- Osteoporosis - Diagnosis and Treatment

Содержание
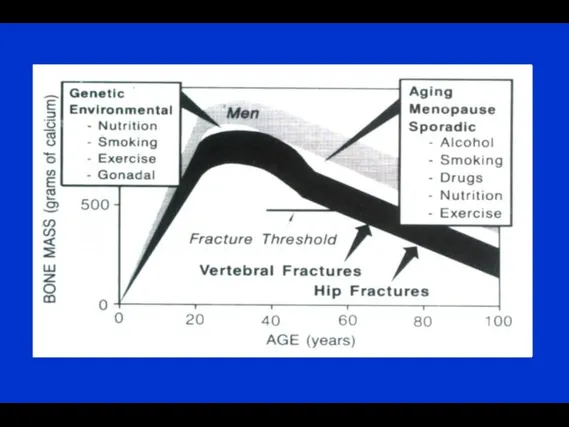
- 3. Osteoporosis Important cause of mortality and morbidity A disease that causes bones to lose mass, weaken
- 4. Incidence of First and Repeat Low-Trauma Fracture in Men and Women by Age Group ? in
- 5. Vertebral fractures Osteoporotic fractures
- 6. 100 % Patients with vertebral fractures that are visible on X-rays 50 % Symptomatic (dorsalgia) 33
- 7. Osteoporotic fractures Colle’s Fracture
- 8. Hip fractures Osteoporotic fractures
- 9. Hip fracture is a deadly condition J. Kanis et al, 2003
- 10. Bone remodelling Quiescence Activation Resorption Formation Quiescence Osteoclasts Osteoblasts Lining cells Mineralized bone Mineralization Bone structural
- 12. Osteoporosis - Causes Menstrual status early menopause (before the age of 45 years) previous amenorrhea (e.g.,
- 13. Glucocorticoid Induced Osteoporosis ? GI Calcium Absorption ? Urinary Calcium Excretion ? LH, FSH, Testosteron, Estrogen
- 14. Osteoporosis - Causes Endocrine disease primary hyperparathryroidism thyrotoxicosis Cushing’s syndrome Rheumatologic diseases rheumatoid arthritis ankylosing spondylitis
- 15. Osteoporosis - Causes Hematologic disease multiple myeloma systemic mastocytosis lymphoma, leukemia pernicious anemia Gastrointestinal diseases malabsorption
- 16. Dual-energy X-ray Absorptiometry - Photons’ source Photons’ source Photons’ beam Collector
- 17. Definition of Osteoporosis in Women According to WHO (diagnostic criteria) Kanis et al Osteoporos Int (1997)7:390-406
- 18. Interpretation failure: a “non-osteoporotic” 89 y old lady with a fractured right femoral neck
- 19. Fracture Risk Calculator FRAX Israel
- 20. Management of osteoporosis: pharmacological therapy Calcium Vitamin D HRT SERMs ( Raloxifen, Evista) Bisphosphonates Denosumab PTH
- 21. Rickets Vit D deficiency in adults: Osteomalacia Fractures Bone pain Muscles pain Difficulties in walking Recommended
- 23. Definition of Vitamin D Status for Multiple Health Outcomes M. Holick 2007 M Parfitt, 1970 Treatment
- 24. Antiresorptive Drugs antiresorptive drugs (estrogen, SERMS, bisphosphonates) ↓ both the rates of bone resorption (in weeks)
- 25. SERMs- Mechanism of Action Acts as Estrogen in bone, decreases incidence of the first vertebral fracture
- 26. Bisphosphonates: Pharmacology Bone-seeking Effective orally or IV Poor absorption orally Not metabolized, excreted by the kidney
- 27. Bisphosphonates: Mechanism of Action Reduce activity of individual osteoclasts • inhibit lysosomal enzymes • inhibit lactate
- 28. Bisphosphonates: Indications and Contraindications Indications Prevention of bone loss in recently menopausal women Treatment of established
- 29. Fracture Intervention Trial (FIT) **P Black DM et al, Lancet 1996;348:1535. © by The Lancet Ltd
- 30. ACLASTA® HAS PROVEN FRACTURE RISK REDUCTION AT ALL 3 KEYS OSTEOPOROSIS SITES DURING 3 YEARS2 2.
- 31. ACLASTA HAS PROVEN TO REDUCE NEW CLINICAL FRACTURES DURING 3 YEARS AND ALL-CAUSE MORTALITY AFTER A
- 32. Denosumab Mechanism of Action © 2007 Amgen. All rights reserved. RANKL RANK OPG Denosumab Bone Formation
- 33. Bone Turnover Markers with Denosumab http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ReproductiveHealthDrugsAdvisoryCommittee/UCM176623.pdf
- 34. The Effect of Denosumab on Fracture Risks at 36 Months Phase 3: The FREEDOM Trial Cummings
- 35. Anabolic Window with Teriparatide Rubin, Bilezikian, 2003. stimulate bone formation overfill resorption cavities the increase in
- 36. Comparison of BMD Changes During Treatment with PTH 1-34 or Fosalan
- 37. Effect of PTH1–34 on Vertebral Fracture Risk Kraenzlin, M. E. & Meier, C. (2011) Parathyroid hormone
- 38. Teriparatide Reduces the Risk of Nonvertebral Fragility Fractures* Placebo (n=544) TPTD20 (n=541) % of Women With
- 39. Teriparatide Improves Skeletal Architecture Patient treated with teriparatide 20µg Female, age 65 Duration of therapy: 637
- 41. Скачать презентацию

Osteoporosis
Important cause of mortality and morbidity
A disease that causes bones to
Osteoporosis
Important cause of mortality and morbidity
A disease that causes bones to
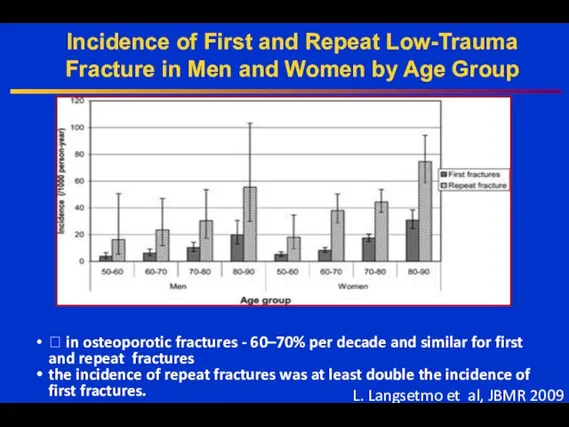
Incidence of First and Repeat Low-Trauma Fracture in Men and Women
Incidence of First and Repeat Low-Trauma Fracture in Men and Women
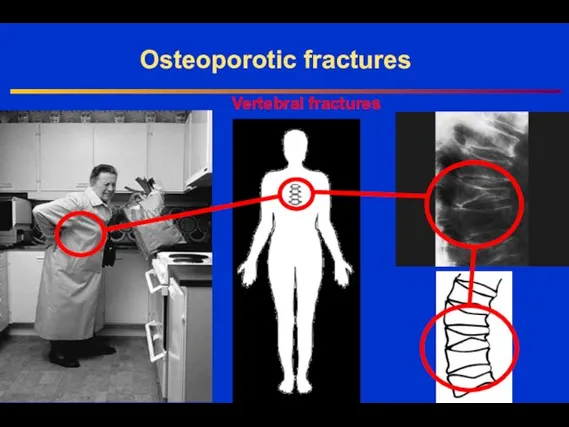
Vertebral fractures
Osteoporotic fractures
Vertebral fractures
Osteoporotic fractures
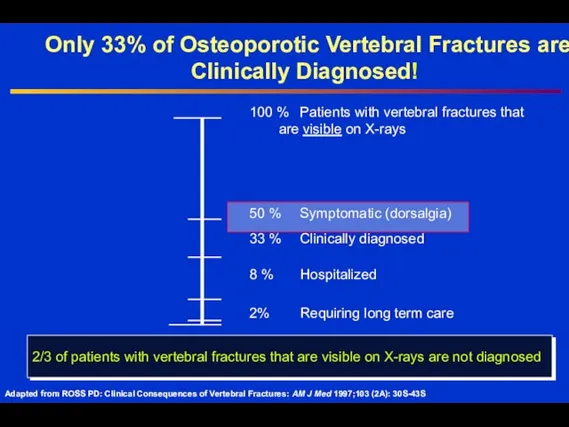
100 % Patients with vertebral fractures that
are visible on
100 % Patients with vertebral fractures that
are visible on
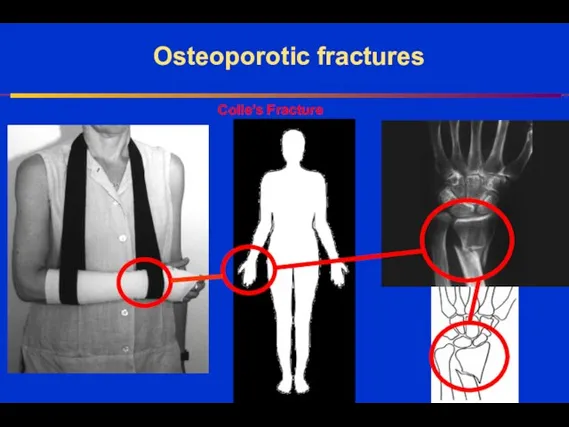
Osteoporotic fractures
Colle’s Fracture
Osteoporotic fractures
Colle’s Fracture
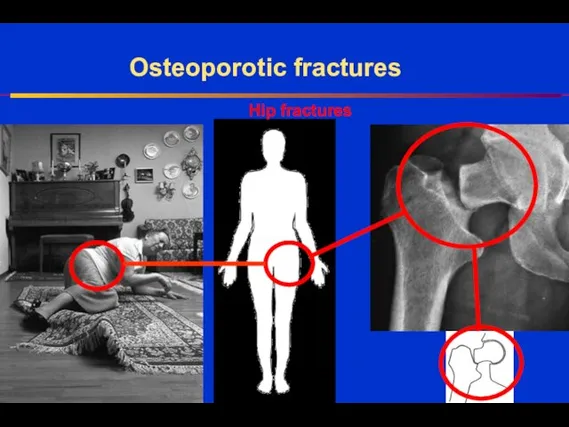
Hip fractures
Osteoporotic fractures
Hip fractures
Osteoporotic fractures
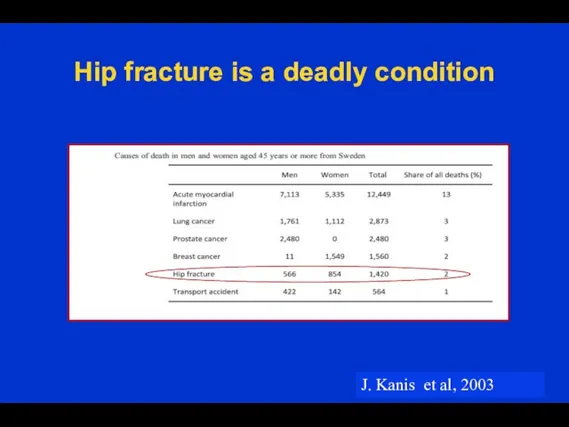
Hip fracture is a deadly condition
J. Kanis et al, 2003
Hip fracture is a deadly condition
J. Kanis et al, 2003
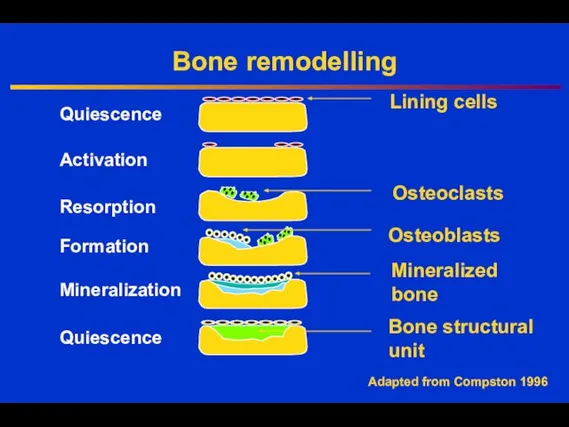
Bone remodelling
Quiescence
Activation
Resorption
Formation
Quiescence
Osteoclasts
Osteoblasts
Lining cells
Mineralized
bone
Mineralization
Bone structural
unit
Adapted from Compston 1996
Bone remodelling
Quiescence
Activation
Resorption
Formation
Quiescence
Osteoclasts
Osteoblasts
Lining cells
Mineralized
bone
Mineralization
Bone structural
unit
Adapted from Compston 1996
Osteoporosis - Causes
Menstrual status
early menopause (before the age of 45 years)
previous
Osteoporosis - Causes
Menstrual status
early menopause (before the age of 45 years)
previous
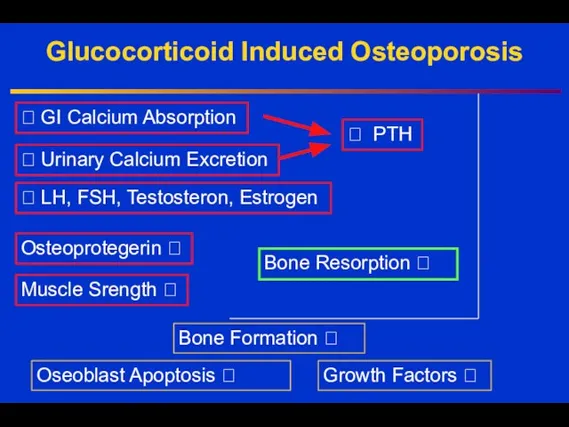
Glucocorticoid Induced Osteoporosis
? GI Calcium Absorption
? Urinary Calcium Excretion
? LH, FSH,
Glucocorticoid Induced Osteoporosis
? GI Calcium Absorption
? Urinary Calcium Excretion
? LH, FSH,
Osteoporosis - Causes
Endocrine disease
primary hyperparathryroidism
thyrotoxicosis
Cushing’s syndrome
Rheumatologic diseases
rheumatoid arthritis
ankylosing spondylitis
Osteoporosis - Causes
Endocrine disease
primary hyperparathryroidism
thyrotoxicosis
Cushing’s syndrome
Rheumatologic diseases
rheumatoid arthritis
ankylosing spondylitis
Osteoporosis - Causes
Hematologic disease
multiple myeloma
systemic mastocytosis
lymphoma, leukemia
pernicious anemia
Gastrointestinal diseases
malabsorption syndromes (e.g.,
Osteoporosis - Causes
Hematologic disease
multiple myeloma
systemic mastocytosis
lymphoma, leukemia
pernicious anemia
Gastrointestinal diseases
malabsorption syndromes (e.g.,
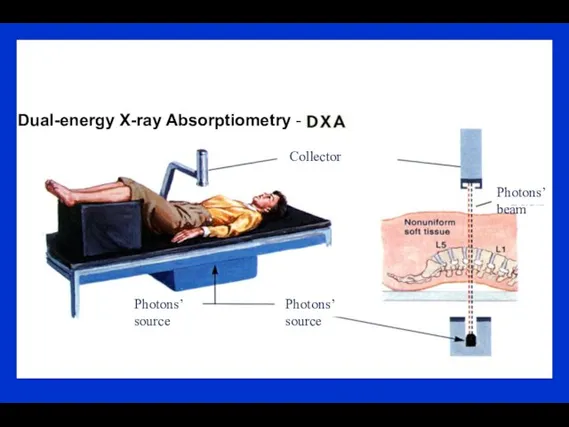
Dual-energy X-ray Absorptiometry -
Photons’ source
Photons’ source
Photons’ beam
Collector
Dual-energy X-ray Absorptiometry -
Photons’ source
Photons’ source
Photons’ beam
Collector
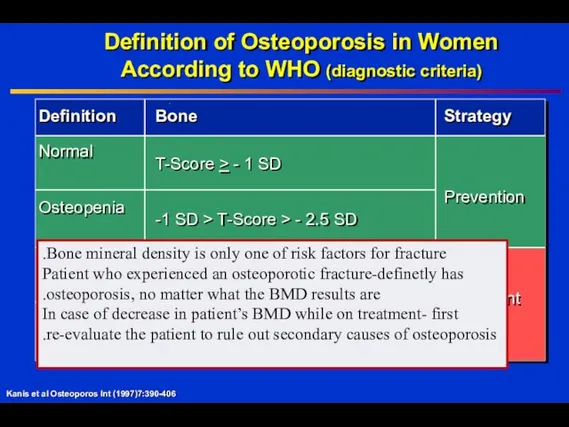
Definition of Osteoporosis in Women
According to WHO (diagnostic criteria)
Kanis et al
Definition of Osteoporosis in Women
According to WHO (diagnostic criteria)
Kanis et al
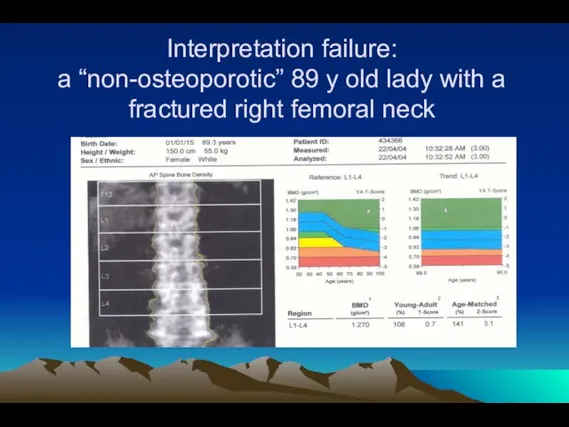
Interpretation failure:
a “non-osteoporotic” 89 y old lady with a fractured right
Interpretation failure: a “non-osteoporotic” 89 y old lady with a fractured right
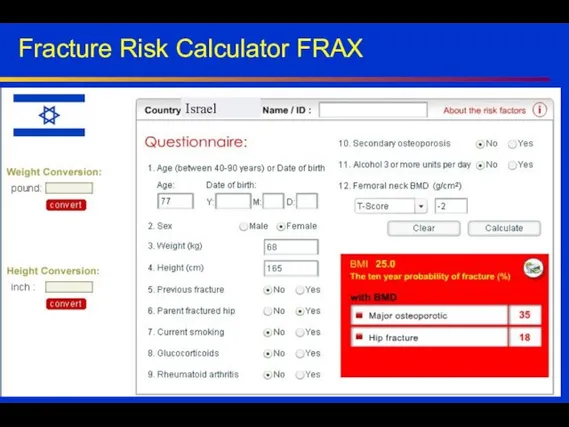
Fracture Risk Calculator FRAX
Israel
Fracture Risk Calculator FRAX
Israel
Management of osteoporosis:
pharmacological therapy
Calcium
Vitamin D
HRT
SERMs ( Raloxifen, Evista)
Bisphosphonates
Denosumab
PTH
HT (not recommended
Management of osteoporosis:
pharmacological therapy
Calcium
Vitamin D
HRT
SERMs ( Raloxifen, Evista)
Bisphosphonates
Denosumab
PTH
HT (not recommended
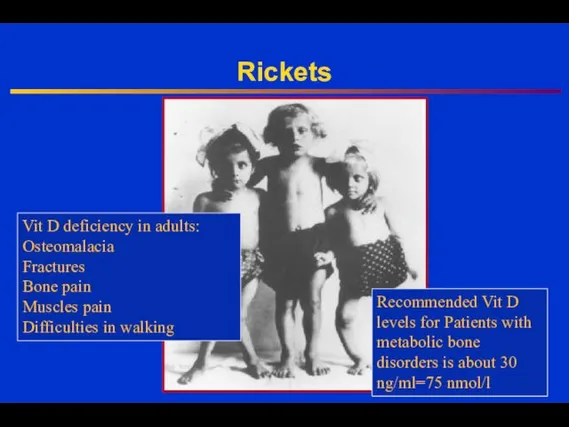
Rickets
Vit D deficiency in adults:
Osteomalacia
Fractures
Bone pain
Muscles pain
Difficulties in walking
Recommended Vit
Rickets
Vit D deficiency in adults:
Osteomalacia
Fractures
Bone pain
Muscles pain
Difficulties in walking
Recommended Vit

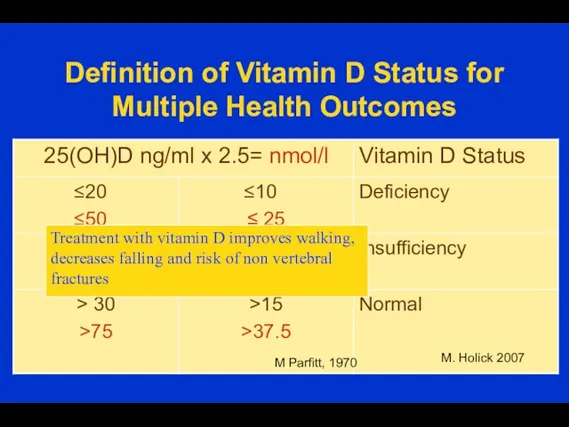
Definition of Vitamin D Status for Multiple Health Outcomes
M. Holick
Definition of Vitamin D Status for Multiple Health Outcomes
M. Holick
Antiresorptive Drugs
antiresorptive drugs (estrogen, SERMS, bisphosphonates) ↓ both the rates of
Antiresorptive Drugs
antiresorptive drugs (estrogen, SERMS, bisphosphonates) ↓ both the rates of
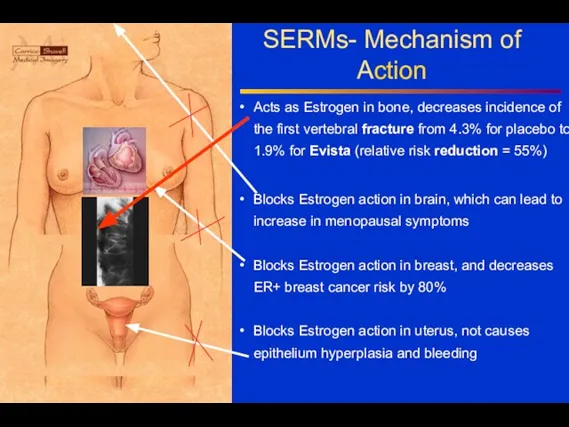
SERMs- Mechanism of Action
Acts as Estrogen in bone, decreases incidence of
SERMs- Mechanism of Action
Acts as Estrogen in bone, decreases incidence of
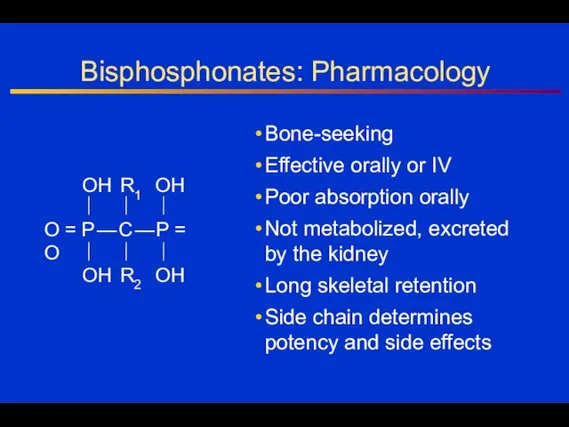
Bisphosphonates: Pharmacology
Bone-seeking
Effective orally or IV
Poor absorption orally
Not metabolized, excreted
by the kidney
Long
Bisphosphonates: Pharmacology
Bone-seeking
Effective orally or IV
Poor absorption orally
Not metabolized, excreted
by the kidney
Long
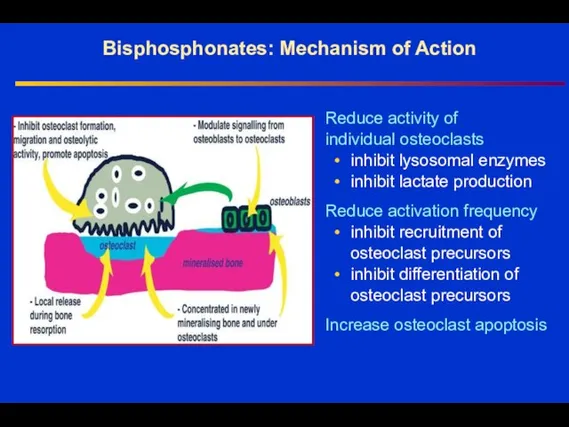
Bisphosphonates: Mechanism of Action
Reduce activity of
individual osteoclasts
• inhibit lysosomal enzymes
• inhibit
Bisphosphonates: Mechanism of Action
Reduce activity of
individual osteoclasts
• inhibit lysosomal enzymes
• inhibit
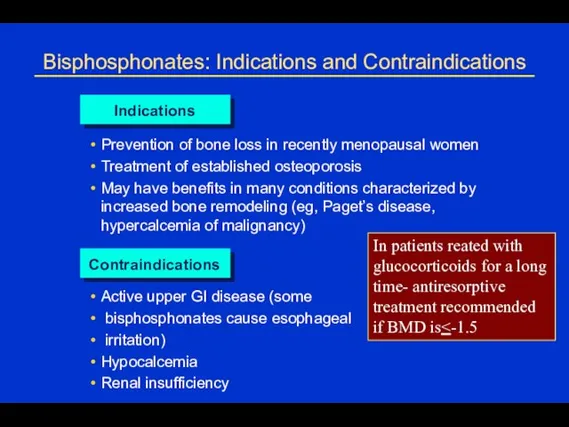
Bisphosphonates: Indications and Contraindications
Indications
Prevention of bone loss in recently menopausal women
Treatment
Bisphosphonates: Indications and Contraindications
Indications
Prevention of bone loss in recently menopausal women
Treatment
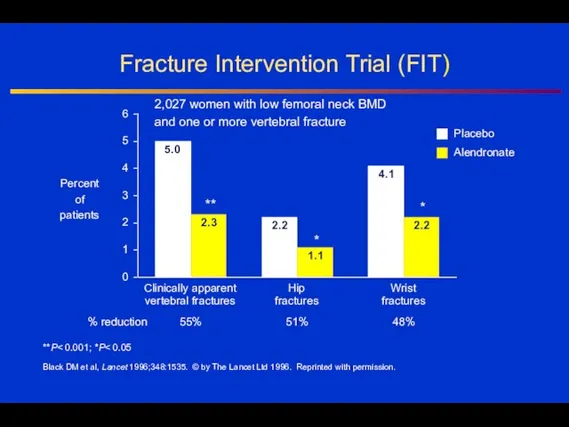
Fracture Intervention Trial (FIT)
**P< 0.001; *P< 0.05
Black DM et al, Lancet
Fracture Intervention Trial (FIT)
**P< 0.001; *P< 0.05
Black DM et al, Lancet
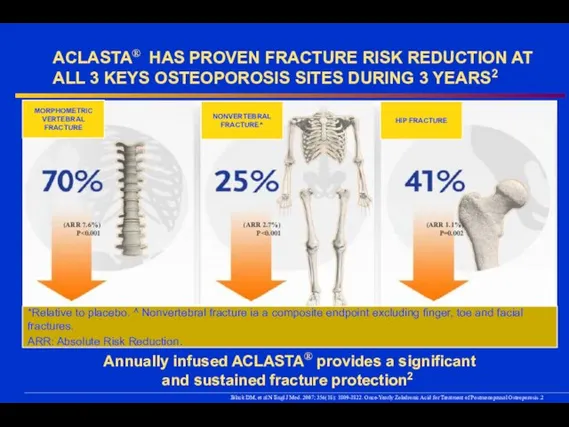
ACLASTA® HAS PROVEN FRACTURE RISK REDUCTION AT ALL 3 KEYS OSTEOPOROSIS
ACLASTA® HAS PROVEN FRACTURE RISK REDUCTION AT ALL 3 KEYS OSTEOPOROSIS
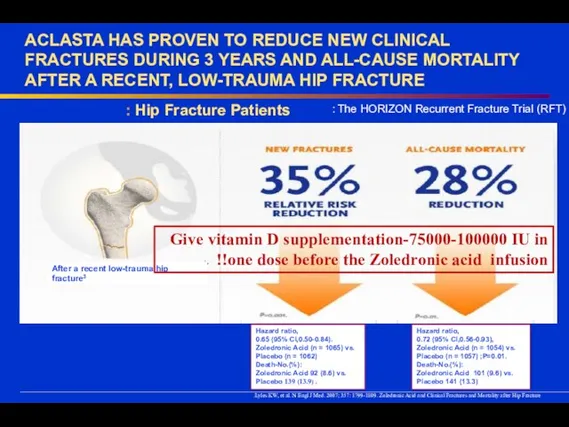
ACLASTA HAS PROVEN TO REDUCE NEW CLINICAL FRACTURES DURING 3 YEARS
ACLASTA HAS PROVEN TO REDUCE NEW CLINICAL FRACTURES DURING 3 YEARS
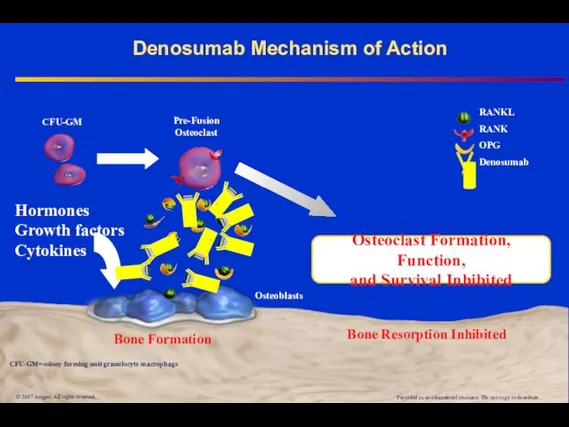
Denosumab Mechanism of Action
© 2007 Amgen. All rights reserved.
RANKL
RANK
OPG
Denosumab
Bone Formation
Hormones
Growth factors
Cytokines
Bone
Denosumab Mechanism of Action
© 2007 Amgen. All rights reserved.
RANKL
RANK
OPG
Denosumab
Bone Formation
Hormones
Growth factors
Cytokines
Bone
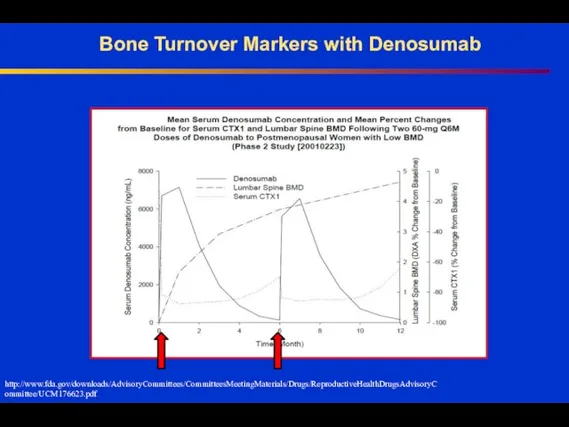
Bone Turnover Markers with Denosumab
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ReproductiveHealthDrugsAdvisoryCommittee/UCM176623.pdf
Bone Turnover Markers with Denosumab
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ReproductiveHealthDrugsAdvisoryCommittee/UCM176623.pdf
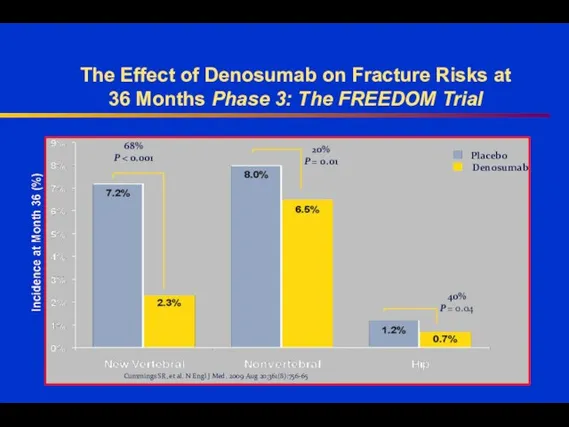
The Effect of Denosumab on Fracture Risks at
36 Months Phase
The Effect of Denosumab on Fracture Risks at 36 Months Phase
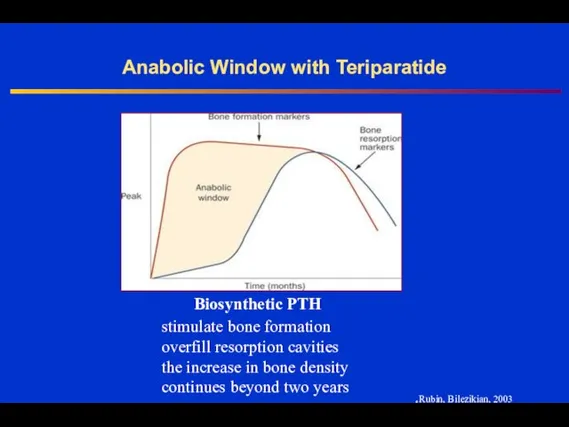
Anabolic Window with Teriparatide
Rubin, Bilezikian, 2003.
stimulate bone formation
overfill resorption cavities
the
Anabolic Window with Teriparatide
Rubin, Bilezikian, 2003.
stimulate bone formation
overfill resorption cavities
the
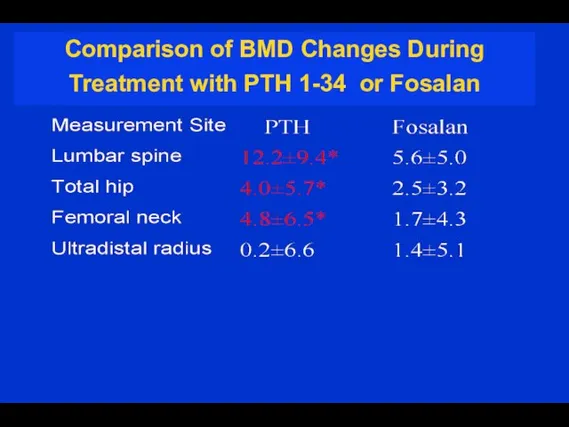
Comparison of BMD Changes During Treatment with PTH 1-34 or Fosalan
Comparison of BMD Changes During Treatment with PTH 1-34 or Fosalan
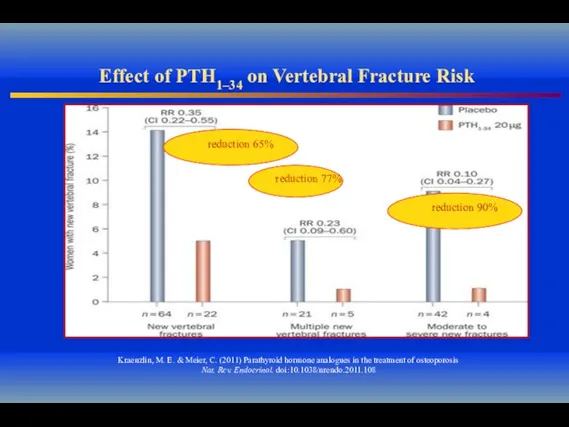
Effect of PTH1–34 on Vertebral Fracture Risk
Kraenzlin, M. E. & Meier,
Effect of PTH1–34 on Vertebral Fracture Risk
Kraenzlin, M. E. & Meier,
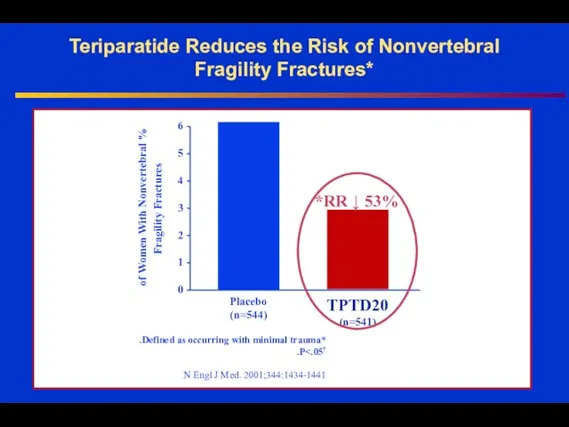
Teriparatide Reduces the Risk of Nonvertebral Fragility Fractures*
Placebo
(n=544)
TPTD20
(n=541)
% of Women
Teriparatide Reduces the Risk of Nonvertebral Fragility Fractures*
Placebo
(n=544)
TPTD20
(n=541)
% of Women
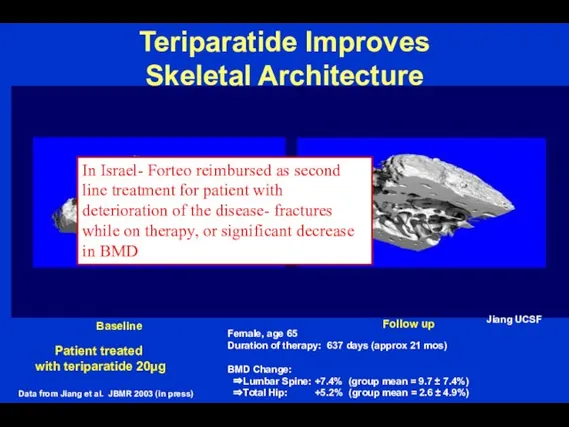
Teriparatide Improves
Skeletal Architecture
Patient treated
with teriparatide 20µg
Female, age 65
Duration of therapy:
Teriparatide Improves
Skeletal Architecture
Patient treated
with teriparatide 20µg
Female, age 65
Duration of therapy:
 Психосоматичні розлади: поняття та класифікація
Психосоматичні розлади: поняття та класифікація Осложнения после удаления зуба
Осложнения после удаления зуба Клиническая картина сагиттальных отклонений прикуса
Клиническая картина сагиттальных отклонений прикуса Врожденная непроходимость желудочно-кишечного тракта
Врожденная непроходимость желудочно-кишечного тракта Назначение целевого и результативного компонентов системы психолого-педагогического сопровождения
Назначение целевого и результативного компонентов системы психолого-педагогического сопровождения Многоплодная беременность
Многоплодная беременность Гигиена кожи
Гигиена кожи Методы обследования слезных органов
Методы обследования слезных органов Тыныс жетіспеушілігінің диагностикасы және емі
Тыныс жетіспеушілігінің диагностикасы және емі Аллергодерматозы
Аллергодерматозы Рентген диагностика заболеваний молочной железы
Рентген диагностика заболеваний молочной железы Доступ к материалам по методикам лечения переломов Surgery Reference на AO сайте
Доступ к материалам по методикам лечения переломов Surgery Reference на AO сайте Вирус СПИДа
Вирус СПИДа Гайморит у детей
Гайморит у детей Норма и патология речи. Речевое поведение. Эмоциональность, скорость и громкость речи
Норма и патология речи. Речевое поведение. Эмоциональность, скорость и громкость речи Адгезия. Условия адгезии. Стандартизация стоматологических материалов
Адгезия. Условия адгезии. Стандартизация стоматологических материалов Технологии развития произвольности внимания в подростковом и взрослом возрасте
Технологии развития произвольности внимания в подростковом и взрослом возрасте Витамин D
Витамин D Фенотипическая классификация первичных иммунодефицитов
Фенотипическая классификация первичных иммунодефицитов Талмажәне талма кезінде алғашқы көмек
Талмажәне талма кезінде алғашқы көмек Послеоперационное обезболивание
Послеоперационное обезболивание Интерлейкины. Перспективы биотехнологического производства и практическое применение
Интерлейкины. Перспективы биотехнологического производства и практическое применение АЧС. Медецина
АЧС. Медецина Рентгенологиялық және эндоскопиялық зерттеу әдістері
Рентгенологиялық және эндоскопиялық зерттеу әдістері Цитомегаловирусты, герпестік, хламидиялық инфекция және жүктілік
Цитомегаловирусты, герпестік, хламидиялық инфекция және жүктілік Биологические вредные и опасные производственные факторы. Классификация заболеваний, вызываемых БОиВПФ
Биологические вредные и опасные производственные факторы. Классификация заболеваний, вызываемых БОиВПФ Профилактика синдрома профессионального выгорания
Профилактика синдрома профессионального выгорания Генитальный герпес
Генитальный герпес