- Surgical Neonatal Vomiting

Содержание
- 2. Interactive Case studies Summary of specific surgical conditions
- 3. What is a neonate? What is preterm? What is term?
- 4. Definitions Neonate – premature and term babies less that 44 weeks post-conceptional age Premature neonate Term
- 5. History and Symptoms
- 6. History and Symptoms Gestation Weight Antenatal history Colour of vomit Frequency of vomit Bowel opening Saliva?
- 7. Physical Findings
- 8. Physical findings Observations Erythema and bruising Distended Scaphoid abdomen Mass Anus – site, size and patency
- 9. Investigations Plain AXR/CXR Upper/Lower GI contrast Abdominal USS
- 10. Case 1 Term neonate 1 day old Vomiting Relevant points in history Relevant examination findings Differential
- 12. Oesophageal atresia and tracheo-oesophageal fistula 1 in 3500 liveborn births Antenatal Polyhydramnios, absent stomach, associated anomalies
- 13. Classification Type A: 8%, Type B: 1%, Type C: 86%, Type D 1%, Type E: 4%
- 14. Repair Right thoracotomy (usually) 4th or 5th intercoastal space Extrapleural approach +/- division of azygous vein
- 18. Duodenal Atresia 1 in 5000 Antenatal diagnosis – ‘double bubble’ Associated with Trisomy 21 - 30%,
- 20. Malrotation +/- volvulus
- 21. Malrotation 1 in 6000 present in babies 0.5% of autopsies show degree of malrotation Abnormal duodenal
- 22. Malrotation + volvulus SURGICAL EMERGENCY Bilious vomiting in neonate Upper GI contrast to diagnose Emergency laparotomy
- 24. Jejunal/Ileal atresia Stenosis – 11% Type 1 – 23% Type 2 – 10% Type 3 –
- 25. Jejunal/ileal atresia 1 in 5000 births Aetiology – antenatal vascular compromise May have short bowel Resection
- 26. Meconium Ileus CF – 1 in 2500 births ~16% of babies with CF Inspissated sticky meconium
- 27. Microcolon in Meconium ileus
- 28. Hirschsprung Disease
- 29. Hirschsprung Disease 1 in 5000 births M:F 4:1 Associated with Trisomy 21 Delayed passage of meconium
- 30. Hirschsprung Disease Aganglionosis of bowel Variable failure of neural crest cell migration Rectosigmoid – 75% Long
- 31. Anorectal malformation
- 32. Anorectal malformation 1 in 4000 births Management depends on level of ARM Primary anoplasty for low
- 33. Case 2 3 week old term baby Relevant points in history Relevant examination findings Differential diagnosis
- 34. Infantile Hypertrophic Pyloric Stenosis 1-4:1000, M:F 4:1 Overgrowth of pyloric muscle Gastric outlet obstruction Increasing non-bilious
- 35. Pyloric stenosis
- 36. Infantile Hypertrophic Pyloric Stenosis Diagnosis – palpable mass on ‘test feed’ USS Pyloric length >16mm Single
- 37. Inguinal hernia
- 38. Inguinal hernia Usually can reduce If truly incacerated – emergency exploration Otherwise if premature baby or
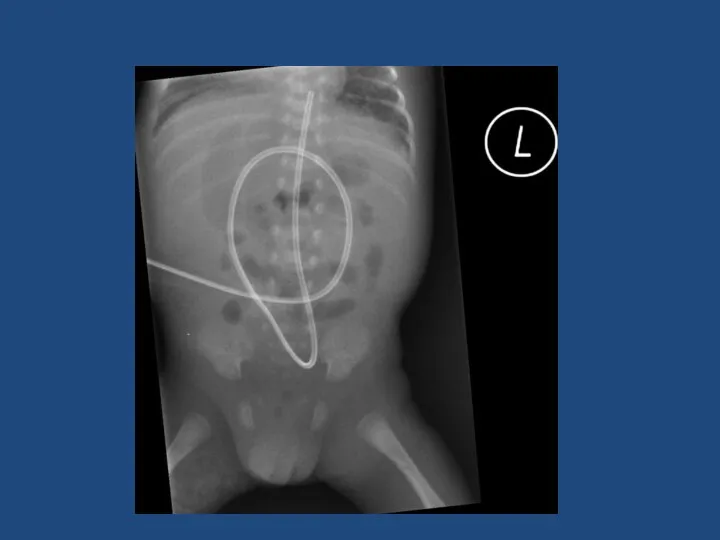
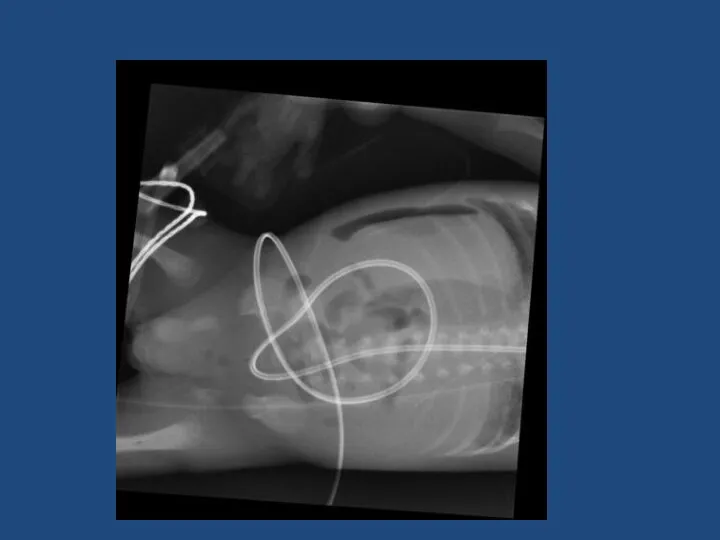
- 39. Case 3 Preterm neonate – bilious vomiting Born 27 weeks gestation Weight 1 kg 1 week
- 43. Necrotising Enterocolitis 90% in preterm 10% in term babies ~5% of all babies admitted to Neonatal
- 44. Necrotising Enterocolitis Surgery indicated for: Worsening clinical condition despite maximal supportive therapy Perforation Laparotomy Assess extent
- 46. Скачать презентацию
Interactive
Case studies
Summary of specific surgical conditions
Interactive
Case studies
Summary of specific surgical conditions
What is a neonate?
What is preterm?
What is term?
What is a neonate?
What is preterm?
What is term?
Definitions
Neonate – premature and term babies less that 44 weeks post-conceptional
Definitions
Neonate – premature and term babies less that 44 weeks post-conceptional
History and Symptoms
History and Symptoms
History and Symptoms
Gestation
Weight
Antenatal history
Colour of vomit
Frequency of vomit
Bowel opening
Saliva?
Associated co-morbidities
History and Symptoms
Gestation
Weight
Antenatal history
Colour of vomit
Frequency of vomit
Bowel opening
Saliva?
Associated co-morbidities

Physical Findings
Physical Findings
Physical findings
Observations
Erythema and bruising
Distended
Scaphoid abdomen
Mass
Anus – site, size and patency
Tenderness
External
Physical findings
Observations
Erythema and bruising
Distended
Scaphoid abdomen
Mass
Anus – site, size and patency
Tenderness
External
Investigations
Plain AXR/CXR
Upper/Lower GI contrast
Abdominal USS
Investigations
Plain AXR/CXR
Upper/Lower GI contrast
Abdominal USS
Case 1
Term neonate
1 day old
Vomiting
Relevant points in history
Relevant examination findings
Differential diagnosis
Case 1
Term neonate
1 day old
Vomiting
Relevant points in history
Relevant examination findings
Differential diagnosis
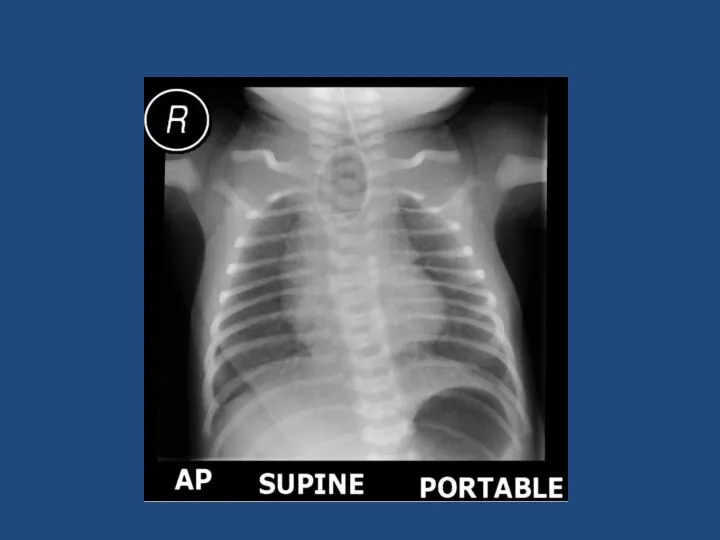
Oesophageal atresia and tracheo-oesophageal fistula
1 in 3500 liveborn births
Antenatal
Polyhydramnios, absent stomach,
Oesophageal atresia and tracheo-oesophageal fistula
1 in 3500 liveborn births
Antenatal
Polyhydramnios, absent stomach,
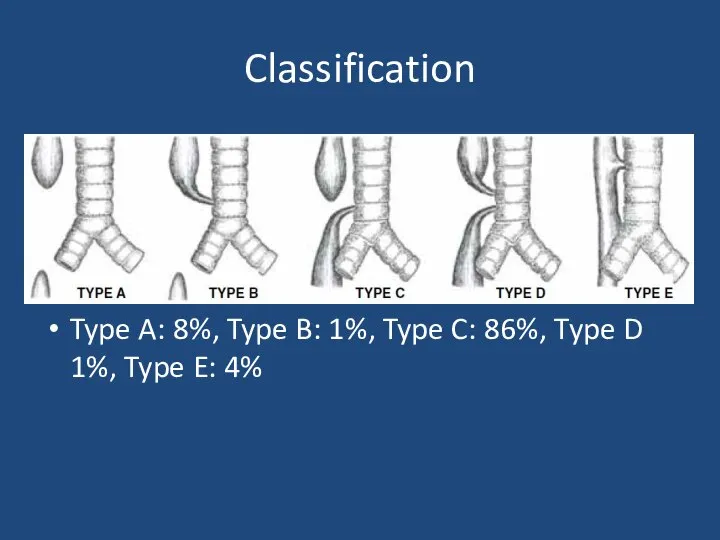
Classification
Type A: 8%, Type B: 1%, Type C: 86%, Type D
Classification
Type A: 8%, Type B: 1%, Type C: 86%, Type D
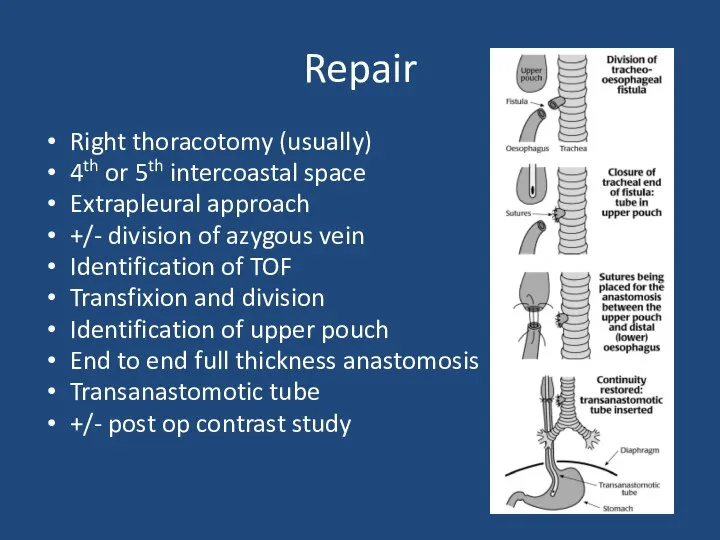
Repair
Right thoracotomy (usually)
4th or 5th intercoastal space
Extrapleural approach
+/- division of azygous
Repair
Right thoracotomy (usually)
4th or 5th intercoastal space
Extrapleural approach
+/- division of azygous


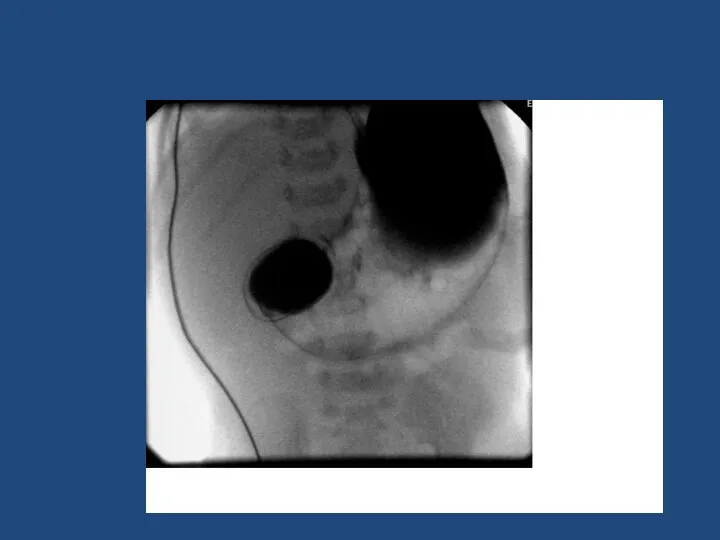
Duodenal Atresia
1 in 5000
Antenatal diagnosis – ‘double bubble’
Associated with Trisomy 21
Duodenal Atresia
1 in 5000
Antenatal diagnosis – ‘double bubble’
Associated with Trisomy 21
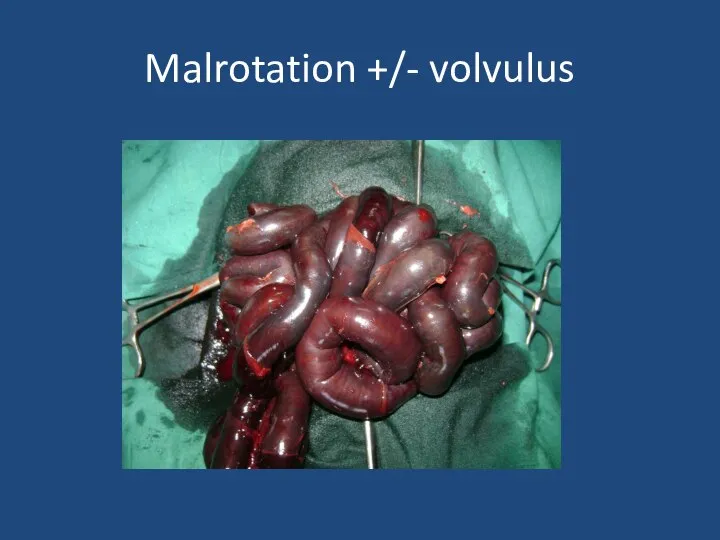
Malrotation +/- volvulus
Malrotation +/- volvulus

Malrotation
1 in 6000 present in babies
0.5% of autopsies show degree of
Malrotation
1 in 6000 present in babies
0.5% of autopsies show degree of
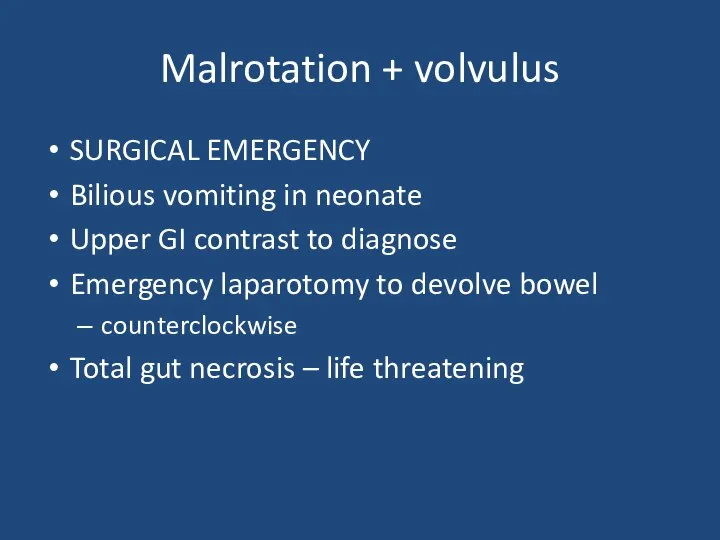
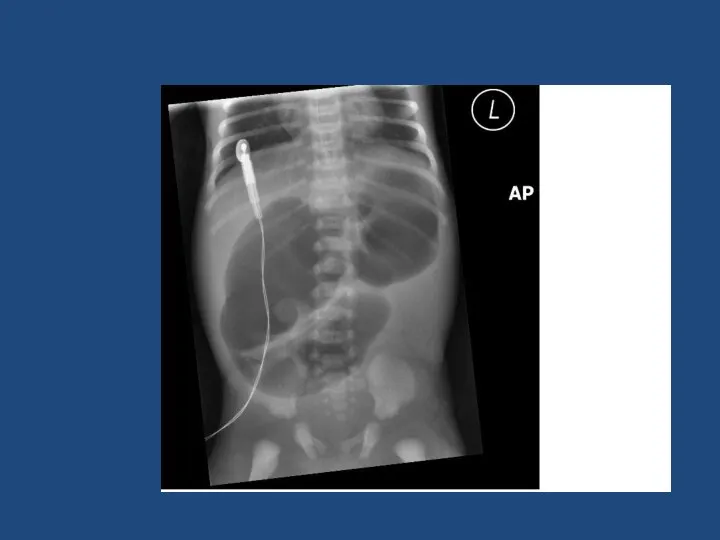
Malrotation + volvulus
SURGICAL EMERGENCY
Bilious vomiting in neonate
Upper GI contrast to
Malrotation + volvulus
SURGICAL EMERGENCY
Bilious vomiting in neonate
Upper GI contrast to
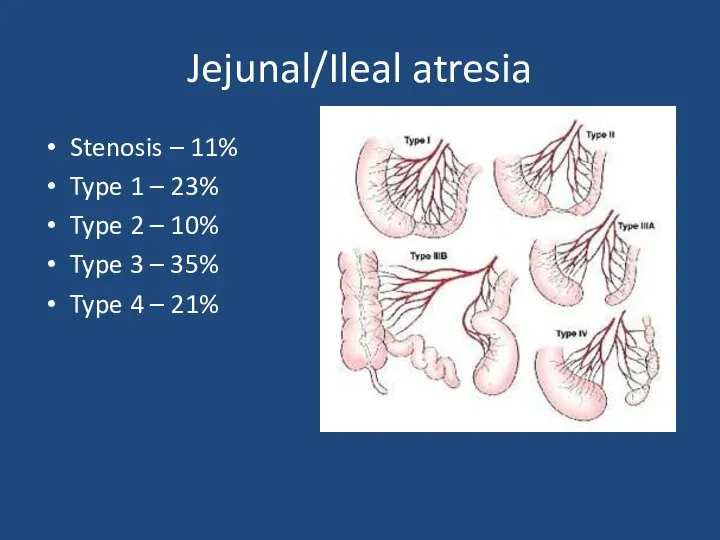
Jejunal/Ileal atresia
Stenosis – 11%
Type 1 – 23%
Type 2 – 10%
Type
Jejunal/Ileal atresia
Stenosis – 11%
Type 1 – 23%
Type 2 – 10%
Type
Jejunal/ileal atresia
1 in 5000 births
Aetiology – antenatal vascular compromise
May have short
Jejunal/ileal atresia
1 in 5000 births
Aetiology – antenatal vascular compromise
May have short
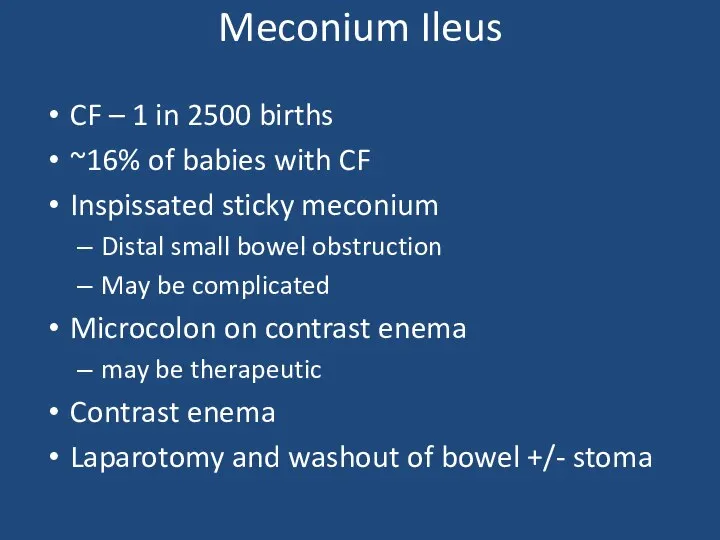
Meconium Ileus
CF – 1 in 2500 births
~16% of babies with CF
Inspissated
Meconium Ileus
CF – 1 in 2500 births
~16% of babies with CF
Inspissated
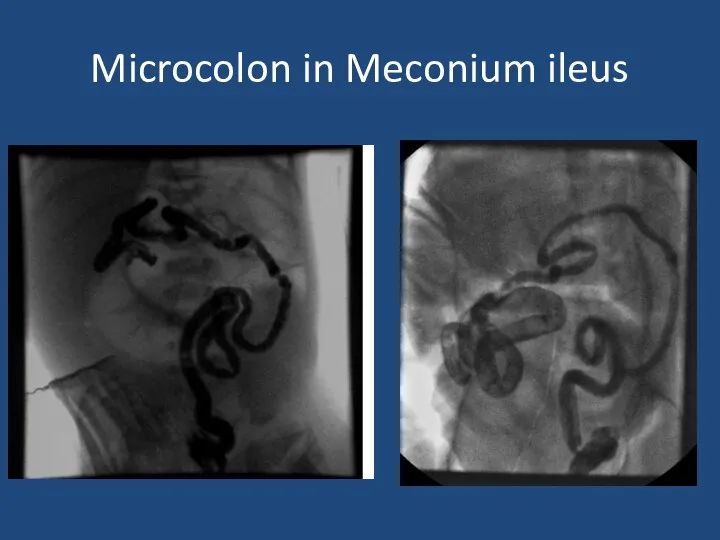
Microcolon in Meconium ileus
Microcolon in Meconium ileus
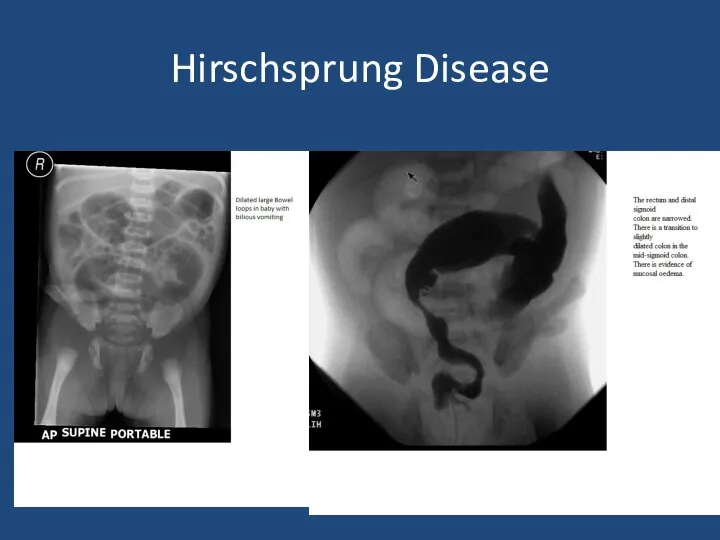
Hirschsprung Disease
Hirschsprung Disease
Hirschsprung Disease
1 in 5000 births
M:F 4:1
Associated with Trisomy 21
Delayed passage of
Hirschsprung Disease
1 in 5000 births
M:F 4:1
Associated with Trisomy 21
Delayed passage of
Hirschsprung Disease
Aganglionosis of bowel
Variable failure of neural crest cell migration
Rectosigmoid –
Hirschsprung Disease
Aganglionosis of bowel
Variable failure of neural crest cell migration
Rectosigmoid –
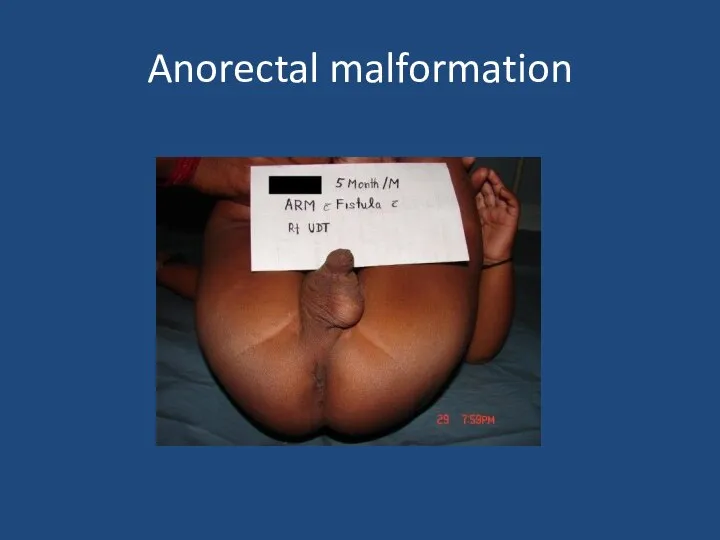
Anorectal malformation
Anorectal malformation
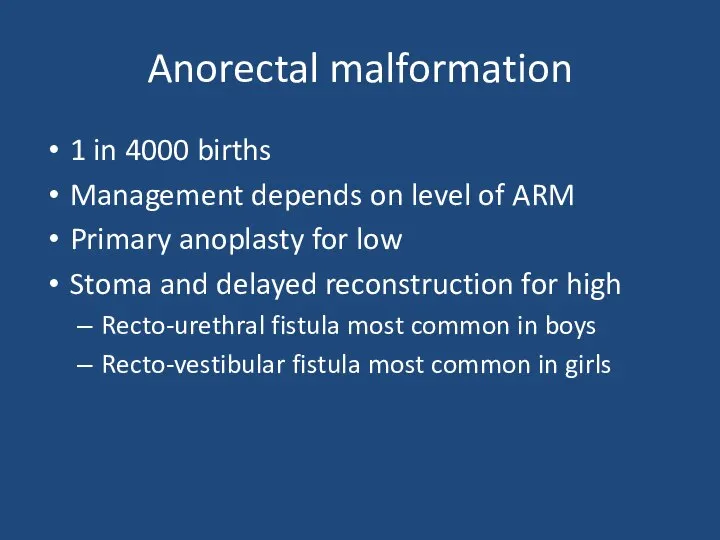
Anorectal malformation
1 in 4000 births
Management depends on level of ARM
Primary anoplasty
Anorectal malformation
1 in 4000 births
Management depends on level of ARM
Primary anoplasty
Case 2
3 week old term baby
Relevant points in history
Relevant examination findings
Differential
Case 2
3 week old term baby
Relevant points in history
Relevant examination findings
Differential
Infantile Hypertrophic Pyloric Stenosis
1-4:1000, M:F 4:1
Overgrowth of pyloric muscle
Gastric outlet obstruction
Increasing
Infantile Hypertrophic Pyloric Stenosis
1-4:1000, M:F 4:1
Overgrowth of pyloric muscle
Gastric outlet obstruction
Increasing
Pyloric stenosis
Pyloric stenosis
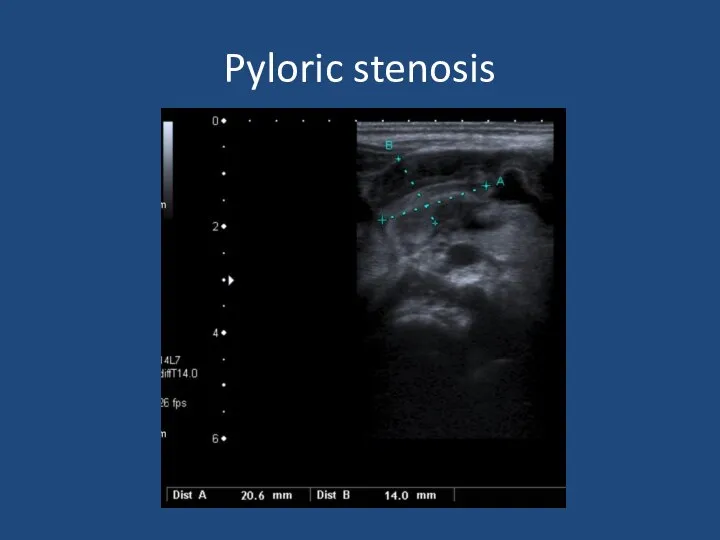
Infantile Hypertrophic Pyloric Stenosis
Diagnosis – palpable mass on ‘test feed’
USS
Pyloric length
Infantile Hypertrophic Pyloric Stenosis
Diagnosis – palpable mass on ‘test feed’
USS
Pyloric length
Inguinal hernia
Inguinal hernia
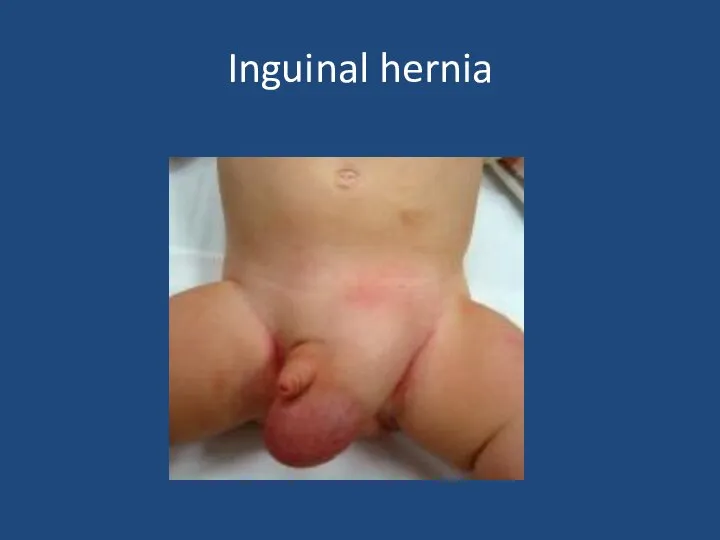
Inguinal hernia
Usually can reduce
If truly incacerated – emergency exploration
Otherwise if premature
Inguinal hernia
Usually can reduce
If truly incacerated – emergency exploration
Otherwise if premature
Case 3
Preterm neonate – bilious vomiting
Born 27 weeks gestation
Weight 1 kg
1
Case 3
Preterm neonate – bilious vomiting
Born 27 weeks gestation
Weight 1 kg
1
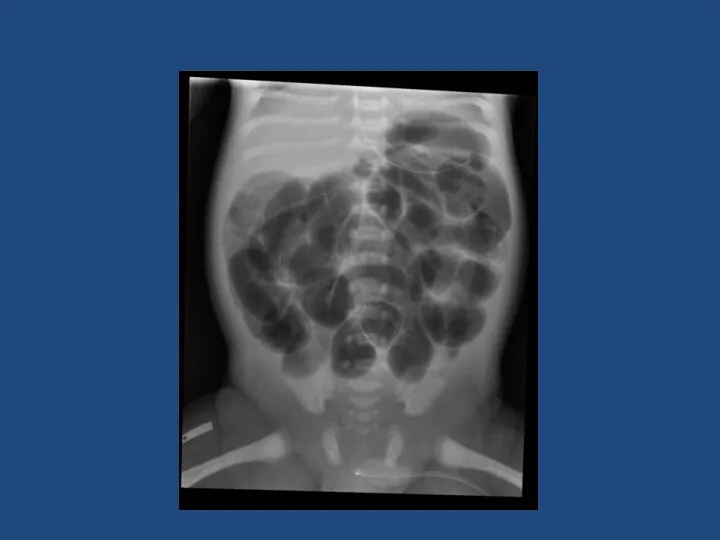
Necrotising Enterocolitis
90% in preterm 10% in term babies
~5% of all babies
Necrotising Enterocolitis
90% in preterm 10% in term babies
~5% of all babies
Necrotising Enterocolitis
Surgery indicated for:
Worsening clinical condition despite maximal supportive therapy
Perforation
Laparotomy
Assess extent
Necrotising Enterocolitis
Surgery indicated for:
Worsening clinical condition despite maximal supportive therapy
Perforation
Laparotomy
Assess extent
 Ультразвук в клинической диагностике глаз и орбиты
Ультразвук в клинической диагностике глаз и орбиты Ортодонтия. Тістем дегеніміз орталық окклюзия жағдайында тістердің түйісуі
Ортодонтия. Тістем дегеніміз орталық окклюзия жағдайында тістердің түйісуі Недоверие и страх системы ОСМС
Недоверие и страх системы ОСМС Влияние антибиотиков на микрофлору
Влияние антибиотиков на микрофлору Сүйек кемігі
Сүйек кемігі Хронические гепатиты, циррозы печени
Хронические гепатиты, циррозы печени Хроническая сердечная недостаточность
Хроническая сердечная недостаточность Сахар и сахарозаменители
Сахар и сахарозаменители Вредное влияние алкоголя, курения и наркотиков в период эмбрионального развития
Вредное влияние алкоголя, курения и наркотиков в период эмбрионального развития Профилактика и ранняя диагностика онкологических заболеваний
Профилактика и ранняя диагностика онкологических заболеваний Уход за пациентами пожилого возраста в стационаре и дома
Уход за пациентами пожилого возраста в стационаре и дома Наркомани. Наркотические средства
Наркомани. Наркотические средства Особенности первичной позитивной профилактики аддиктивного поведения в образовательных учреждениях
Особенности первичной позитивной профилактики аддиктивного поведения в образовательных учреждениях Основные правила рационального питания
Основные правила рационального питания Классный час на тему: Глаза - главные помощники человека. Гигиена зрения. Забота о глазах
Классный час на тему: Глаза - главные помощники человека. Гигиена зрения. Забота о глазах Правила оказания первой помощи при ранениях
Правила оказания первой помощи при ранениях Сознание. Свойства сознания
Сознание. Свойства сознания Методы обследования больного: субъективные и объективные
Методы обследования больного: субъективные и объективные Гистологиялық препараттардың электрондық нұсқасы
Гистологиялық препараттардың электрондық нұсқасы Вірус Зіка
Вірус Зіка Взгляд косметолога на акне и качество кожи лица
Взгляд косметолога на акне и качество кожи лица Тромбоэмболия легочной артерии в акушерской практике
Тромбоэмболия легочной артерии в акушерской практике Профессиональное выгорание педагогов-психологов
Профессиональное выгорание педагогов-психологов Детский церебральный паралич. Клинические симптомы
Детский церебральный паралич. Клинические симптомы Пуринергиялық синапстарда қозудың берілуіне әсер ететін дәрілер
Пуринергиялық синапстарда қозудың берілуіне әсер ететін дәрілер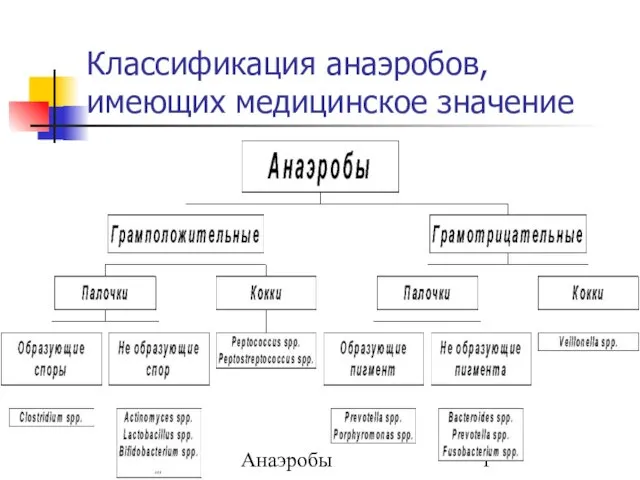 Классификация анаэробов, имеющих медицинское значение
Классификация анаэробов, имеющих медицинское значение Виды медицинского страхования
Виды медицинского страхования Когнитивная психология
Когнитивная психология