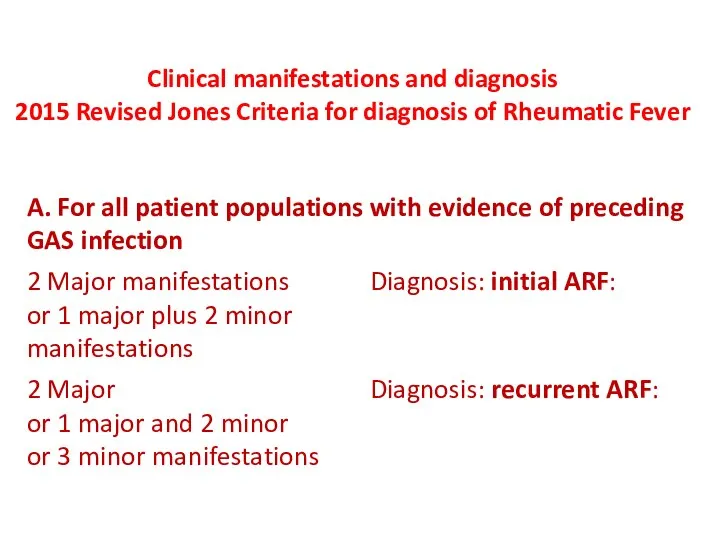
- 8. Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever
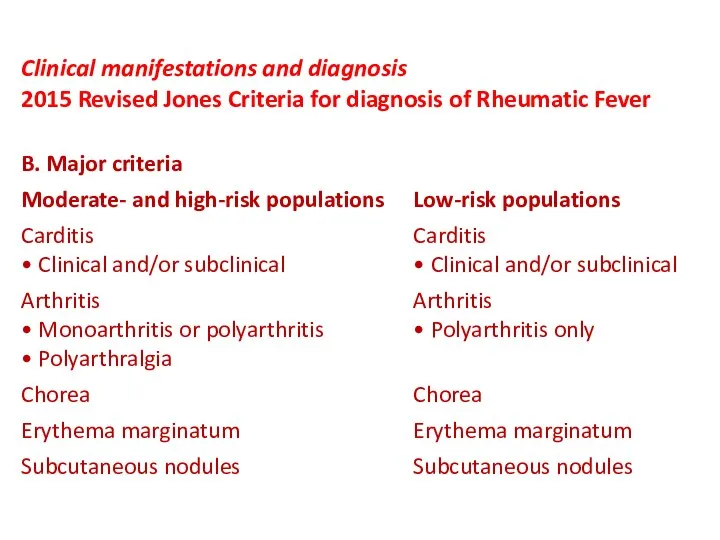
- 9. Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever
- 10. Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever
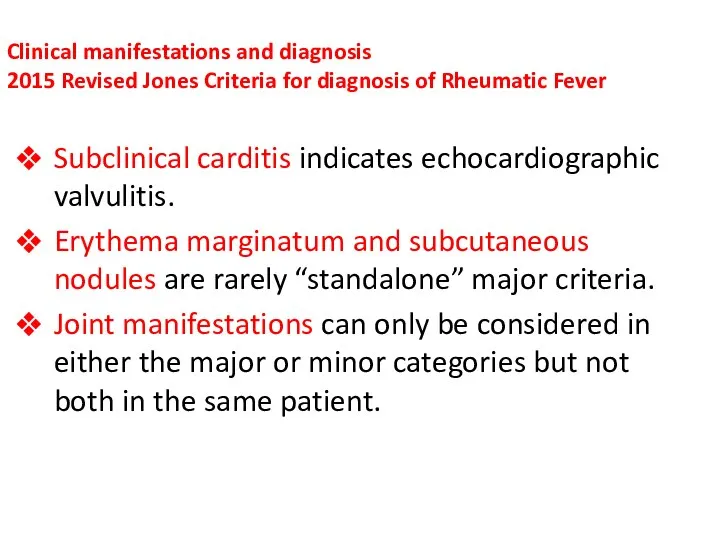
- 11. Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever Subclinical carditis indicates
- 12. Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever
- 13. Clinical manifestations and diagnosis: 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever
- 14. Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever CRP value must
- 15. Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever Prolonged P-R interval
- 16. Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever
- 17. Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic Fever
- 18. Guidelines for the diagnosis of initial or recurrent attack of RF Revised Jones criteria, Updated 2015
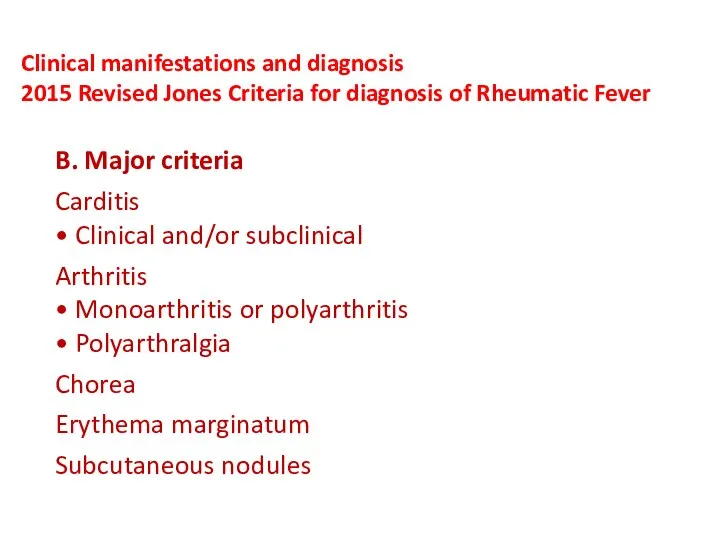
- 20. Major Jones criteria
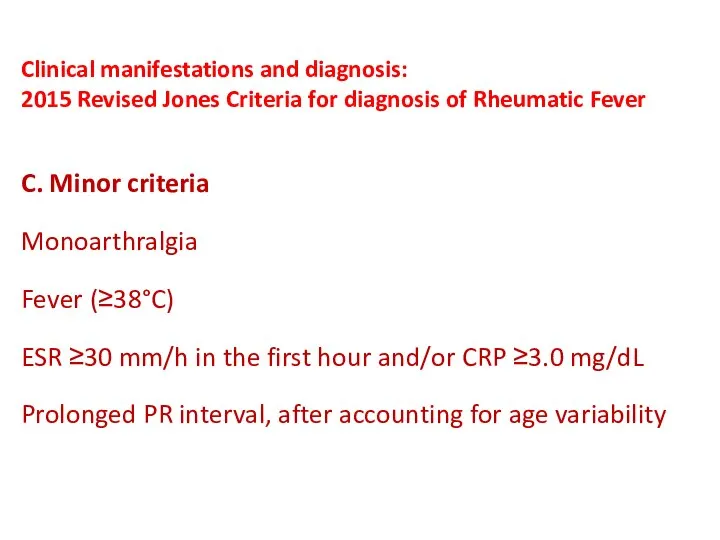
- 21. Minor Jones criteria
- 22. Rheumatic Carditis Most serious manifestations of ARF Occurs in about 50-60% of all cases of ARF
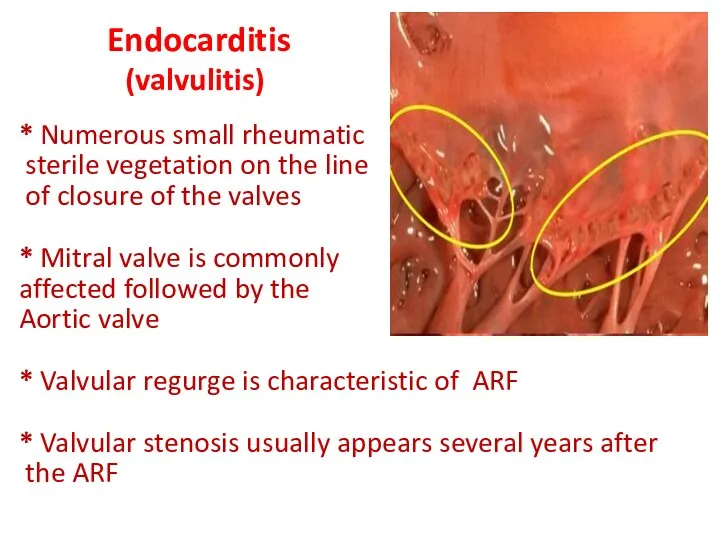
- 23. Endocarditis (valvulitis) * Numerous small rheumatic sterile vegetation on the line of closure of the valves
- 24. Murmurs in patients with endocarditis soft - musical - not associated with thrill 1- Apical pansystolic
- 25. Myocarditis Cardiac dilatation Congestive heart failure Tachycardia disproportionate to fever Arrhythmias Muffled Heart sounds
- 26. Pericarditis Dry pericarditis precordial pain and friction rub Wet Pericarditis mild to moderate effusion
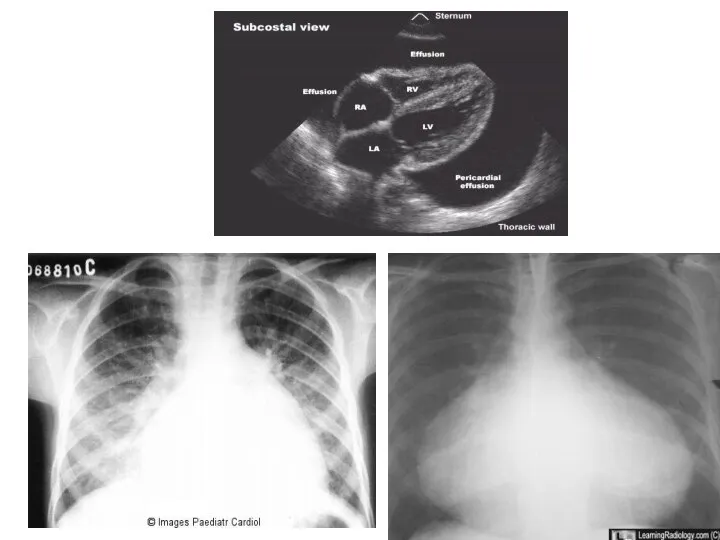
- 27. Pericarditis with massive pericardial effusion: Weak pulse. Pulsus paradoxus is an abnormally large decrease in systolic
- 29. DD of rheumatic carditis: Other causes of myocarditis such as viral myocarditis. Other causes of pericarditis.
- 30. Treatment of carditis * Mild cases without HF or cardiomegaly Salicylates 50-70mg/kg/day orally after meal divided
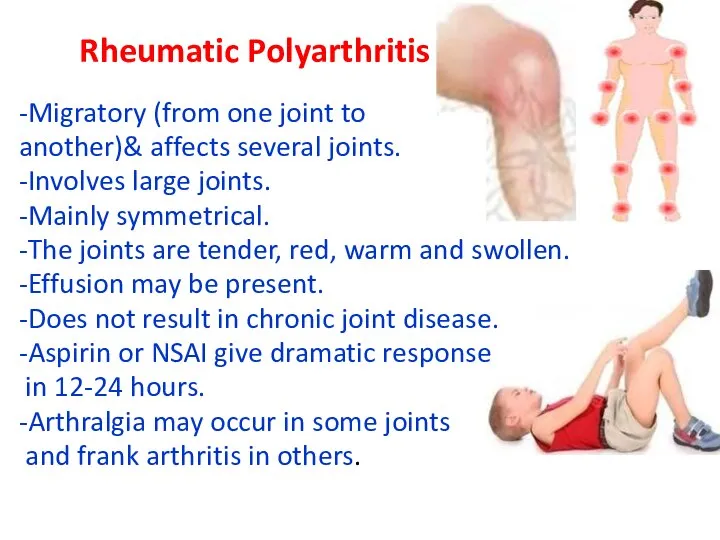
- 31. Rheumatic Polyarthritis -Migratory (from one joint to another)& affects several joints. -Involves large joints. -Mainly symmetrical.
- 32. Differential diagnosis: Other causes of arthritis - Juvenile rheumatoid arthritis & other collagen diseases. - Infective
- 33. Treatment of arthritis Salicylates 50-70mg/kg/day orally after meal divided into 4 doses for 3-5 days, then
- 34. Rheumatic Chorea (Sydenham chorea) Has long latent period (2-6 months), the onset is usually insidious. May
- 35. Clinical manifestation: - Characterized by involuntary movements, emotional liability & hypotonia. - Purposeless, irregular, rapid, jerking
- 36. Sydenhams chorea watch please
- 37. Clinical tests for detection of chorea Marked fluctuation in muscle tone (felt by asking the patient
- 38. In pure chorea the ESR and ASOT are normal. This is attributed to the long latent
- 39. Prognosis Chorea is a self limited condition. Mild cases subside within few weeks - 3 months
- 40. Treatment of rheumatic chorea - Anti inflamatory - Phenobarbital - Haloperidol - Chlorpromazine
- 41. Subcutaneous nodules Bilaterally symmetrical firm nodules varying in diameter from few millimeters to centimeter. Movable painless
- 42. Erythema marginatum Red, raised, non pruritic macules extend to form wavy lines or rings with pale
- 43. Complications of Acute Rheumatic fever Chronic valvular heart disease (RHD) after an attack of rheumatic carditis.
- 44. Prevention of rheumatic fever can be divided into three approaches General measures Primary prevention Secondary orevention
- 45. 1. Treatment (eradication ) of GAS infection Treatment of streptococcal upper respiratory tract infection must be
- 46. Primary prevention eradication of GAS all patients with ARF should receive
- 47. Secondary prevention (for recurrences of acute rheumatic fever)
- 48. Duration of Secondary prevention
- 50. Скачать презентацию
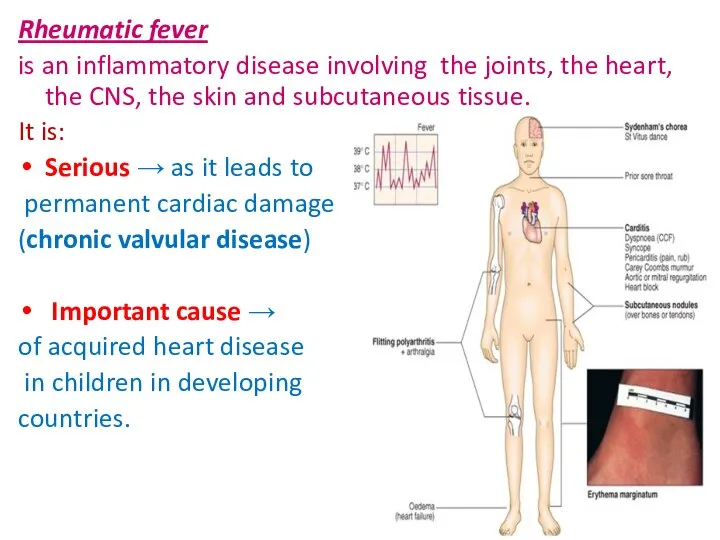
Rheumatic fever
is an inflammatory disease involving the joints, the
Rheumatic fever
is an inflammatory disease involving the joints, the
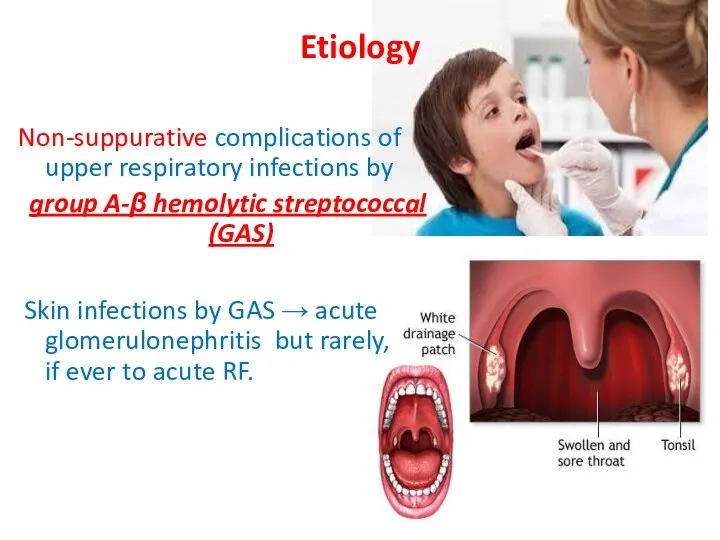
Etiology
Non-suppurative complications of upper respiratory infections by
group A-β hemolytic
Etiology
Non-suppurative complications of upper respiratory infections by
group A-β hemolytic
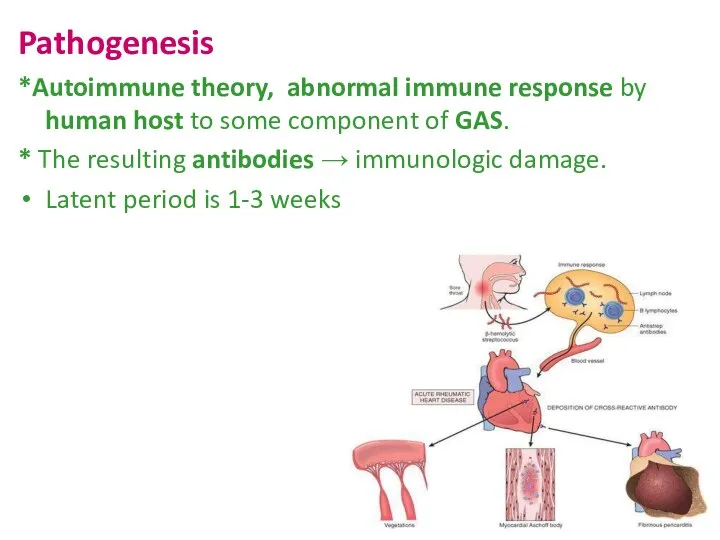
Pathogenesis
*Autoimmune theory, abnormal immune response by human host to some component
Pathogenesis
*Autoimmune theory, abnormal immune response by human host to some component
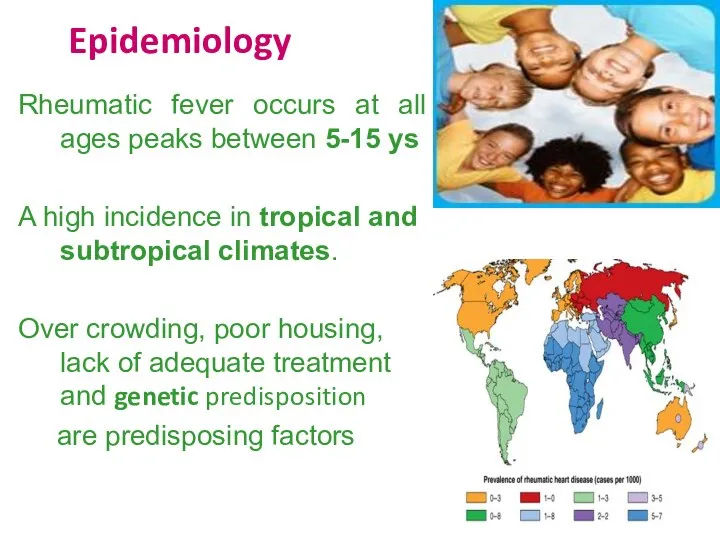
Epidemiology
Rheumatic fever occurs at all ages peaks between 5-15 ys
A
Epidemiology
Rheumatic fever occurs at all ages peaks between 5-15 ys
A
Epidemiology
Low-Risk populations:
Those with incidence ≤2 per 100,000 school-age children per
Epidemiology
Low-Risk populations:
Those with incidence ≤2 per 100,000 school-age children per
Epidemiology
High-Risk populations:
Those with incidence >2 per 100,000 school-age children per
Epidemiology
High-Risk populations:
Those with incidence >2 per 100,000 school-age children per
Clinical manifestations and diagnosis
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis:
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis: 2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis
2015 Revised Jones Criteria for diagnosis of Rheumatic
Clinical manifestations and diagnosis 2015 Revised Jones Criteria for diagnosis of Rheumatic
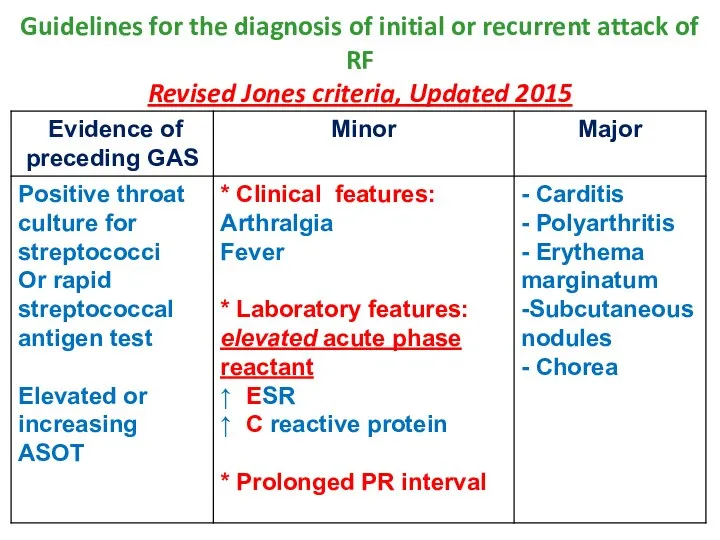
Guidelines for the diagnosis of initial or recurrent attack of RF
Guidelines for the diagnosis of initial or recurrent attack of RF
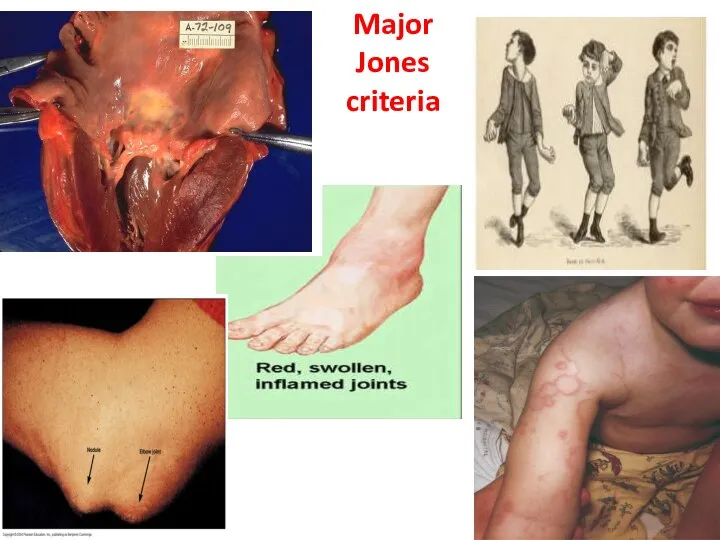
Major
Jones
criteria
Major
Jones
criteria
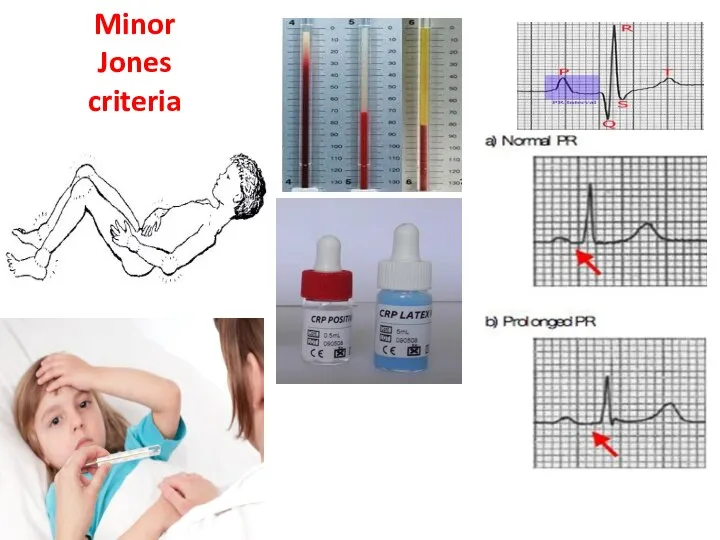
Minor
Jones
criteria
Minor
Jones
criteria
Rheumatic Carditis
Most serious manifestations of ARF
Occurs in about 50-60% of all
Most serious manifestations of ARF
Occurs in about 50-60% of all
Endocarditis
(valvulitis)
* Numerous small rheumatic
sterile vegetation on the line
Endocarditis
(valvulitis)
* Numerous small rheumatic
sterile vegetation on the line
Murmurs in patients with endocarditis
soft - musical - not associated with
soft - musical - not associated with
Myocarditis
Cardiac dilatation
Congestive heart failure
Tachycardia disproportionate to fever
Arrhythmias
Muffled Heart sounds
Myocarditis
Cardiac dilatation
Congestive heart failure
Tachycardia disproportionate to fever
Arrhythmias
Muffled Heart sounds
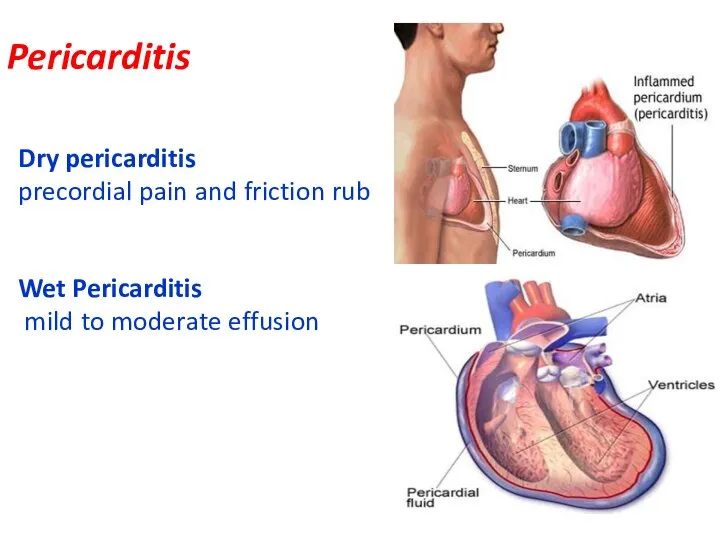
Pericarditis
Dry pericarditis
precordial pain and friction rub
Wet Pericarditis
mild to moderate
Pericarditis
Dry pericarditis
precordial pain and friction rub
Wet Pericarditis
mild to moderate
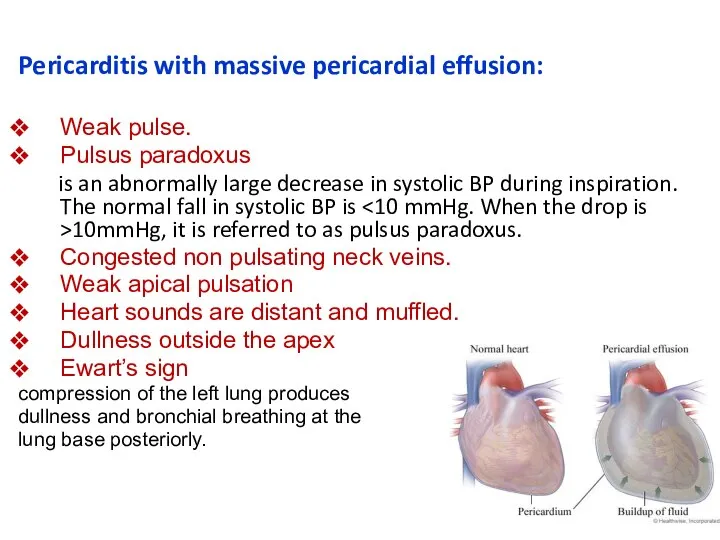
Pericarditis with massive pericardial effusion:
Weak pulse.
Pulsus paradoxus
is an abnormally large
Weak pulse.
Pulsus paradoxus
is an abnormally large
DD of rheumatic carditis:
Other causes of myocarditis such as viral myocarditis.
Other
Other causes of myocarditis such as viral myocarditis.
Other
Treatment of carditis
* Mild cases without HF or cardiomegaly
Salicylates
Treatment of carditis
* Mild cases without HF or cardiomegaly
Salicylates
Rheumatic Polyarthritis
-Migratory (from one joint to
another)& affects several joints.
-Involves large
Rheumatic Polyarthritis
-Migratory (from one joint to
another)& affects several joints.
-Involves large
Differential diagnosis:
Other causes of arthritis
- Juvenile rheumatoid arthritis & other collagen
Differential diagnosis:
Other causes of arthritis
- Juvenile rheumatoid arthritis & other collagen
Treatment of arthritis
Salicylates 50-70mg/kg/day orally after meal divided into
Treatment of arthritis
Salicylates 50-70mg/kg/day orally after meal divided into
Rheumatic Chorea
(Sydenham chorea)
Has long latent period (2-6 months), the
Rheumatic Chorea
(Sydenham chorea)
Has long latent period (2-6 months), the
Clinical manifestation:
- Characterized by involuntary movements, emotional liability & hypotonia.
-
Clinical manifestation:
- Characterized by involuntary movements, emotional liability & hypotonia.
-
Sydenhams chorea
watch please
Sydenhams chorea
watch please
Clinical tests for detection of chorea
Marked fluctuation in muscle tone
Clinical tests for detection of chorea
Marked fluctuation in muscle tone
In pure chorea the ESR and ASOT are normal. This is
In pure chorea the ESR and ASOT are normal. This is
Prognosis
Chorea is a self limited condition.
Mild cases subside within few weeks
Prognosis
Chorea is a self limited condition.
Mild cases subside within few weeks
Treatment of rheumatic chorea
- Anti inflamatory
- Phenobarbital
-
Treatment of rheumatic chorea
- Anti inflamatory
- Phenobarbital
-
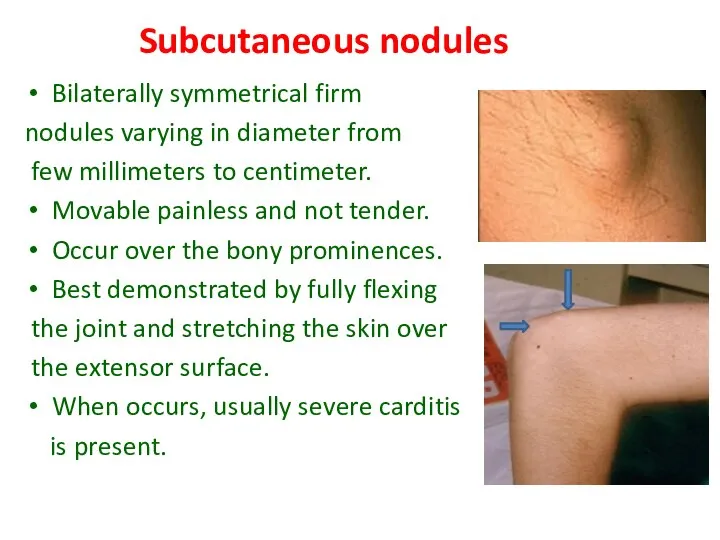
Subcutaneous nodules
Bilaterally symmetrical firm
nodules varying in diameter from
Subcutaneous nodules
Bilaterally symmetrical firm
nodules varying in diameter from
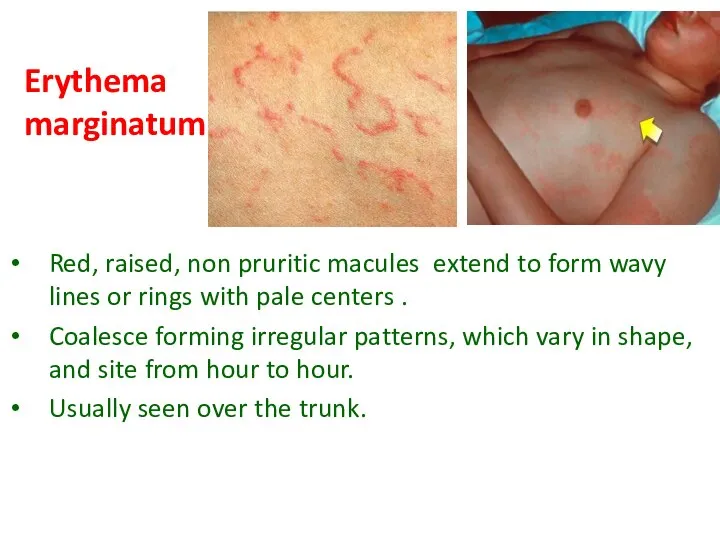
Erythema marginatum
Red, raised, non pruritic macules extend to form wavy lines
Erythema marginatum
Red, raised, non pruritic macules extend to form wavy lines
Complications of Acute Rheumatic fever
Chronic valvular heart disease (RHD) after
Complications of Acute Rheumatic fever
Chronic valvular heart disease (RHD) after
Prevention of rheumatic fever
can be divided into three approaches
General measures
Primary prevention
Secondary
Prevention of rheumatic fever
can be divided into three approaches
General measures
Primary prevention
Secondary
1. Treatment (eradication ) of GAS infection
Treatment of streptococcal upper respiratory
1. Treatment (eradication ) of GAS infection
Treatment of streptococcal upper respiratory
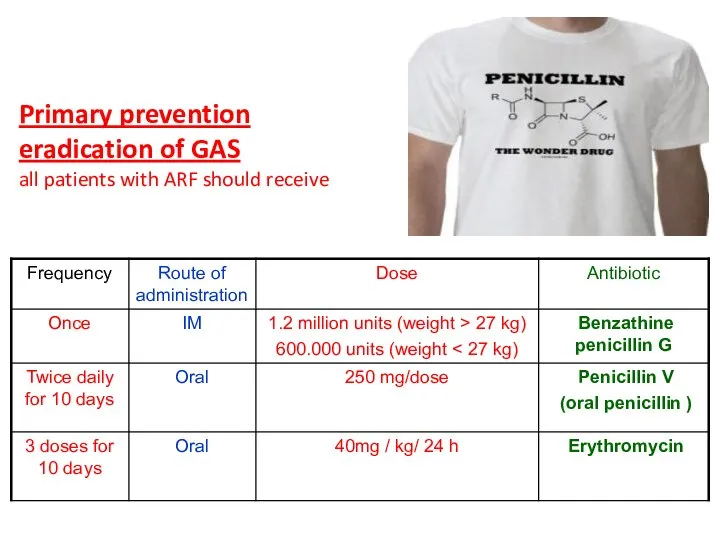
Primary prevention
eradication of GAS
all patients with ARF should receive
Primary prevention
eradication of GAS
all patients with ARF should receive
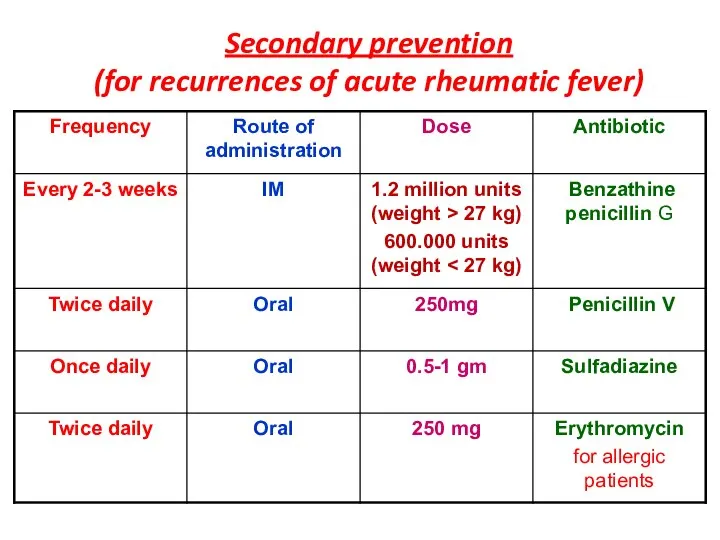
Secondary prevention
(for recurrences of acute rheumatic fever)
Secondary prevention
(for recurrences of acute rheumatic fever)
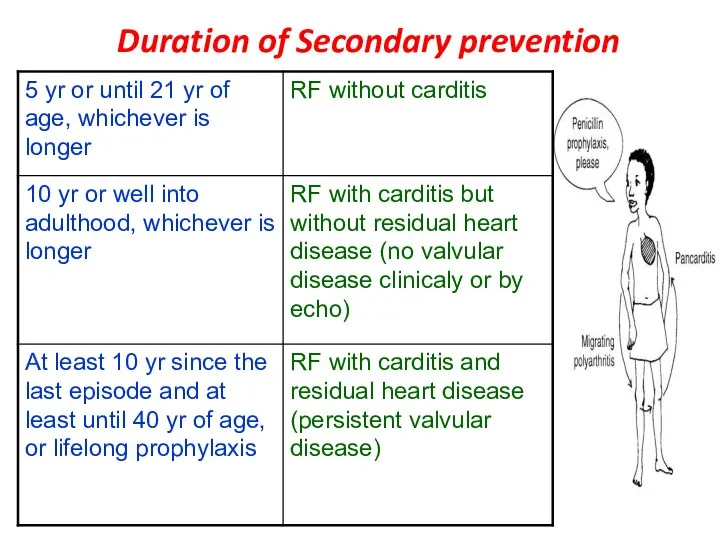
Duration of Secondary prevention
Duration of Secondary prevention
 COVID–19 и животные компаньоны
COVID–19 и животные компаньоны Методы изучения генетики человека
Методы изучения генетики человека Портальная гипертензия
Портальная гипертензия Вас приветствует Калининград!
Вас приветствует Калининград! Микробиологическая диагностика столбняка
Микробиологическая диагностика столбняка Диагностическое значение онкомаркеров в ранней диагностике рака
Диагностическое значение онкомаркеров в ранней диагностике рака Азбука здорового питания
Азбука здорового питания Стоматологическое просвещение. Методы оценки эффективности стоматологического просвещения
Стоматологическое просвещение. Методы оценки эффективности стоматологического просвещения Основні клінічні синдроми та їх клінічне значення в діагностиці захворювань дитячого віку
Основні клінічні синдроми та їх клінічне значення в діагностиці захворювань дитячого віку Факторы риска развития артериальной гипертензии
Факторы риска развития артериальной гипертензии Болезни органов дыхания
Болезни органов дыхания Жүректің туа пайда болған ақауының алдын алуда поливитаминдердің тиімділігін бағалау
Жүректің туа пайда болған ақауының алдын алуда поливитаминдердің тиімділігін бағалау Рекомендации ЕОК по ведению пациентов с острым коронарным синдромом с подъёмом сегмента ST
Рекомендации ЕОК по ведению пациентов с острым коронарным синдромом с подъёмом сегмента ST Психология, патопсихология и психопатология эмоционально - волевой сферы
Психология, патопсихология и психопатология эмоционально - волевой сферы Некомпактный миокард левого желудочка в педиатрической практике
Некомпактный миокард левого желудочка в педиатрической практике Прикладная эстетика. Applied aesthetics
Прикладная эстетика. Applied aesthetics Омыртқа жотасының зақымдануы
Омыртқа жотасының зақымдануы Болезнь Паркинсона. Современные методы лечения
Болезнь Паркинсона. Современные методы лечения КГП на ПХВ Больница района Аққулы Представление на ЦВКК
КГП на ПХВ Больница района Аққулы Представление на ЦВКК Неонатальный период. Доношенный новорожденный. Тема 3
Неонатальный период. Доношенный новорожденный. Тема 3 Скорая помощь для кожи и волос: серия средств со змеиным жиром
Скорая помощь для кожи и волос: серия средств со змеиным жиром Созылмалы өкпелік жүрек
Созылмалы өкпелік жүрек Опыт лечения синдромов множественной эндокринной неоплазии
Опыт лечения синдромов множественной эндокринной неоплазии ÐÑиÑ
иаÑÑиÑ_2.РаÑÑÑÑойÑÑва воÑпÑиÑÑиÑ
ÐÑиÑ
иаÑÑиÑ_2.РаÑÑÑÑойÑÑва воÑпÑиÑÑиÑ Рентген диагностика заболеваний молочной железы
Рентген диагностика заболеваний молочной железы Морфология, структура, окраска бактерий
Морфология, структура, окраска бактерий Методы исследования и синдромы патологии эндокринных органов
Методы исследования и синдромы патологии эндокринных органов Организация службы скорой медицинской помощи населению
Организация службы скорой медицинской помощи населению