- Anemia

Содержание
- 2. Initial Laboratory Evaluation Complete blood count with indices: MCV – indication of RBC size. RDW –
- 3. Additional Labs Vitamin levels: iron profile, ferritin, Vitamin B12, folate. LDH, bilirubin, haptoglobin. Coomb’s test Hemoglobin
- 4. Definition of Anemia Reduction in the volume of RBC’s (hematocrit) or concentration (hemoglobin) when compared to
- 5. Morphology Classification Microcytic (MCV Iron deficiency, thalassemia, chronic disease/inflammation, sideroblastic anemia, lead poisoning. Normocytic (MCV 80-100
- 6. Case 1 A 35 year old woman has a history of pleurisy and has been told
- 7. Case 1 Initial Labs: Hemoglobin 7.9 gm/dL HCT 23.9% WBC 4000/mm3 with a normal differential Platelet
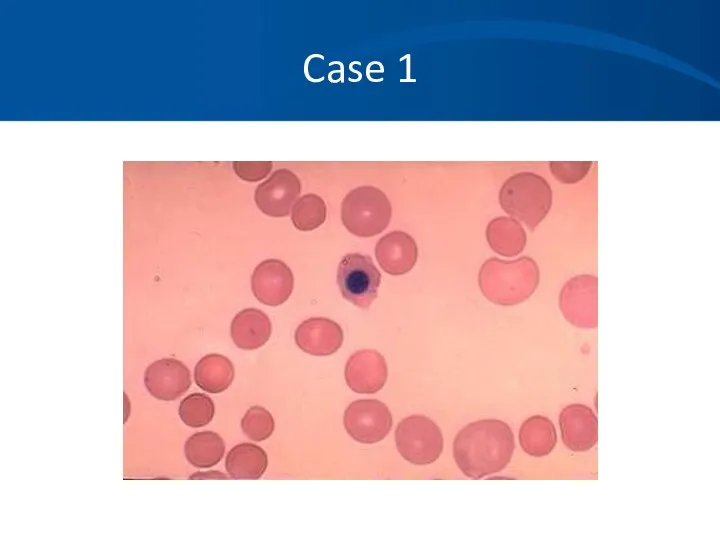
- 8. Case 1 MCV 114 Uncorrected Retic count 14.2% LDH 2343 U/L Bilirubin 4.3mg/dL Direct bili .8mg/dL
- 9. Case 1
- 10. Case 1 You suspect an autoimmune hemolytic anemia based on her history, Physical Exam, labs, and
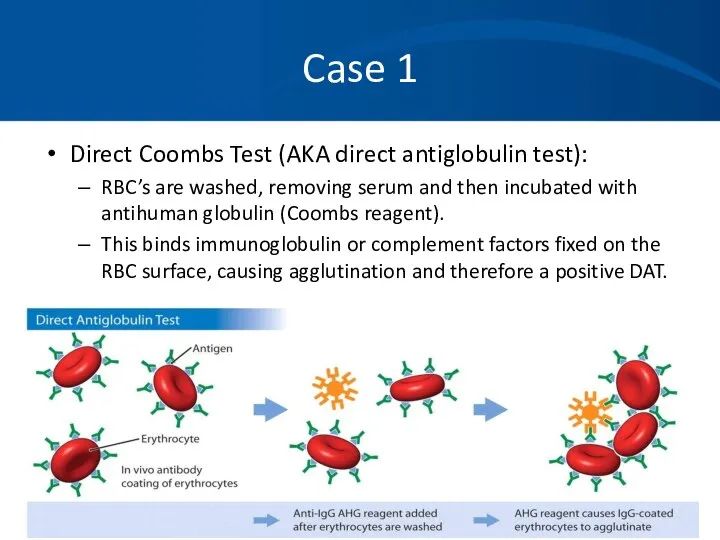
- 11. Case 1 Direct Coombs Test (AKA direct antiglobulin test): RBC’s are washed, removing serum and then
- 12. Case 1 Direct Coombs test results are as follows: DAT: Positive 3+ IgG: Positive 3+ Complement:
- 13. Case 1 You diagnose a warm-antibody hemolytic anemia and suspect an underlying autoimmune disorder. Etiology: Idiopathic
- 14. Case 1 You decide to avoid blood transfusion because of: The difficulties in obtaining cross match
- 15. Case 1 Treatment: Prednisone Splenectomy Rituximab (monoclonal antibody) Immunosuppressive agents Cytoxan, imuran, cyclosporin Danazol Plasma exchange
- 16. Case 1 You begin her on 60 mg Prednisone and she has a good response. Upon
- 17. Case 1 She responds well to splenectomy, but still requires very low maintenance doses of Prednisone.
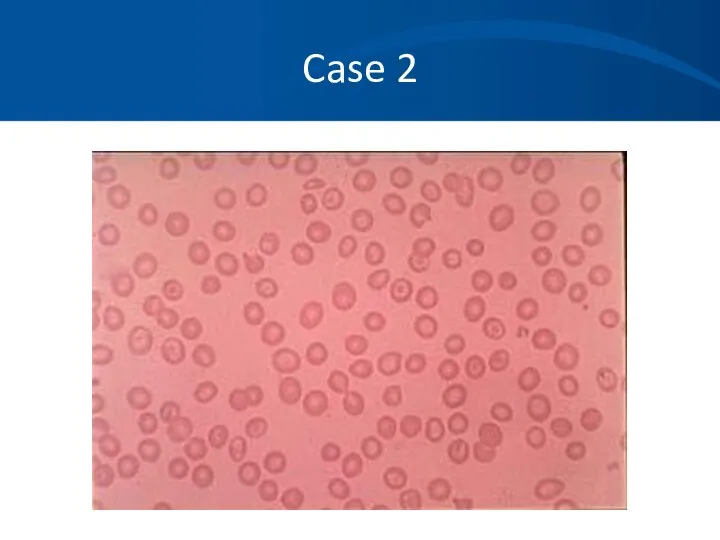
- 18. Case 2 You are referred a pleasant 34 year old African American woman who has been
- 19. Case 2 Labs: HCT 31-34% Hgb 10.6-11.4gm/dL PLT 232-312K/mm3 WBC 6500-8000/mm3 with a normal differential MCV
- 20. Case 2 Differential Diagnosis: Iron deficiency anemia Noncompliance, inadequate dosing, incorrect formulation. Beta thalassemia Alpha thalassemia
- 21. Case 2 Iron studies are normal. Chemistries, liver function tests, thyroid studies are normal. No history
- 22. Case 2
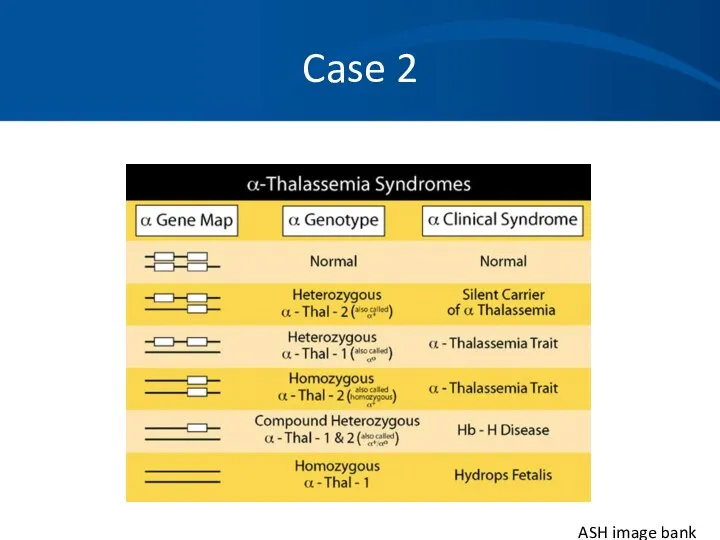
- 23. Case 2 ASH image bank
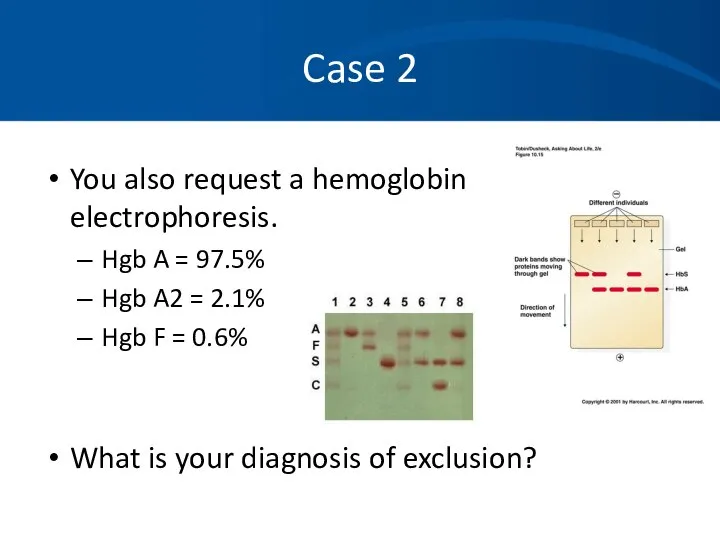
- 24. Case 2 You also request a hemoglobin electrophoresis. Hgb A = 97.5% Hgb A2 = 2.1%
- 25. Case 2 Alpha thalassemia with a double gene deletion. No treatment is necessary. Anemia is not
- 26. Case 3 A 32 year old previously healthy woman with no prior medical history presents to
- 27. Case 3 Physical exam confirms an ill appearing woman. T = 38.6, pulse 122, BP 123/54
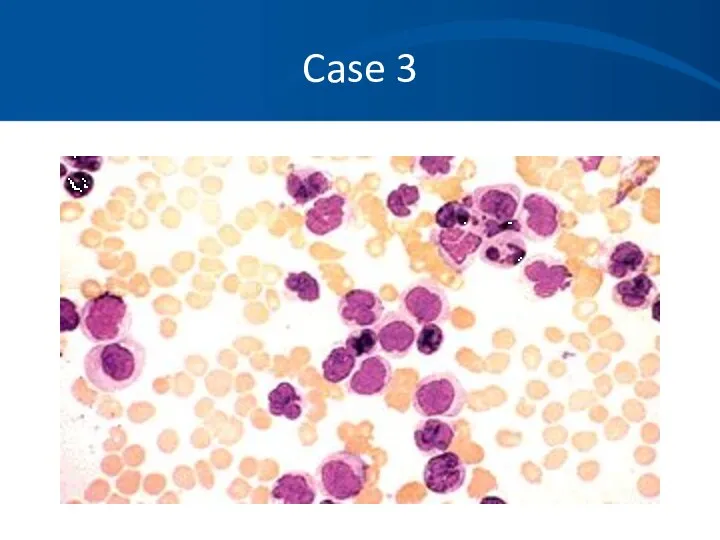
- 28. Case 3 Routine labs: WBC = 1700/mm3 Hgb = 5.6 gm/dL HCT 18.2% Platelet – 12,000/mm3
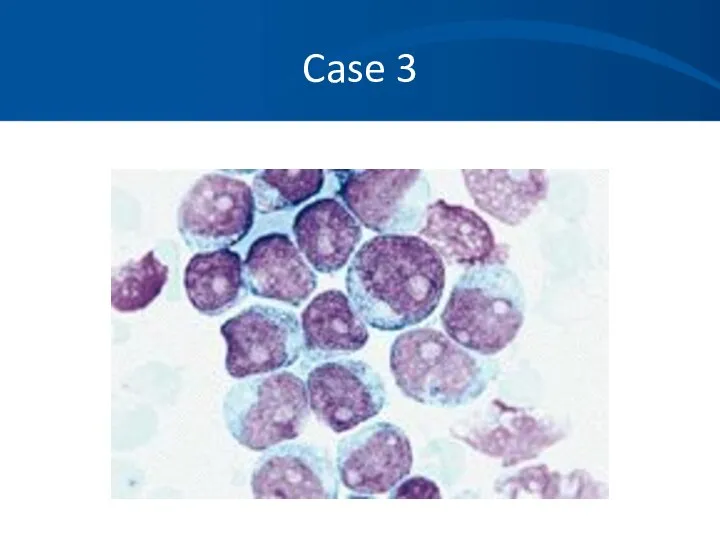
- 29. Case 3 Differential of the white blood cell count reveals at least 50% of young white
- 30. Case 3
- 31. Case 3
- 32. Case 3
- 33. Case 3 Hematopathology evaluation revealed AML subtype M1. Chromosomal studies were normal. What should you do
- 34. Case 3 The patient tolerated induction chemotherapy well and remains in remission 4 months after completing
- 35. Case 4 You are asked to see a 43 year old previously healthy woman who presented
- 36. Case 4 The ER attending notes: The patient to be ill appearing T 38.3, HR 123,
- 37. Case 4 Labs: WBC 5600/mm3, normal differential HCT 16.3% Hgb 5.3 gm/dL Platelets 21,000/mm3 PT 11
- 38. Case 4 Labs: Creatinine 2.4 mg/dL LDH 3000 U/L Bili 3.2 mg/dL, mostly indirect Reticulocyte count
- 39. Case 4
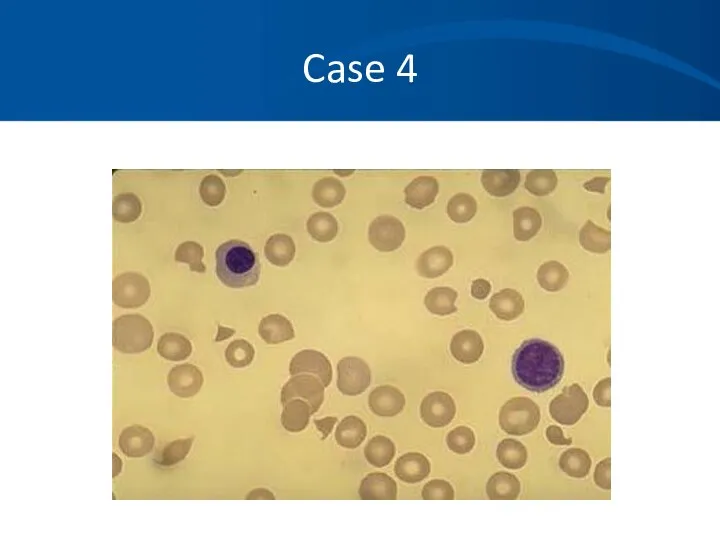
- 40. Case 4 What is your differential diagnosis based on the history, physical, labs and blood smear?
- 41. Case 4 You diagnosis TTP based on the classic pentad and consistent blood smear: Microangiopathic hemolytic
- 42. Case 4 You begin daily plasma exchange procedures using FFP as your replacement fluid. Her mental
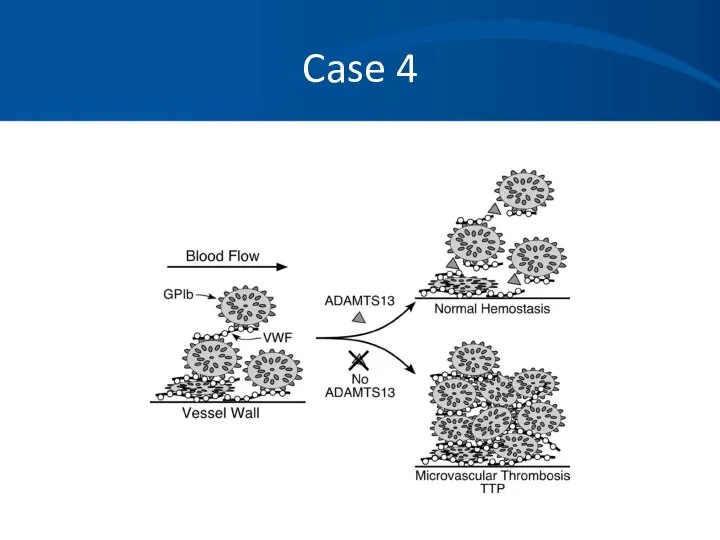
- 43. Case 4 Pathophysiology: Typically an inhibitor against ADAMTS- 13, a vWF cleaving to protease leading to
- 44. Case 4
- 45. Case 5 A 36 year old Caucasian man with a history of progressive renal failure over
- 46. Case 5 Physical exam is significant for pale sclera and an AV shunt in his left
- 47. Case 5 Prior labs reveal a hematocrit that was normal 4 years ago, but has steadily
- 48. Case 5
- 49. Case 5 Differential Diagnosis: Anemia of renal failure Iron deficiency anemia Thalassemia Lead poisoning Myelodysplasia Mixed
- 50. Case 5 You order an erythropoietin level which returns at 12 IU ( 4.1-19.5 ) within
- 51. Case 5 You place the patient on 10,000 units of EPO SQ tiw with dialysis. He
- 52. Case 5 He continues on his EPO injections for four months. Soon after he again becomes
- 53. Case 5
- 54. Case 5 You suspect with his increased reticulocytosis and hgb/hct over the last few months he
- 55. Case 5 He again feels much improved and is tolerating the iron fairly well. His hematocrit
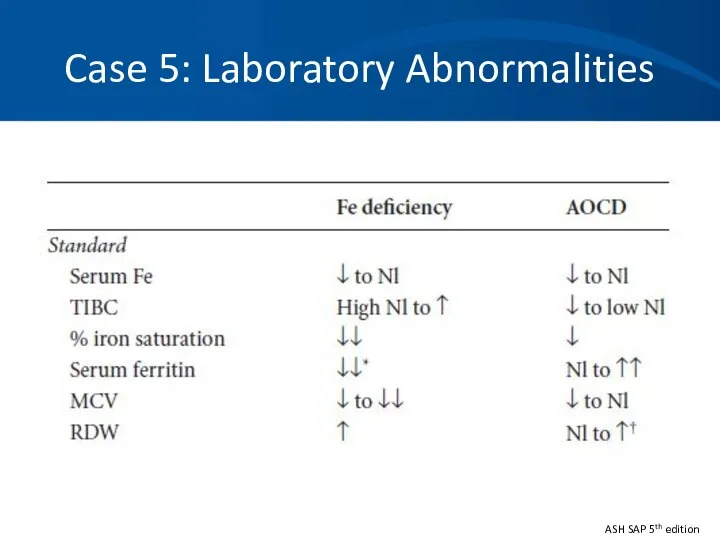
- 56. Case 5: Anemia of Chronic Inflammation Mild to moderate anemia that is persistent for greater than
- 57. Case 5: Pathophysiology Epo production is inhibited or decreased, so inappropriately low levels. Increased levels of
- 58. Case 5: Laboratory Abnormalities ASH SAP 5th edition
- 59. Case 5 ACI does not usually require treatment. Iron replacement is typically not necessary. Erythrocyte-stimulating agent
- 60. Case 6 A 53 year-old female complains of fatigue for 3 months. She falls and breaks
- 61. Case 6 What is the most likely diagnosis? How do you want to proceed with your
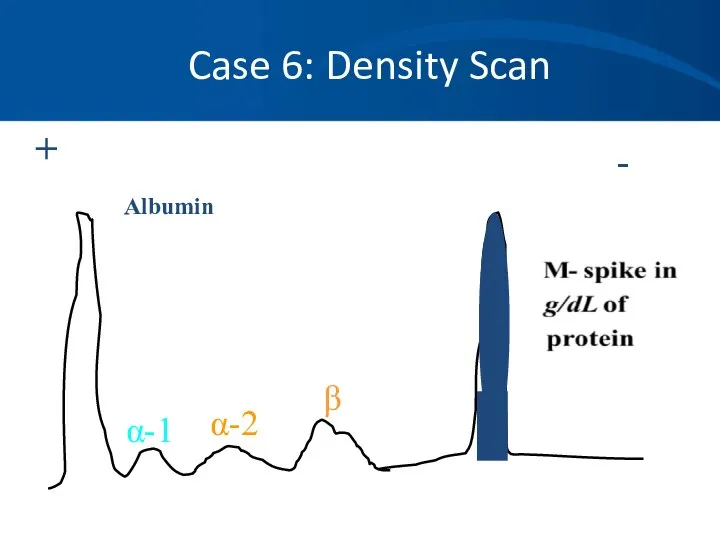
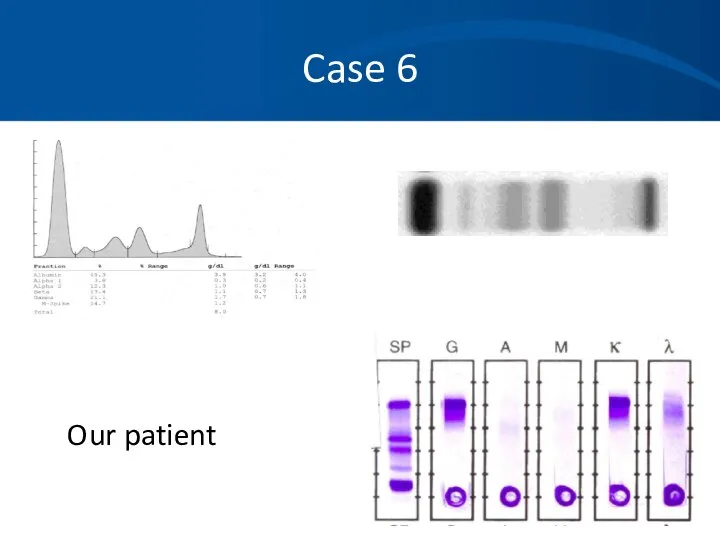
- 62. Case 6 Serum protein electrophoresis (SPEP) M- spike of 4.2 gm/dl Immunofixation (IFE) IgG lambda noted
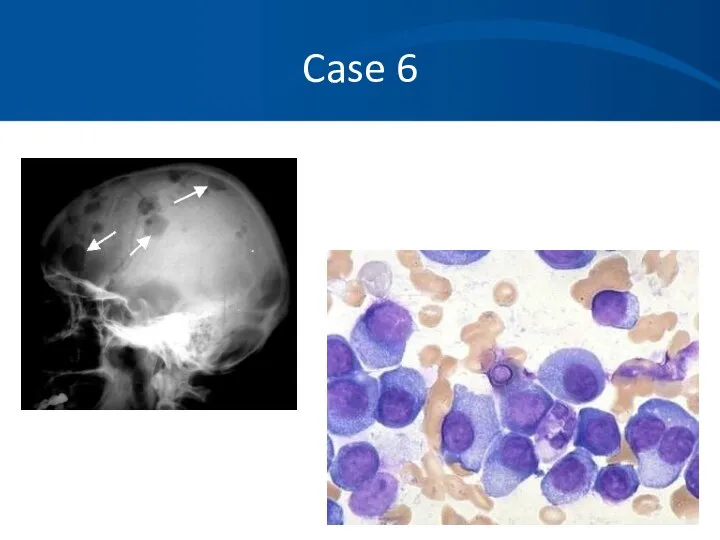
- 63. Case 6 Skeletal survey Multiple lytic lesions throughout the skeleton Bone Marrow aspirate and biopsy Sheets
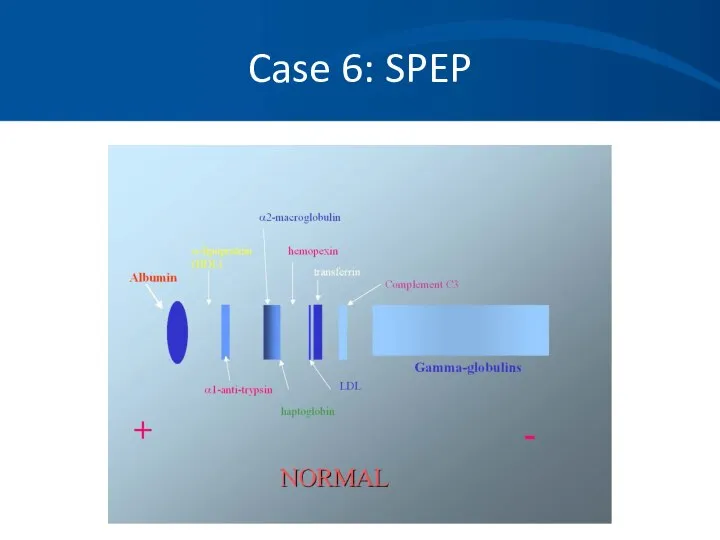
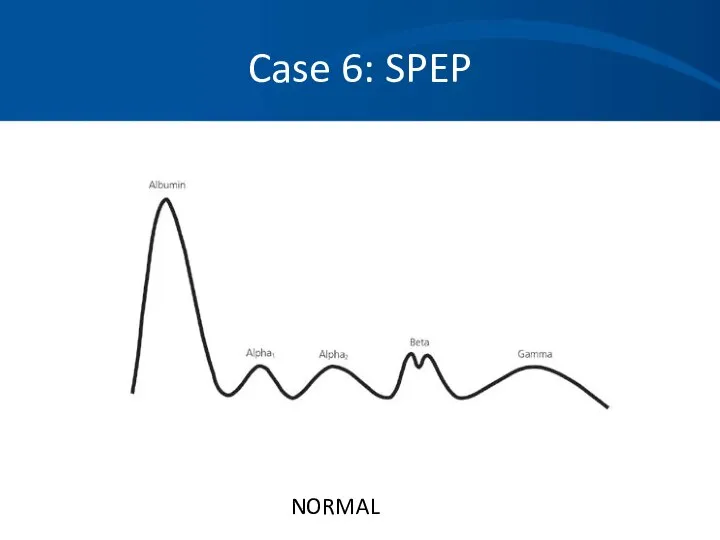
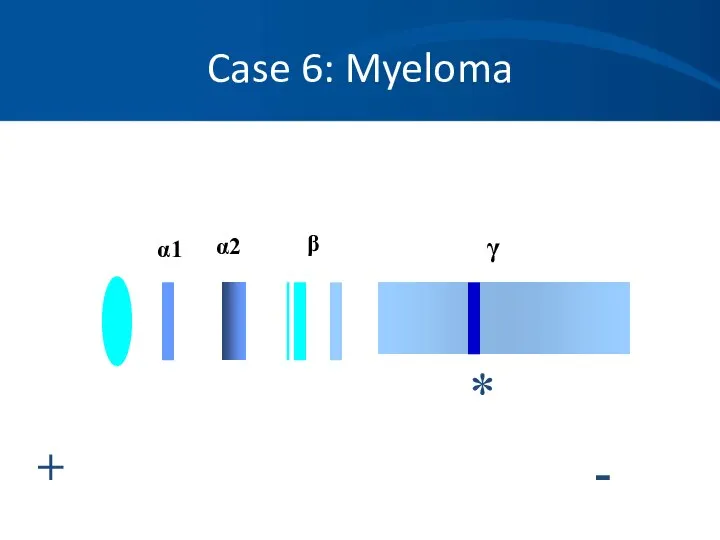
- 64. Case 6 An M-protein is usually seen as a discrete band on agarose gel electrophoresis in
- 65. Case 6: SPEP
- 66. Case 6: SPEP NORMAL
- 67. Case 6: Myeloma + - α1 α2 β γ *
- 68. Case 6: Density Scan + - Albumin α-1 α-2 β
- 69. Case 6 When to order an SPEP: When you suspect multiple myeloma, Waldenstrom’s macroglobulinemia or amyloidosis.
- 70. Case 6 Immunofixation (IFE): Proteins are fractioned on electrophoretic strips: Each lane overlaid with monospecific antisera
- 71. Case 6: Normal IFE gamma alpha mu kappa lambda SPE
- 72. Case 6 When to order an IFE: To type the paraprotein (M spike) identified on SPEP
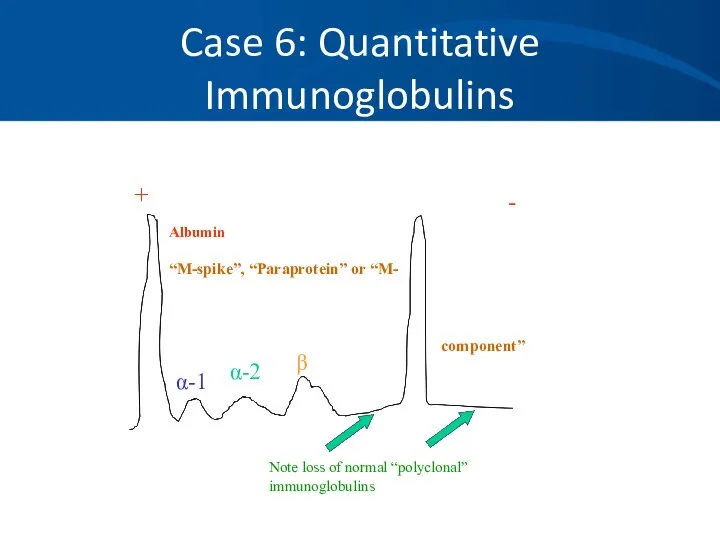
- 73. Case 6: Quantitative Immunoglobulins Useful to quantitate: The amount of monoclonal protein Suppression of uninvolved immunoglobulins
- 74. Case 6 Serum light chain assays are newer and a very sensitive technique for measuring serum
- 75. Case 6: Quantitative Immunoglobulins + - Albumin “M-spike”, “Paraprotein” or “M- α-1 α-2 β Note loss
- 76. Case 6 Our patient
- 77. Case 6
- 78. Case 6: Stage III Multiple Myeloma The patient is started on systemic chemotherapy and an autologous
- 79. Case A A 45 yo white male presents to his physician complaining of tiredness and fatigue
- 80. Case A Progression of symptoms Blood in stool Other medications or toxins, including EToH Prior history
- 81. Case A The patient does note he has had black tarry stools for a few weeks
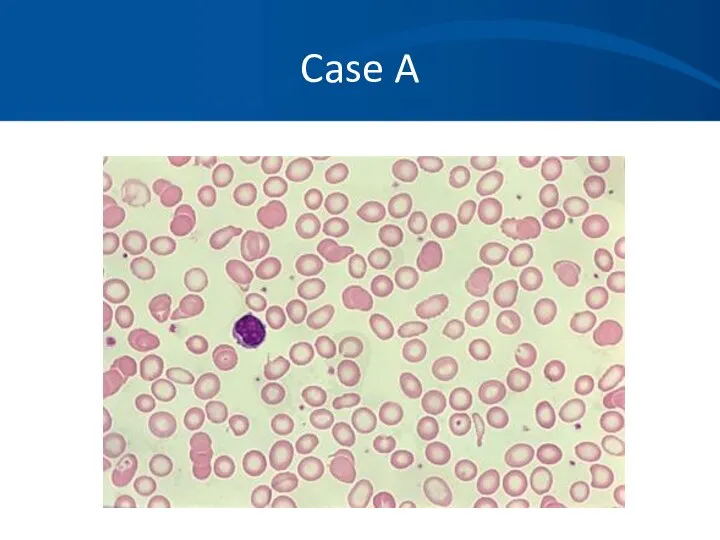
- 82. Case A You order a CBC which shows the following results: Hbg 8.2 gm/dL HCT 26%
- 83. Case A
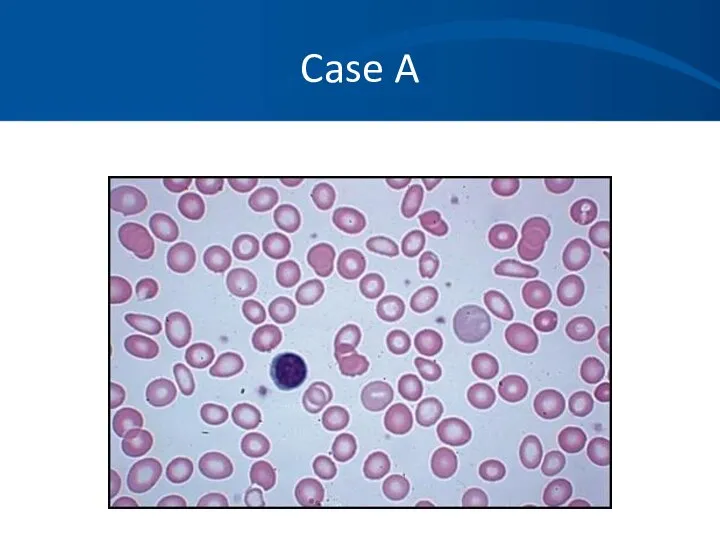
- 84. Case A Iron studies: Fe 14 ug/dL TIBC 426 ug/dL % sat 3% Ferritin 10ng/mL Corrected
- 85. Case A You confirm iron deficiency likely secondary to NSAID use. An endoscopy confirms a H.pylori
- 86. Case A He feels much better and has experienced resolution of his fatigue and lethargy. Hgb
- 87. Case A
- 88. Case B A 67 year old woman with a history of IDDM and treated hypothyroidism is
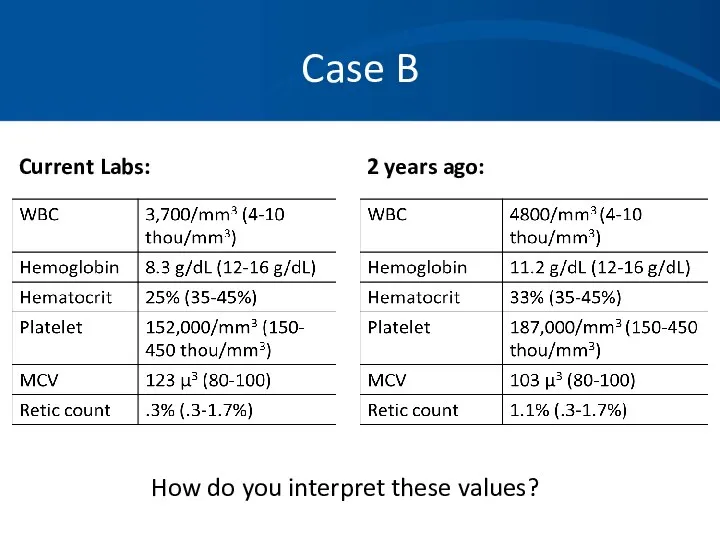
- 89. Case B Current Labs: 2 years ago: How do you interpret these values?
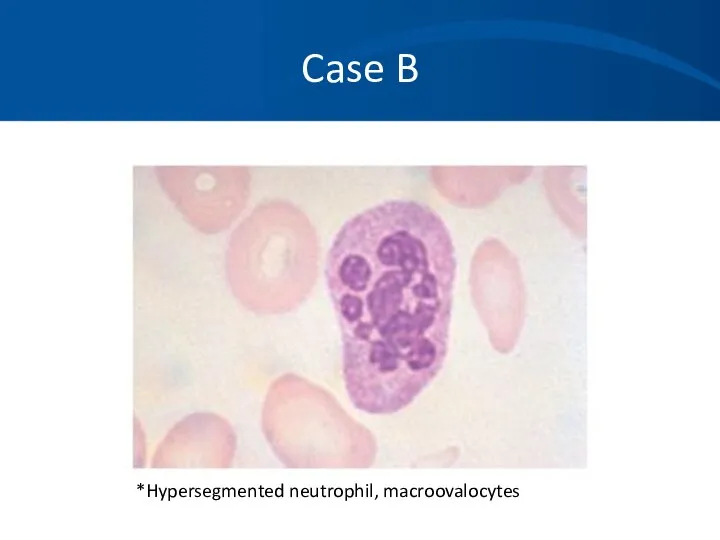
- 90. Case B *Hypersegmented neutrophil, macroovalocytes
- 91. Case B What tests or procedures do you want to perform to further evaluate this patient?
- 92. Case B You diagnose B12 deficiency and prescribe B12 injections 1000ug weekly x4 then 1000ug a
- 93. Case B: Vitamin B12 Deficiency Found primarily in animal meats. Large hepatic reservoir. Deficiency from decreased
- 94. Case B: Vitamin B12 Deficiency Clinical findings: Insidious onset. Glossitis, weight loss, pale yellow skin. Neurologic
- 95. Case B: Vitamin B12 Deficiency Lab findings: Cobalamin If low-normal (200-350ng/L), check homocysteine and MMA. Both
- 97. Скачать презентацию
Initial Laboratory Evaluation
Complete blood count with indices:
MCV – indication of
Initial Laboratory Evaluation
Complete blood count with indices:
MCV – indication of
Additional Labs
Vitamin levels: iron profile, ferritin, Vitamin B12, folate.
LDH, bilirubin,
Additional Labs
Vitamin levels: iron profile, ferritin, Vitamin B12, folate.
LDH, bilirubin,
Definition of Anemia
Reduction in the volume of RBC’s (hematocrit) or concentration
Definition of Anemia
Reduction in the volume of RBC’s (hematocrit) or concentration
Morphology Classification
Microcytic (MCV <80 µ3):
Iron deficiency, thalassemia, chronic disease/inflammation, sideroblastic
Morphology Classification
Microcytic (MCV <80 µ3):
Iron deficiency, thalassemia, chronic disease/inflammation, sideroblastic
Case 1
A 35 year old woman has a history of pleurisy
Case 1
A 35 year old woman has a history of pleurisy
Case 1
Initial Labs:
Hemoglobin 7.9 gm/dL
HCT 23.9%
WBC 4000/mm3 with a normal
Case 1
Initial Labs:
Hemoglobin 7.9 gm/dL
HCT 23.9%
WBC 4000/mm3 with a normal
Case 1
MCV 114
Uncorrected Retic count 14.2%
LDH 2343 U/L
Bilirubin 4.3mg/dL
Direct bili
Case 1
MCV 114
Uncorrected Retic count 14.2%
LDH 2343 U/L
Bilirubin 4.3mg/dL
Direct bili
Case 1
Case 1
Case 1
You suspect an autoimmune hemolytic anemia based on her history,
Case 1
You suspect an autoimmune hemolytic anemia based on her history,
Case 1
Direct Coombs Test (AKA direct antiglobulin test):
RBC’s are washed,
Case 1
Direct Coombs Test (AKA direct antiglobulin test):
RBC’s are washed,
Case 1
Direct Coombs test results are as follows:
DAT: Positive 3+
IgG:
Case 1
Direct Coombs test results are as follows:
DAT: Positive 3+
IgG:
Case 1
You diagnose a warm-antibody hemolytic anemia and suspect an underlying
Case 1
You diagnose a warm-antibody hemolytic anemia and suspect an underlying
Case 1
You decide to avoid blood transfusion because of:
The difficulties
Case 1
You decide to avoid blood transfusion because of:
The difficulties
Case 1
Treatment:
Prednisone
Splenectomy
Rituximab (monoclonal antibody)
Immunosuppressive agents
Cytoxan, imuran, cyclosporin
Danazol
Plasma exchange
Case 1
Treatment:
Prednisone
Splenectomy
Rituximab (monoclonal antibody)
Immunosuppressive agents
Cytoxan, imuran, cyclosporin
Danazol
Plasma exchange
Case 1
You begin her on 60 mg Prednisone and she has
Case 1
You begin her on 60 mg Prednisone and she has
Case 1
She responds well to splenectomy, but still requires very low
Case 1
She responds well to splenectomy, but still requires very low
Case 2
You are referred a pleasant 34 year old African American
Case 2
You are referred a pleasant 34 year old African American
Case 2
Labs:
HCT 31-34%
Hgb 10.6-11.4gm/dL
PLT 232-312K/mm3
WBC 6500-8000/mm3 with a normal differential
MCV
Case 2
Labs:
HCT 31-34%
Hgb 10.6-11.4gm/dL
PLT 232-312K/mm3
WBC 6500-8000/mm3 with a normal differential
MCV
Case 2
Differential Diagnosis:
Iron deficiency anemia
Noncompliance, inadequate dosing, incorrect formulation.
Beta
Case 2
Differential Diagnosis:
Iron deficiency anemia
Noncompliance, inadequate dosing, incorrect formulation.
Beta
Case 2
Iron studies are normal.
Chemistries, liver function tests, thyroid studies
Case 2
Iron studies are normal.
Chemistries, liver function tests, thyroid studies
Case 2
Case 2
Case 2
ASH image bank
Case 2
ASH image bank
Case 2
You also request a hemoglobin electrophoresis.
Hgb A = 97.5%
Hgb
Case 2
You also request a hemoglobin electrophoresis.
Hgb A = 97.5%
Hgb
Case 2
Alpha thalassemia with a double gene deletion.
No treatment is
Case 2
Alpha thalassemia with a double gene deletion.
No treatment is
Case 3
A 32 year old previously healthy woman with no prior
Case 3
A 32 year old previously healthy woman with no prior
Case 3
Physical exam confirms an ill appearing woman.
T = 38.6,
Case 3
Physical exam confirms an ill appearing woman.
T = 38.6,
Case 3
Routine labs:
WBC = 1700/mm3
Hgb = 5.6 gm/dL
HCT 18.2%
Platelet –
Case 3
Routine labs:
WBC = 1700/mm3
Hgb = 5.6 gm/dL
HCT 18.2%
Platelet –
Case 3
Differential of the white blood cell count reveals at least
Case 3
Differential of the white blood cell count reveals at least
Case 3
Case 3
Case 3
Case 3
Case 3
Case 3
Case 3
Hematopathology evaluation revealed AML subtype M1.
Chromosomal studies were normal.
Case 3
Hematopathology evaluation revealed AML subtype M1.
Chromosomal studies were normal.
Case 3
The patient tolerated induction chemotherapy well and remains in remission
Case 3
The patient tolerated induction chemotherapy well and remains in remission
Case 4
You are asked to see a 43 year old previously
Case 4
You are asked to see a 43 year old previously
Case 4
The ER attending notes:
The patient to be ill appearing
T
Case 4
The ER attending notes:
The patient to be ill appearing
T
Case 4
Labs:
WBC 5600/mm3, normal differential
HCT 16.3%
Hgb 5.3 gm/dL
Platelets 21,000/mm3
PT 11
Case 4
Labs:
WBC 5600/mm3, normal differential
HCT 16.3%
Hgb 5.3 gm/dL
Platelets 21,000/mm3
PT 11
Case 4
Labs:
Creatinine 2.4 mg/dL
LDH 3000 U/L
Bili 3.2 mg/dL, mostly indirect
Reticulocyte
Case 4
Labs:
Creatinine 2.4 mg/dL
LDH 3000 U/L
Bili 3.2 mg/dL, mostly indirect
Reticulocyte
Case 4
Case 4
Case 4
What is your differential diagnosis based on the history, physical,
Case 4
What is your differential diagnosis based on the history, physical,
Case 4
You diagnosis TTP based on the classic pentad and consistent
Case 4
You diagnosis TTP based on the classic pentad and consistent
Case 4
You begin daily plasma exchange procedures using FFP as your
Case 4
You begin daily plasma exchange procedures using FFP as your
Case 4
Pathophysiology:
Typically an inhibitor against ADAMTS- 13, a vWF cleaving
Case 4
Pathophysiology:
Typically an inhibitor against ADAMTS- 13, a vWF cleaving
Case 4
Case 4
Case 5
A 36 year old Caucasian man with a history of
Case 5
A 36 year old Caucasian man with a history of
Case 5
Physical exam is significant for pale sclera and an AV
Case 5
Physical exam is significant for pale sclera and an AV
Case 5
Prior labs reveal a hematocrit that was normal 4 years
Case 5
Prior labs reveal a hematocrit that was normal 4 years
Case 5
Case 5
Case 5
Differential Diagnosis:
Anemia of renal failure
Iron deficiency anemia
Thalassemia
Lead poisoning
Myelodysplasia
Mixed microcytic
Case 5
Differential Diagnosis:
Anemia of renal failure
Iron deficiency anemia
Thalassemia
Lead poisoning
Myelodysplasia
Mixed microcytic
Case 5
You order an erythropoietin level which returns at 12 IU
Case 5
You order an erythropoietin level which returns at 12 IU
Case 5
You place the patient on 10,000 units of EPO SQ
Case 5
You place the patient on 10,000 units of EPO SQ
Case 5
He continues on his EPO injections for four months. Soon after
Case 5
He continues on his EPO injections for four months. Soon after
Case 5
Case 5
Case 5
You suspect with his increased reticulocytosis and hgb/hct over the
Case 5
You suspect with his increased reticulocytosis and hgb/hct over the
Case 5
He again feels much improved and is tolerating the iron
Case 5
He again feels much improved and is tolerating the iron
Case 5: Anemia of Chronic Inflammation
Mild to moderate anemia that is
Case 5: Anemia of Chronic Inflammation
Mild to moderate anemia that is
Case 5: Pathophysiology
Epo production is inhibited or decreased, so inappropriately low
Case 5: Pathophysiology
Epo production is inhibited or decreased, so inappropriately low
Case 5: Laboratory Abnormalities
ASH SAP 5th edition
Case 5: Laboratory Abnormalities
ASH SAP 5th edition
Case 5
ACI does not usually require treatment.
Iron replacement is typically
Case 5
ACI does not usually require treatment.
Iron replacement is typically
Case 6
A 53 year-old female complains of fatigue for 3 months.
Case 6
A 53 year-old female complains of fatigue for 3 months.
Case 6
What is the most likely diagnosis?
How do you want to
Case 6
What is the most likely diagnosis?
How do you want to
Case 6
Serum protein electrophoresis (SPEP)
M- spike of 4.2 gm/dl
Immunofixation (IFE)
IgG lambda
Case 6
Serum protein electrophoresis (SPEP)
M- spike of 4.2 gm/dl
Immunofixation (IFE)
IgG lambda
Case 6
Skeletal survey
Multiple lytic lesions throughout the skeleton
Bone Marrow aspirate and
Case 6
Skeletal survey
Multiple lytic lesions throughout the skeleton
Bone Marrow aspirate and
Case 6
An M-protein is usually seen as a discrete band on
Case 6
An M-protein is usually seen as a discrete band on
Case 6: SPEP
Case 6: SPEP
Case 6: SPEP
NORMAL
Case 6: SPEP
NORMAL
Case 6: Myeloma
+
-
α1
α2
β
γ
*
Case 6: Myeloma
+
-
α1
α2
β
γ
*
Case 6: Density Scan
+
-
Albumin
α-1
α-2
β
Case 6: Density Scan
+
-
Albumin
α-1
α-2
β
Case 6
When to order an SPEP:
When you suspect multiple myeloma,
Case 6
When to order an SPEP:
When you suspect multiple myeloma,
Case 6
Immunofixation (IFE):
Proteins are fractioned on electrophoretic strips:
Each lane overlaid
Case 6
Immunofixation (IFE):
Proteins are fractioned on electrophoretic strips:
Each lane overlaid
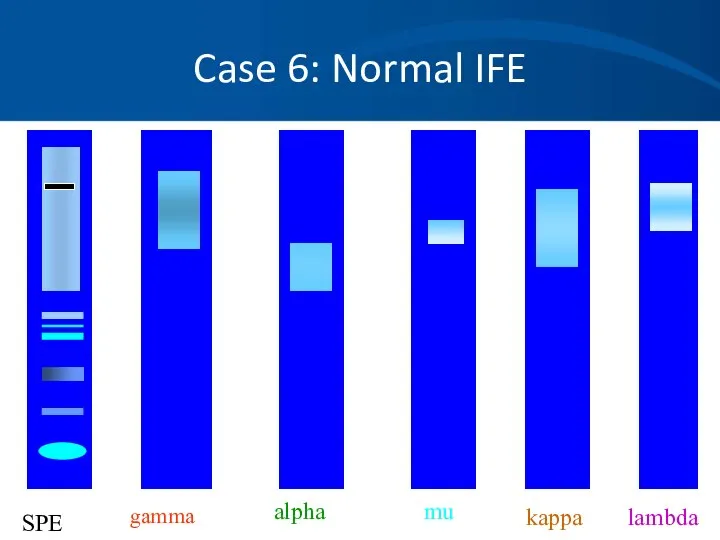
Case 6: Normal IFE
gamma
alpha
mu
kappa
lambda
SPE
Case 6: Normal IFE
gamma
alpha
mu
kappa
lambda
SPE
Case 6
When to order an IFE:
To type the paraprotein (M
Case 6
When to order an IFE:
To type the paraprotein (M
Case 6: Quantitative Immunoglobulins
Useful to quantitate:
The amount of monoclonal protein
Suppression
Case 6: Quantitative Immunoglobulins
Useful to quantitate:
The amount of monoclonal protein
Suppression
Case 6
Serum light chain assays are newer and a very sensitive
Case 6
Serum light chain assays are newer and a very sensitive
Case 6: Quantitative Immunoglobulins
+
-
Albumin
“M-spike”, “Paraprotein” or “M-
α-1
α-2
β
Note loss of normal “polyclonal”
Case 6: Quantitative Immunoglobulins
+
-
Albumin
“M-spike”, “Paraprotein” or “M-
α-1
α-2
β
Note loss of normal “polyclonal”
Case 6
Our patient
Case 6
Our patient
Case 6
Case 6
Case 6: Stage III Multiple Myeloma
The patient is started on systemic
Case 6: Stage III Multiple Myeloma
The patient is started on systemic
Case A
A 45 yo white male presents to his physician complaining
Case A
A 45 yo white male presents to his physician complaining
Case A
Progression of symptoms
Blood in stool
Other medications or toxins, including EToH
Prior
Case A
Progression of symptoms
Blood in stool
Other medications or toxins, including EToH
Prior
Case A
The patient does note he has had black tarry stools
Case A
The patient does note he has had black tarry stools
Case A
You order a CBC which shows the following results:
Hbg
Case A
You order a CBC which shows the following results:
Hbg
Case A
Case A
Case A
Iron studies:
Fe 14 ug/dL
TIBC 426 ug/dL
% sat 3%
Ferritin 10ng/mL
Corrected
Case A
Iron studies:
Fe 14 ug/dL
TIBC 426 ug/dL
% sat 3%
Ferritin 10ng/mL
Corrected
Case A
You confirm iron deficiency likely secondary to NSAID use. An endoscopy
Case A
You confirm iron deficiency likely secondary to NSAID use. An endoscopy
Case A
He feels much better and has experienced resolution of his
Case A
He feels much better and has experienced resolution of his
Case A
Case A
Case B
A 67 year old woman with a history of IDDM
Case B
A 67 year old woman with a history of IDDM
Case B
Current Labs:
2 years ago:
How do you interpret these values?
Case B
Current Labs:
2 years ago:
How do you interpret these values?
Case B
*Hypersegmented neutrophil, macroovalocytes
Case B
*Hypersegmented neutrophil, macroovalocytes

Case B
What tests or procedures do you want to perform to
Case B
What tests or procedures do you want to perform to
Case B
You diagnose B12 deficiency and prescribe B12 injections 1000ug weekly
Case B
You diagnose B12 deficiency and prescribe B12 injections 1000ug weekly
Case B: Vitamin B12 Deficiency
Found primarily in animal meats.
Large hepatic
Case B: Vitamin B12 Deficiency
Found primarily in animal meats.
Large hepatic
Case B: Vitamin B12 Deficiency
Clinical findings:
Insidious onset.
Glossitis, weight loss, pale
Case B: Vitamin B12 Deficiency
Clinical findings:
Insidious onset.
Glossitis, weight loss, pale
Case B: Vitamin B12 Deficiency
Lab findings:
Cobalamin <200ng/L.
If low-normal (200-350ng/L), check
Case B: Vitamin B12 Deficiency
Lab findings:
Cobalamin <200ng/L.
If low-normal (200-350ng/L), check
 Б±ќаралыќ аќпарат ќ±ралдары
Б±ќаралыќ аќпарат ќ±ралдары Защити себя от ВИЧ
Защити себя от ВИЧ Состояние здоровья и физическое развитие детей и подростков
Состояние здоровья и физическое развитие детей и подростков ЗОЖ
ЗОЖ Гепатит A, C, G, T вирусы
Гепатит A, C, G, T вирусы Остеохондроз позвоночника. Рентгенографические признаки остеохондроза
Остеохондроз позвоночника. Рентгенографические признаки остеохондроза Вплив алкоголю та паління на репродуктивну систему і потомство
Вплив алкоголю та паління на репродуктивну систему і потомство Причины нарушений зрения
Причины нарушений зрения Регуляторные системы организма. Органы иммунной системы. Нормальные и патологические реакции иммунной системы
Регуляторные системы организма. Органы иммунной системы. Нормальные и патологические реакции иммунной системы Гематологические исследования
Гематологические исследования Хронический бронхит
Хронический бронхит Заболевания щитовидной железы
Заболевания щитовидной железы Партограмма
Партограмма Сестринский уход при различных заболеваниях и состояниях. Сестринская помощь в хирургии. Кровотечение и гемостаз
Сестринский уход при различных заболеваниях и состояниях. Сестринская помощь в хирургии. Кровотечение и гемостаз Туберкулез кезіндегі шаралар стандарттары мен алгоритмдері
Туберкулез кезіндегі шаралар стандарттары мен алгоритмдері ICH процесі шеңберіндегі CTD жалпы техникалық құжаты
ICH процесі шеңберіндегі CTD жалпы техникалық құжаты Тестовый контроль по теме: Инфузии и основы трансфузиологии для специальности Сестринское дело
Тестовый контроль по теме: Инфузии и основы трансфузиологии для специальности Сестринское дело Рентгенографическая и компьютерно-томографическая диагностика острых и хронических синуситов
Рентгенографическая и компьютерно-томографическая диагностика острых и хронических синуситов Витамины
Витамины Вербальные и невербальные коммуникации
Вербальные и невербальные коммуникации Правильные ответы викторины по станции Медицинская
Правильные ответы викторины по станции Медицинская Вегетативная нервная система и синдромы ее нарушения
Вегетативная нервная система и синдромы ее нарушения Антибиотики: лечат или калечат
Антибиотики: лечат или калечат То что просто для детей, невозможно для взрослых. 2 класс
То что просто для детей, невозможно для взрослых. 2 класс Синдром марфана
Синдром марфана Эпидемиология РМЖ
Эпидемиология РМЖ Комбинированные поражения (лекция № 5)
Комбинированные поражения (лекция № 5) Обследование больного в ортопедическом отделении. Оформление документации. Деонтология и этика в ортопедической стоматологии
Обследование больного в ортопедическом отделении. Оформление документации. Деонтология и этика в ортопедической стоматологии