- Chronic Rheumatic Heart Disease

Содержание
- 2. The diagnosis of heart disease must be * Etiological: → (Congenital - Rheumatic) * Anatomical: →
- 3. Occurs in severe cardiac involvement during initial or recurrent attacks of ARF Left - sided heart
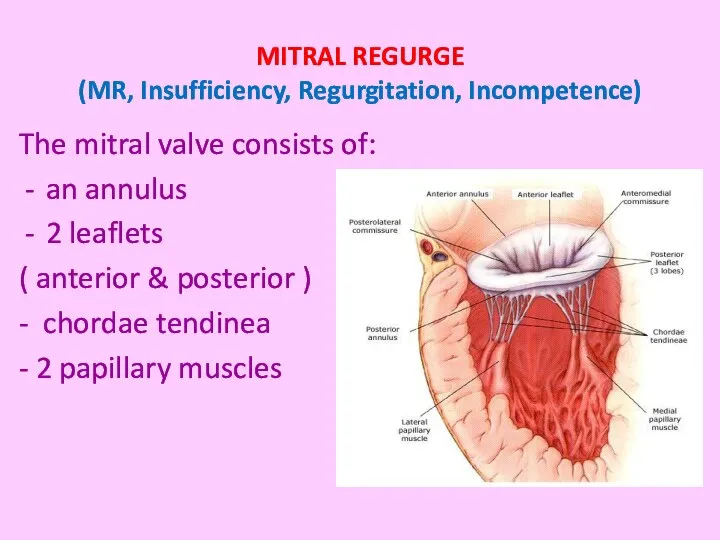
- 4. MITRAL REGURGE (MR, Insufficiency, Regurgitation, Incompetence) The mitral valve consists of: an annulus 2 leaflets (
- 5. Healing of ARF results in Fibrosis & contracture of leaflets Shortening & thickening of chordea tendinea.
- 6. Mild MR → no symptoms Severe MR → Symptoms of HF, pulmonary congestion, pulmonary edema dyspnea
- 7. Signs: Apex → (LV apex), shifted downward, localized, forcible, hyperdynamic (ill sustained) with systolic thrill. S1
- 8. Mitral regurge CXR Mitral regurge Echocardiography
- 9. 1- VSD: -maximal intensity over the 3rd & 4th left intercostal spaces -propagated in fan manner
- 10. Prophylaxis → Against rheumatic recurrences (LONG ACTING PENECILLIN) → Against infective endocarditis Medical treatment of heart
- 11. MITRAL STENOSIS (MS) Pathophysiology -Thickening of valve leaflets - Fusion of commissures - Shortening & thickening
- 12. The clinical course depends on the severity of MS. Symptoms: Dyspnea on exertion. Orthopnea & paroxysmal
- 13. Signs Signs of RV hypertrophy: a- The apex is diffuse and shifted outward (RV apex), diastolic
- 14. Mitral stenosis CXR Mitral stenosis echo
- 15. Mitral flow murmur (functional MS) associated with large VSD, PDA, MR, AR (Austin flint murmur) -
- 16. Prophylaxis → Against rheumatic recurrences (LONG ACTING PENECILLIN) → Against infective endocarditis Medical treatment: Heart failure
- 17. Combined MS and MR Dilatation, scaring and narrowing → stenosis & leakage Obstruction and leakage of
- 18. Which of the following pathological change occur in rheumatic mitral stenosis ? Increased left atrial pressure
- 19. Rheumatic AR is the result of fibrosis and contracture of the aortic valve structure Hemodynamically AR
- 20. Symptoms Depend on the severity. In moderate and severe cases: Effort intolerance, palpitation, dyspnea, orthopnea &
- 21. The rapid run off of the blood from aorta during diastole causes the signs of hyperdynamic
- 22. * Manifestations of LV enlargement. The apex is shifted downword, forcible, localized and hyperdynamic (ill sustained)
- 23. Aortic regurge CXR Aortic regurge Echocardiography
- 24. Prophylaxis → Against rheumatic recurrences (LONG ACTING PENECILLIN) → Against infective endocarditis Surgery: Aortic valve replacement.
- 25. AORTIC STENOSIS - Commissural adhesions occur slowly and progressive → narrowing and calcification of the orifice
- 26. In cases with severe stenosis: Chest pain, exercise intolerance, dyspnea, syncope. Clinical manifestations: Symptoms:
- 27. - The apex: Localized, forceful & sustained (pressure overload). - Systolic thrill is common on Rt
- 28. Aortic stenosis CXR Aortic stenosis Echocardiography shows morphology of the valve and degree of stenosis.
- 29. → Against rheumatic recurrences (LONG ACTING PENECILLIN) → Against infective endocarditis Surgical intervention by valve replacement.
- 30. A case with dilated left ventricle and normal size of the other chamber. The most likely
- 32. Скачать презентацию
The diagnosis of heart disease must be
* Etiological: → (Congenital -
The diagnosis of heart disease must be
* Etiological: → (Congenital -
Occurs in severe cardiac
involvement during initial or
recurrent attacks of
Occurs in severe cardiac
involvement during initial or
recurrent attacks of
MITRAL REGURGE
(MR, Insufficiency, Regurgitation, Incompetence)
The mitral valve consists of:
an annulus
MITRAL REGURGE
(MR, Insufficiency, Regurgitation, Incompetence)
The mitral valve consists of:
an annulus

Healing of
ARF results in
Fibrosis & contracture of leaflets
Shortening &
Healing of
ARF results in
Fibrosis & contracture of leaflets
Shortening &
Mild MR → no symptoms
Severe MR → Symptoms of HF, pulmonary
Severe MR → Symptoms of HF, pulmonary
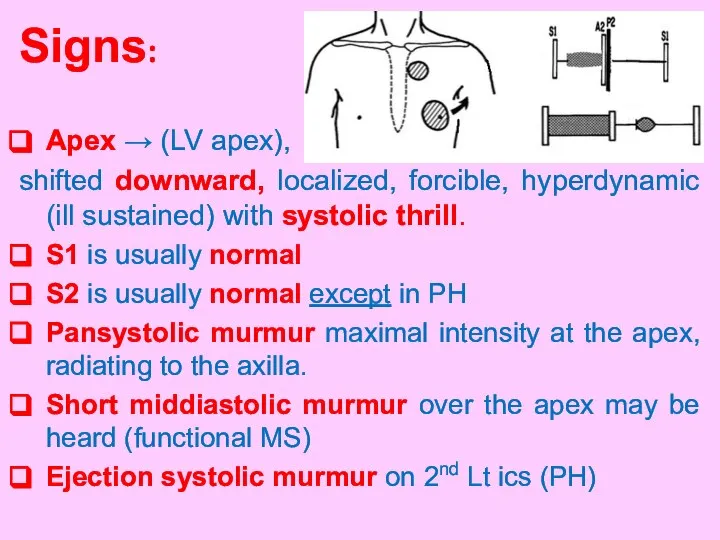
Signs:
Apex → (LV apex),
shifted downward, localized, forcible, hyperdynamic (ill sustained)
Signs:
Apex → (LV apex),
shifted downward, localized, forcible, hyperdynamic (ill sustained)

Mitral regurge CXR
Mitral regurge
Echocardiography
Mitral regurge CXR
Mitral regurge
Echocardiography

1- VSD:
-maximal intensity over the 3rd &
4th left intercostal
1- VSD:
-maximal intensity over the 3rd &
4th left intercostal
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against

MITRAL STENOSIS (MS)
Pathophysiology
-Thickening of valve leaflets
- Fusion of commissures
- Shortening
MITRAL STENOSIS (MS)
Pathophysiology
-Thickening of valve leaflets
- Fusion of commissures
- Shortening

The clinical course depends
on the severity of MS.
Symptoms:
Dyspnea on exertion.
Orthopnea
The clinical course depends
on the severity of MS.
Symptoms:
Dyspnea on exertion.
Orthopnea

Signs
Signs of RV hypertrophy:
a- The apex is diffuse and shifted
Signs
Signs of RV hypertrophy:
a- The apex is diffuse and shifted

Mitral stenosis CXR
Mitral stenosis echo
Mitral stenosis CXR
Mitral stenosis echo
Mitral flow murmur (functional MS)
associated with large VSD, PDA,
Mitral flow murmur (functional MS)
associated with large VSD, PDA,

Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against

Combined MS and MR
Dilatation, scaring and narrowing →
stenosis
Combined MS and MR
Dilatation, scaring and narrowing →
stenosis
Which of the following pathological change occur in rheumatic mitral stenosis

Rheumatic AR is the result of
fibrosis and contracture of the
Rheumatic AR is the result of
fibrosis and contracture of the

Symptoms
Depend on the severity.
In moderate and severe cases:
Effort intolerance, palpitation,
Symptoms
Depend on the severity.
In moderate and severe cases:
Effort intolerance, palpitation,

The rapid run off of the blood from aorta
during diastole
The rapid run off of the blood from aorta
during diastole

* Manifestations of LV enlargement.
The apex is shifted downword, forcible,
localized
The apex is shifted downword, forcible,
localized

Aortic regurge CXR Aortic regurge Echocardiography
Aortic regurge CXR Aortic regurge Echocardiography

Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against

AORTIC STENOSIS
- Commissural adhesions occur slowly and progressive → narrowing and
AORTIC STENOSIS
- Commissural adhesions occur slowly and progressive → narrowing and

In cases with severe stenosis:
Chest pain, exercise intolerance, dyspnea, syncope.
Clinical manifestations:
In cases with severe stenosis:
Chest pain, exercise intolerance, dyspnea, syncope.
Clinical manifestations:

- The apex: Localized, forceful & sustained (pressure overload).
- Systolic thrill
- The apex: Localized, forceful & sustained (pressure overload).
- Systolic thrill

Aortic stenosis CXR
Aortic stenosis Echocardiography
shows morphology of
Aortic stenosis CXR
Aortic stenosis Echocardiography
shows morphology of

→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against infective
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against infective

 Ультразвуковое исследование легких и плевры
Ультразвуковое исследование легких и плевры Предмет і завдання психіатрії та наркології. Класифікація психічних розладів і захворювань
Предмет і завдання психіатрії та наркології. Класифікація психічних розладів і захворювань Печень. Поджелудочная железа. Гистология
Печень. Поджелудочная железа. Гистология Спортивная медицина
Спортивная медицина Энцефалиты
Энцефалиты Завтрак школьника в условиях пандемии
Завтрак школьника в условиях пандемии Жұқпалы ауру және жүктілік
Жұқпалы ауру және жүктілік Антиген
Антиген Гемолитические анемии
Гемолитические анемии Мотивационно-потребностная сфера подростков(11-14 лет)
Мотивационно-потребностная сфера подростков(11-14 лет) Способности и прирожденные условия развития способностей
Способности и прирожденные условия развития способностей История и перспективы развития медико-социальной экспертизы Санкт-Петербурга. К 100-летию службы МСЭ
История и перспективы развития медико-социальной экспертизы Санкт-Петербурга. К 100-летию службы МСЭ Сердце. Физиология
Сердце. Физиология Агранулоцитарная ангина
Агранулоцитарная ангина Психология, патопсихология и психопатология сознания
Психология, патопсихология и психопатология сознания Ощущение, восприятие, память (занятие 14)
Ощущение, восприятие, память (занятие 14) Еңбек жағдайының гигиеналық бағалау критерийлері мен жіктелуі
Еңбек жағдайының гигиеналық бағалау критерийлері мен жіктелуі Гиповолемический шок
Гиповолемический шок Сестринский уход за пациентами с заболеваниями глотки
Сестринский уход за пациентами с заболеваниями глотки Патофизиология системы иммунобиологического надзора. Иммунодефицитные и иммунодепрессивные состояния. (Лекция 9, 10, 11)
Патофизиология системы иммунобиологического надзора. Иммунодефицитные и иммунодепрессивные состояния. (Лекция 9, 10, 11) Психологические особенности межличностных отношений в подростковом возрасте
Психологические особенности межличностных отношений в подростковом возрасте Топография таза и операции на органах таза
Топография таза и операции на органах таза Особенности новорожденного ребенка
Особенности новорожденного ребенка Высшая нервная деятельность
Высшая нервная деятельность ЭКГ в норме и при основных поражениях сердца
ЭКГ в норме и при основных поражениях сердца Анализ многолетней динамики заболеваемости в эпидемиологической диагностике
Анализ многолетней динамики заболеваемости в эпидемиологической диагностике Перфоративная язва желудка и двенадцатиперстной кишки
Перфоративная язва желудка и двенадцатиперстной кишки Темперамент
Темперамент