- Meningococcal infection

Содержание
- 2. Meningococcal infection occurs on the all continents. It is serious problem for public health. It is
- 3. The zone lying between 5 and 15 degree N of the equator in tropical Africa is
- 4. Meningococcal infection is an acute infectious disease of the caused by meningococcus Neisseria Meningitidis. Meningococcal disease
- 5. The main clinical syndromes characterize meningococcal infection: Intoxication syndrome; Hemorrhagic rash
- 6. Meningeal syndrome
- 7. Waterhause-Fridrechsen syndrome Hemorrhages in the adrenal glands and others organs
- 8. The disease is characterized by damage of the -- mucous membrane of nasopharynx (nasopharingitis); Generalization of
- 9. The causative agent is Neisseria meningitidis. It is small gramm-negative diplococcus, aerobic, and possesses a polysaccharide
- 10. Meningococcus may be seen inside and outside of neutrophils. The main serogroups of the pathogenic organisms
- 11. Serological classification: Meningococci are divisible into various serogroups: Group A is in most countries, the serogroup
- 12. Group B meningococci are seen in both epidemic and outbreak situations; Group C strains have been
- 13. Serogroups Z and 29E (Z') are killed by normal human serum; they rarely cause disease and
- 14. Meningococci are very exacting to composition of nutritive mediums. Its reproduction may be only in presence
- 15. The agent of meningococcal infection is characterized by low resistance in the environment. Meningococci perish in
- 16. Epidemiology Meningococcal infections occur worldwide and are notifiable in most countries. About two-thirds of cases occur
- 17. The incidence of meningococcal infection is increasing. Acute meningitis causes about 150000 deaths per year. Epidemic
- 18. Epidemic strains of group A or group B may give rise to a high incidence of
- 19. The patients with generalized form are more dangerous. It is proved than they are dangerous for
- 20. The mechanism of transmission of the infection is air-drop. The infection is realized in cough, sneezing.
- 21. In this the narrow contact and sufficient exposition are necessary. It was proved that the infection
- 22. In meningococcal infection epidemic process is characterized by seasonal spread. The morbidity may compose 60-70% from
- 23. Pathogenesis In meningococcal infection the entrance gates is mucous membrane of nasopharynx. It is the place
- 24. The stages of inculcation on the mucous membrane of nasopharynx and penetration of meningococcus into the
- 25. Meningococci are able to break local barriers with help of factors of spread (hyaluronidase). Capsule protects
- 26. Meningococci penetrate into the blood after break of protective barriers of the mucous membrane of the
- 27. It may be septic course of meningococcemia with formation of the secondary metastatic focuses in the
- 28. Thus, the meningococci enter into subarachnoid space, multiply and course serous-purulent and purulent inflammation of the
- 29. In the pathogenesis of meningococcal infection toxic and allergic components play an important role. Thus, in
- 30. The severe complication may develop as a result of expressive toxicosis. It is cerebral hypertension, leading
- 31. Clinical manifestation Classification of the clinical forms of meningococcal infection: I. Primarily localized forms: a) meningococcal
- 32. II. Generalized forms: a) meningococcemia: typical, acute meningococcal sepsis; chronic; b) meningitis; meningoencephalitis; c) mixed forms
- 33. Meningococcal nasopharyngitis The most common complains of the a patients are headache, mainly in the frontal-parietal
- 34. Meningococcal nasopharyngitis There are hyperemia and edema of the mucous membrane of the nose. In many
- 35. Meningitis It may start after meningococcal nasopharyngitis, but sometimes primary symptoms of the disease arise suddenly.
- 36. Temperature increases quickly with chill and may reach 40-41° for few hours. The patients suffer from
- 37. The disorders of consciousness occupy the great place in the clinical picture (from sopor till coma).
- 38. The fulminant course of meningitis with syndrome of brain swelling and edema is the most unfavorable
- 39. Meningococcemia (meningococcal sepsis). The disease is more impetuous, with symptoms of toxicosis and development of the
- 45. Exanthema is more clear, constant and diagnostically valuable sign of meningococcemia. Dermal rashes appear in 5-15
- 46. The deep and extensive hemorrhages may be necrotic. Then it may be formation of deep ulcers.
- 47. Laboratory diagnostic Specific methods Bacteriological method Material for bacteriological examination - a smear of the mucous
- 48. The examination of cerebrospinal fluid (CSF) has the great meaning in diagnostics of meningitis. On lumbar
- 49. Treatment The therapeutic tactics depends on the clinical forms. In the moderate and middle serious course
- 50. In the therapy of generalized forms of meningococcal infection used Benzylpenicillin in dosage of 300 000
- 51. Daily dose is injected to the patient every 3 hours. In some cases interval between injections
- 52. If pleocytosis more than 100 cells in 1 mcl or predominate neutrophyles antibacterial therapy is necessary
- 54. Скачать презентацию

Meningococcal infection
occurs on the all continents. It is serious
Meningococcal infection
occurs on the all continents. It is serious

The zone lying between 5 and 15 degree N of the
The zone lying between 5 and 15 degree N of the

Meningococcal infection is an acute infectious disease of the caused by
Meningococcal infection is an acute infectious disease of the caused by

The main clinical syndromes characterize meningococcal infection:
Intoxication syndrome;
Hemorrhagic rash
The main clinical syndromes characterize meningococcal infection:
Intoxication syndrome;
Hemorrhagic rash
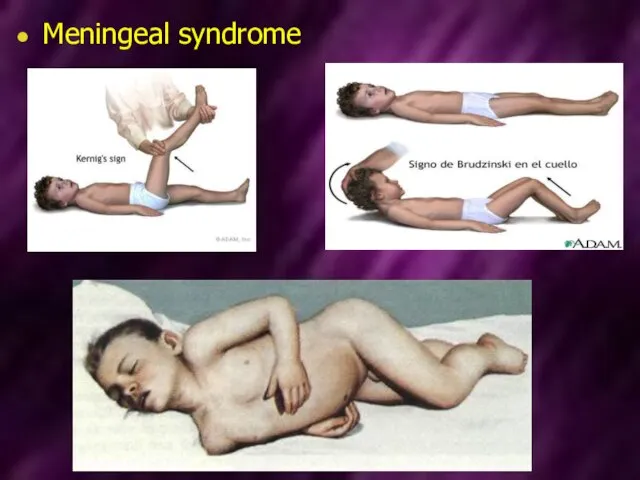
Meningeal syndrome
Meningeal syndrome

Waterhause-Fridrechsen syndrome
Hemorrhages
in the adrenal glands and others organs
Waterhause-Fridrechsen syndrome
Hemorrhages
in the adrenal glands and others organs

The disease is characterized by damage of the -- mucous membrane
The disease is characterized by damage of the -- mucous membrane
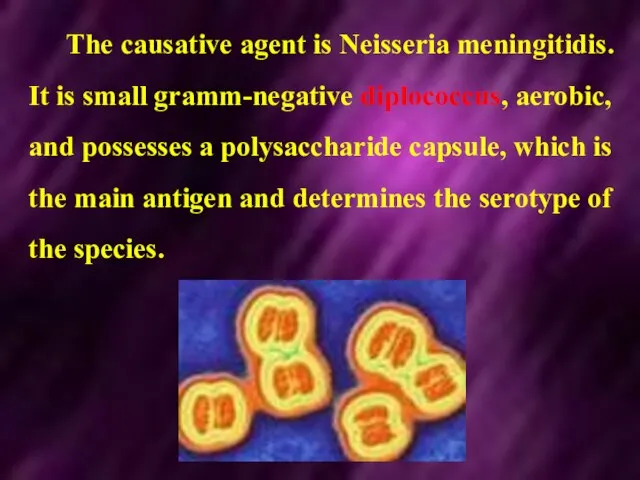
The causative agent is Neisseria meningitidis. It is small gramm-negative diplococcus,
The causative agent is Neisseria meningitidis. It is small gramm-negative diplococcus,
Meningococcus may be seen inside and outside of neutrophils. The main
Meningococcus may be seen inside and outside of neutrophils. The main

Serological classification:
Meningococci are divisible into various serogroups:
Group A is in most
Serological classification:
Meningococci are divisible into various serogroups:
Group A is in most

Group B meningococci are seen in both epidemic and outbreak situations;
Group
Group B meningococci are seen in both epidemic and outbreak situations;
Group

Serogroups Z and 29E (Z') are killed by normal human serum;
Serogroups Z and 29E (Z') are killed by normal human serum;

Meningococci are very exacting to composition of nutritive mediums.
Its reproduction
Meningococci are very exacting to composition of nutritive mediums.
Its reproduction

The agent of meningococcal infection is characterized by low resistance in
The agent of meningococcal infection is characterized by low resistance in
Epidemiology
Meningococcal infections occur worldwide and are notifiable in most countries.
About
Epidemiology
Meningococcal infections occur worldwide and are notifiable in most countries.
About
The incidence of meningococcal infection is increasing. Acute meningitis causes about
The incidence of meningococcal infection is increasing. Acute meningitis causes about
Epidemic strains of group A or group B may give rise
Epidemic strains of group A or group B may give rise
The patients with generalized form are more dangerous.
It is proved
The patients with generalized form are more dangerous.
It is proved
The mechanism of transmission of the infection is air-drop.
The infection
The mechanism of transmission of the infection is air-drop. The infection
In this the narrow contact and sufficient exposition are necessary.
It
It
In meningococcal infection epidemic process is characterized by seasonal spread.
The
In meningococcal infection epidemic process is characterized by seasonal spread.
The
Pathogenesis
In meningococcal infection the entrance gates is mucous membrane of nasopharynx.
Pathogenesis
In meningococcal infection the entrance gates is mucous membrane of nasopharynx.
The stages of inculcation on the mucous membrane of nasopharynx and
The stages of inculcation on the mucous membrane of nasopharynx and
Meningococci are able to break local barriers with help of factors
Meningococci are able to break local barriers with help of factors
Meningococci penetrate into the blood after break of protective barriers of
Meningococci penetrate into the blood after break of protective barriers of
It may be septic course of meningococcemia with formation of the
It may be septic course of meningococcemia with formation of the

Thus, the meningococci enter into subarachnoid space, multiply and course serous-purulent
Thus, the meningococci enter into subarachnoid space, multiply and course serous-purulent

In the pathogenesis of meningococcal infection toxic and allergic components
In the pathogenesis of meningococcal infection toxic and allergic components

The severe complication may develop as a result of expressive
The severe complication may develop as a result of expressive

Clinical manifestation
Classification of the clinical forms of meningococcal infection:
I. Primarily
Clinical manifestation
Classification of the clinical forms of meningococcal infection:
I. Primarily

II. Generalized forms:
a) meningococcemia: typical, acute meningococcal sepsis; chronic;
b) meningitis; meningoencephalitis;
c)
II. Generalized forms:
a) meningococcemia: typical, acute meningococcal sepsis; chronic;
b) meningitis; meningoencephalitis;
c)

Meningococcal nasopharyngitis
The most common complains of the a patients are headache,
Meningococcal nasopharyngitis
The most common complains of the a patients are headache,
Meningococcal nasopharyngitis
There are hyperemia and edema of the mucous membrane of
Meningococcal nasopharyngitis
There are hyperemia and edema of the mucous membrane of
Meningitis
It may start after meningococcal nasopharyngitis, but sometimes primary symptoms
Meningitis
It may start after meningococcal nasopharyngitis, but sometimes primary symptoms
Temperature increases quickly with chill and may reach 40-41° for few
Temperature increases quickly with chill and may reach 40-41° for few
The disorders of consciousness occupy the great place in the clinical
The disorders of consciousness occupy the great place in the clinical
The fulminant course of meningitis with syndrome of brain swelling and
The fulminant course of meningitis with syndrome of brain swelling and
Meningococcemia (meningococcal sepsis).
The disease is more impetuous, with symptoms of toxicosis
Meningococcemia (meningococcal sepsis).
The disease is more impetuous, with symptoms of toxicosis






Exanthema is more clear, constant and diagnostically valuable sign of meningococcemia.
Exanthema is more clear, constant and diagnostically valuable sign of meningococcemia.

The deep and extensive hemorrhages may be necrotic. Then it may
The deep and extensive hemorrhages may be necrotic. Then it may
Laboratory diagnostic
Specific methods
Bacteriological method
Material for bacteriological examination - a smear of
Laboratory diagnostic
Specific methods
Bacteriological method
Material for bacteriological examination - a smear of
The examination of cerebrospinal fluid (CSF) has the great meaning in
The examination of cerebrospinal fluid (CSF) has the great meaning in
Treatment
The therapeutic tactics depends on the clinical forms.
In the moderate
Treatment
The therapeutic tactics depends on the clinical forms.
In the moderate

In the therapy of generalized forms of meningococcal infection used Benzylpenicillin
In the therapy of generalized forms of meningococcal infection used Benzylpenicillin

Daily dose is injected to the patient every 3 hours. In
Daily dose is injected to the patient every 3 hours. In

If pleocytosis more than 100 cells in 1 mcl or predominate
If pleocytosis more than 100 cells in 1 mcl or predominate
 Заболевание глаукома
Заболевание глаукома Хирургические заболевания головы
Хирургические заболевания головы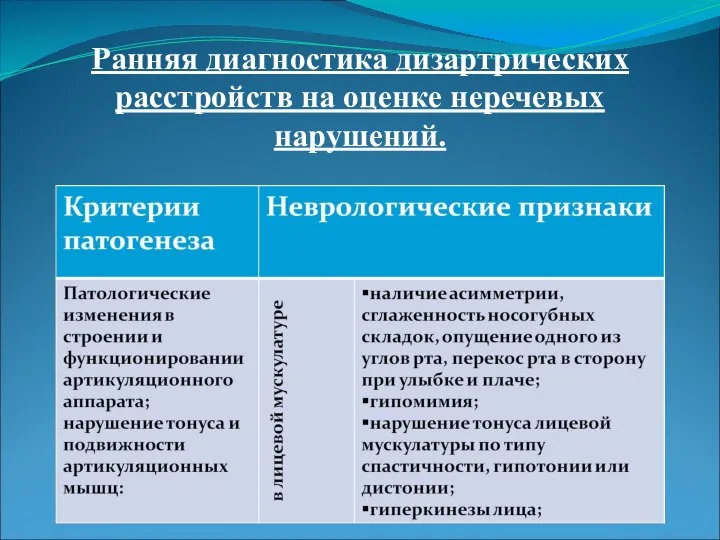 Ранняя диагностика дизартрических расстройств на оценке неречевых нарушений
Ранняя диагностика дизартрических расстройств на оценке неречевых нарушений Беседа о гипер и гипогликемических состояниях
Беседа о гипер и гипогликемических состояниях Temporary fillings
Temporary fillings Тест. Який ти друг !
Тест. Який ти друг ! Лучевая диагностика заболеваний сердечно-сосудистой системы
Лучевая диагностика заболеваний сердечно-сосудистой системы Сүт безінің қатерлі және қатерсіз ісігі
Сүт безінің қатерлі және қатерсіз ісігі УЗИ диагностика заболеваний печени
УЗИ диагностика заболеваний печени Амбулаториялық - емханалық көмекті ұйымдастыру мәселелері
Амбулаториялық - емханалық көмекті ұйымдастыру мәселелері Особенности лечения переломов при остеопорозе
Особенности лечения переломов при остеопорозе Opioid (narcotic) analgesics and antagonists. Non-opioid (non-narcotic) analgesics
Opioid (narcotic) analgesics and antagonists. Non-opioid (non-narcotic) analgesics Психологические особенности личности серийного убийцы
Психологические особенности личности серийного убийцы Инструментальные методы исследование сердечно-сосудистой системы у детей
Инструментальные методы исследование сердечно-сосудистой системы у детей Кровь. Состав крови
Кровь. Состав крови Запоры у детей – кто виноват и что делать
Запоры у детей – кто виноват и что делать Анализ статей и их критическая оценка. Специальность: психиатрия и наркология
Анализ статей и их критическая оценка. Специальность: психиатрия и наркология Виды аптечек
Виды аптечек Преэклампсия. Эклампсия. Лечение. Профилактика
Преэклампсия. Эклампсия. Лечение. Профилактика Детские инфекции у детей: дифтерия, менингококковая инфекция
Детские инфекции у детей: дифтерия, менингококковая инфекция Всемирный день борьбы со СПИДом
Всемирный день борьбы со СПИДом Абсцессы легких. Эмпиемы плевры
Абсцессы легких. Эмпиемы плевры Сектор по вопросам пропаганды здорового образа жизни в ГБПОУ Самарский медицинский колледж им. Н. Ляпиной
Сектор по вопросам пропаганды здорового образа жизни в ГБПОУ Самарский медицинский колледж им. Н. Ляпиной Нейротропные средства. Лекарственные средства, влияющие αφφερεητηυιο иннервацию
Нейротропные средства. Лекарственные средства, влияющие αφφερεητηυιο иннервацию Ќан препараттары жјне ќан ќўюдыѕ ќазіргі заманауи јдістері
Ќан препараттары жјне ќан ќўюдыѕ ќазіргі заманауи јдістері Внебольничная пневмония
Внебольничная пневмония Спонтанный пневмоторакс
Спонтанный пневмоторакс Мужской климакс
Мужской климакс