- Systemic lupus erythematosus

Содержание
- 2. General characteristics Unknown etiology, multifactorial disease Involve joints, kidneys, mucous membranes, the central nervous system Variety
- 3. Epidemiology Prevalence: 50-100 /100.000 Incidence: 2-7 /100.000/year age at onset: 20-30 Female vs. male ratio: 9-10:1
- 4. Etiology Family history (1st degree relatives 1%) Genetic predisposition MHC genes: HLA DR2,DR3 DR4-DIL, DR5-APS non-MHC
- 5. Etiology Provoking factors Sunlight, UV light Infections Hormonal status:estrogen, prolactin Drugs Isoniacid Hidantoin Hydralazin Procainamid D
- 6. PATHOGENESIS Disturbed immune regulation: Pathologic antigen presentation Increased MHC expression Enhanced co-stimulation Cytokine imbalance (Th1/Th2) Decrease
- 7. Pathogenesis of SLE Provoking factors: Genetics predisposition (MHC and non-MHC genes Triggering factors (UV, drugs, infections)
- 9. Antigen targets for autoantibodies in SLE Nuclear antigens: ssDNA, dsDNA, histon, Sm, RNP Cytoplasmic antigens: SS-A,
- 10. General symptoms Weakness Fatigue Tiredness Fever Weight loss Hair loss Lymphadenopathy
- 11. CLASSIFICATION OF SKIN SYMPTOMS IN SLE (Sontheimer RD.Lupus 6:84-95, 1997) Lupus specific A. Acute cutan LE
- 12. Lupus specific skin symptoms Vespertilio=butterfly rash Acute cutan LE
- 13. Lupus specific skin symptoms DLE SCLE
- 14. Non-lupus specific skin symptoms vasculitis Raynaud phenomenon
- 15. Musculosceletal involvment of lupus Small joint symmetric non erosive polyarthritis Aseptic femur neck necrosis Osteoporosis Myositis
- 16. Polyserositis Pleuritis Pericarditis Peritonitis pleuritis pericarditis
- 17. Respiratory involvment Pleuritis Alveolitis obliterans Pulmonal fibrosis Pulmonal hypertension ARDS Pulmonal embolism
- 18. Cardiovascular involvments Pericarditis Myocarditis Cardiomyopathy Endocarditis non-infectious verrucosus endocarditis (Libman-Sacks endocarditis) subacute infectious endocarditis Valvulopathy Atherosclerosis
- 19. Pericarditis AMI Non-infectious endocarditis
- 20. Nomenclature of neuro-psychiatric symptoms of SLE (ACR ad hoc Committee, Arthritis Rheum. 42:599-608, 1999.) CNS Aseptic
- 21. Histopathologic classification of lupus nephritis (ISN/RPS) Weening JJ et al. J Am Soc Nephrol 15: 241-50,
- 22. Mesangial LN Diffuse LN
- 23. Other manifestations Haematology Leukopenia, lymphopenia AIHA/ Thrombocytopenia/Evans sy. Pancytopenia TTP, CAPS Lymphadenopathy/Splenomegaly Othe Vasculitis Pancreatitis, lupus
- 24. Laboratory tests and findings in SLE General inflammatory findings: ESR , normal CRP Haematology: pancytopenia, Kidney
- 25. Radiology and other examinations in SLE Chest X ray, CT (HRCT), breath test, scan Abdominal ultrasonograph
- 26. Classification criteria for the diagnosis of lupus according to the American College of Rheumatology (ACR) 1.
- 27. Differential diagnosis of SLE 1. Other polysystemic autoimmune disorders polyarthritis myositis, muscle weakness Raynaud’s sy. Sjögren’s
- 28. Monitoring of activity in SLE disease activity index: DAI Convulsion 8 Psychosis 8 Organic brain syndrome
- 29. Subgroups in SLE Subacute cutan lupus erythematosus Neonatal lupus erythematosus Drug-induced lupus SLE in elderly SLE
- 30. SUBGROUPS IN SLE 1. SUBACUTE CUTAN LUPUS (SCLE) Clinical characteristics: annular/psoriasiform skin eruptions photosensitivity (60-70%) less
- 31. SLE SUBGROUPS 2. NEONATAL LUPUS (NLE) Frequency: rare Cause: maternal autoantibodies passing through the placenta Clinical
- 32. SUBGROUPS IN SLE 3. SLE IN ELDERLY Onset: over the age of 60 Frequency: around 10%
- 33. SLE SUBGOUPS 4. DRUG-INDUCED LUPUS (DIL) Clinical characteristics: more frequent in elderly reversible milder kidney and
- 34. Negative prognostic factors in SLE Sex:male Age under 20 or above 50 Diffuse proliferative lupus nephritis
- 35. Causes of death In the early phase of the disease process Kidney failer Neurology involvement SLE
- 36. Therapy of lupus - General procedures Avoidance of UV lights Sunscreens Termination of the use of
- 37. Therapy of SLE Antimalarial drugs: hydroxichlorouin, chloroquin (Delagil) In the cases of arthralgia, arthritis, skin symptoms,
- 38. Therapy of SLE Steroids: methylpednisolon (Solu-Medrol, Medrol, Methypred) In acute flares and relapses in neonatal lupus:
- 39. Immunosupressives Methotrexat (Trexan) 7.5-20 mg/week, treatment of polyarthritis, vasculitis CAVE: bonemarrow and liver toxicity Azathiorpin (Imuran)
- 40. Immunmodulation Cyclosporin A (Sandimmun Neoral) In the cases of haematology involvement, membranous lupus nephritis dosis: 3
- 41. Potential targets in the therapy of SLE
- 43. Скачать презентацию
General characteristics
Unknown etiology, multifactorial disease
Involve joints, kidneys, mucous membranes, the central
General characteristics
Unknown etiology, multifactorial disease
Involve joints, kidneys, mucous membranes, the central
Epidemiology
Prevalence: 50-100 /100.000
Incidence: 2-7 /100.000/year
age at onset: 20-30
Female vs. male ratio:
Epidemiology
Prevalence: 50-100 /100.000
Incidence: 2-7 /100.000/year
age at onset: 20-30
Female vs. male ratio:
Etiology
Family history (1st degree relatives 1%)
Genetic predisposition
MHC genes: HLA DR2,DR3
Etiology
Family history (1st degree relatives 1%)
Genetic predisposition
MHC genes: HLA DR2,DR3
Etiology
Provoking factors
Sunlight, UV light
Infections
Hormonal status:estrogen, prolactin
Drugs
Isoniacid
Hidantoin
Hydralazin
Procainamid
D penicillinamin
Penicillins
Sulphonamids
TNF alpha blockers
Etiology
Provoking factors
Sunlight, UV light
Infections
Hormonal status:estrogen, prolactin
Drugs
Isoniacid
Hidantoin
Hydralazin
Procainamid
D penicillinamin
Penicillins
Sulphonamids
TNF alpha blockers
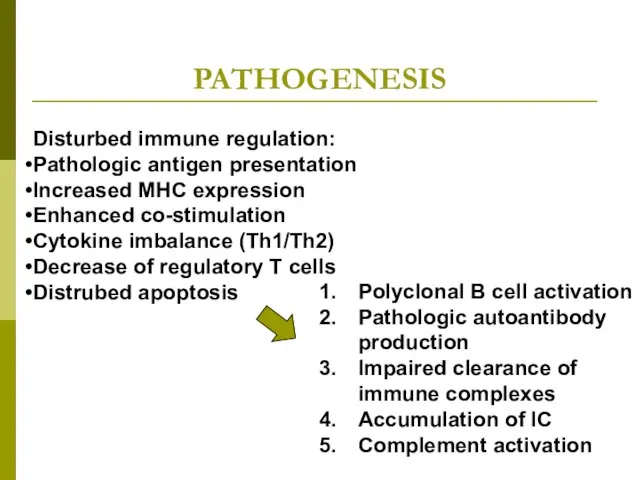
PATHOGENESIS
Disturbed immune regulation:
Pathologic antigen presentation
Increased MHC expression
Enhanced co-stimulation
Cytokine imbalance (Th1/Th2)
Decrease
PATHOGENESIS
Disturbed immune regulation:
Pathologic antigen presentation
Increased MHC expression
Enhanced co-stimulation
Cytokine imbalance (Th1/Th2)
Decrease
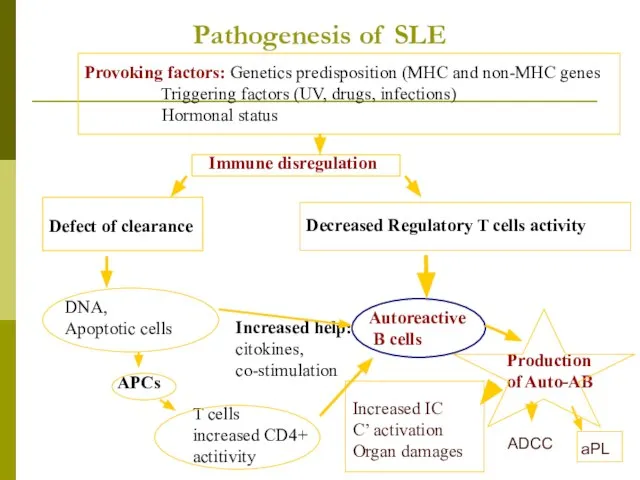
Pathogenesis of SLE
Provoking factors: Genetics predisposition (MHC and non-MHC genes
Triggering
Pathogenesis of SLE
Provoking factors: Genetics predisposition (MHC and non-MHC genes
Triggering
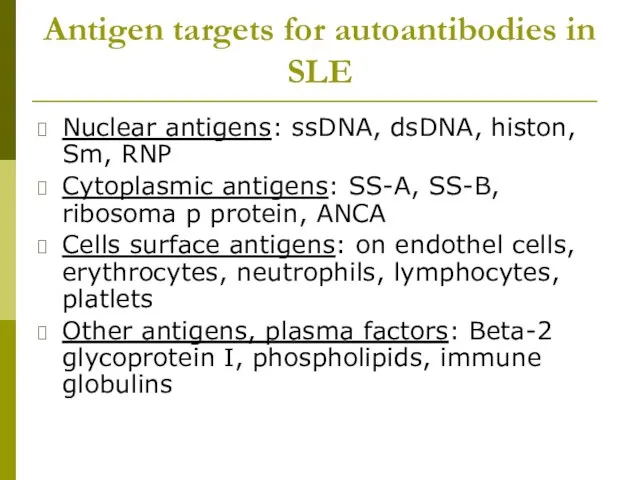
Antigen targets for autoantibodies in SLE
Nuclear antigens: ssDNA, dsDNA, histon, Sm,
Antigen targets for autoantibodies in SLE
Nuclear antigens: ssDNA, dsDNA, histon, Sm,
General symptoms
Weakness
Fatigue
Tiredness
Fever
Weight loss
Hair loss
Lymphadenopathy
General symptoms
Weakness
Fatigue
Tiredness
Fever
Weight loss
Hair loss
Lymphadenopathy
CLASSIFICATION OF SKIN SYMPTOMS IN SLE
(Sontheimer RD.Lupus 6:84-95, 1997)
Lupus specific
A.
CLASSIFICATION OF SKIN SYMPTOMS IN SLE
(Sontheimer RD.Lupus 6:84-95, 1997)
Lupus specific
A.
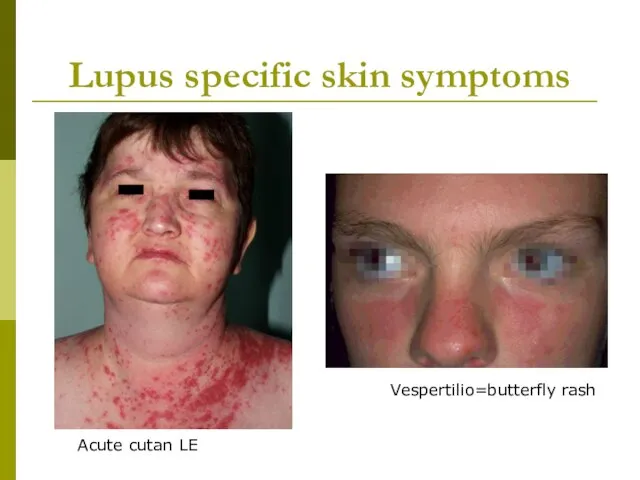
Lupus specific skin symptoms
Vespertilio=butterfly rash
Acute cutan LE
Lupus specific skin symptoms
Vespertilio=butterfly rash
Acute cutan LE

Lupus specific skin symptoms
DLE
SCLE
Lupus specific skin symptoms
DLE
SCLE

Non-lupus specific skin symptoms
vasculitis
Raynaud phenomenon
Non-lupus specific skin symptoms
vasculitis
Raynaud phenomenon
Musculosceletal involvment of lupus
Small joint symmetric non erosive polyarthritis
Aseptic femur neck
Musculosceletal involvment of lupus
Small joint symmetric non erosive polyarthritis
Aseptic femur neck
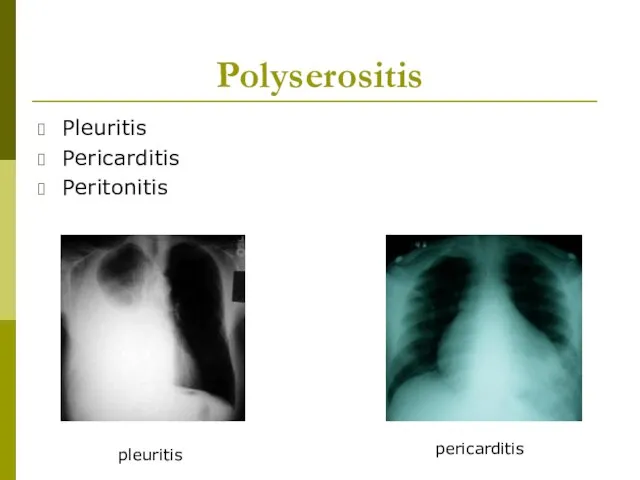
Polyserositis
Pleuritis
Pericarditis
Peritonitis
pleuritis
pericarditis
Polyserositis
Pleuritis
Pericarditis
Peritonitis
pleuritis
pericarditis
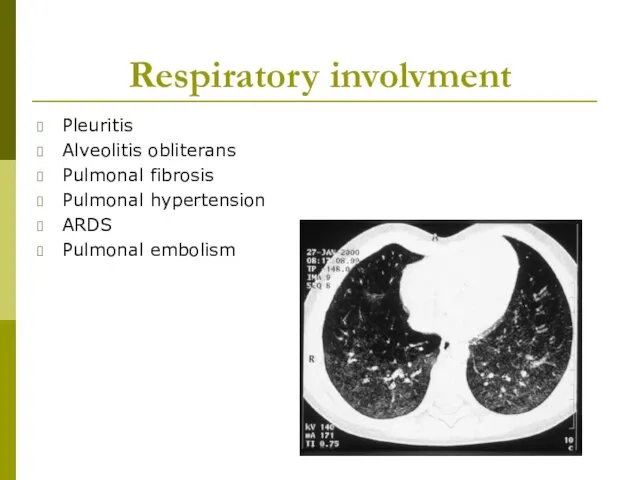
Respiratory involvment
Pleuritis
Alveolitis obliterans
Pulmonal fibrosis
Pulmonal hypertension
ARDS
Pulmonal embolism
Respiratory involvment
Pleuritis
Alveolitis obliterans
Pulmonal fibrosis
Pulmonal hypertension
ARDS
Pulmonal embolism
Cardiovascular involvments
Pericarditis
Myocarditis
Cardiomyopathy
Endocarditis
non-infectious verrucosus endocarditis
(Libman-Sacks endocarditis)
subacute infectious endocarditis
Valvulopathy
Atherosclerosis of coronary
Cardiovascular involvments
Pericarditis
Myocarditis
Cardiomyopathy
Endocarditis
non-infectious verrucosus endocarditis
(Libman-Sacks endocarditis)
subacute infectious endocarditis
Valvulopathy
Atherosclerosis of coronary
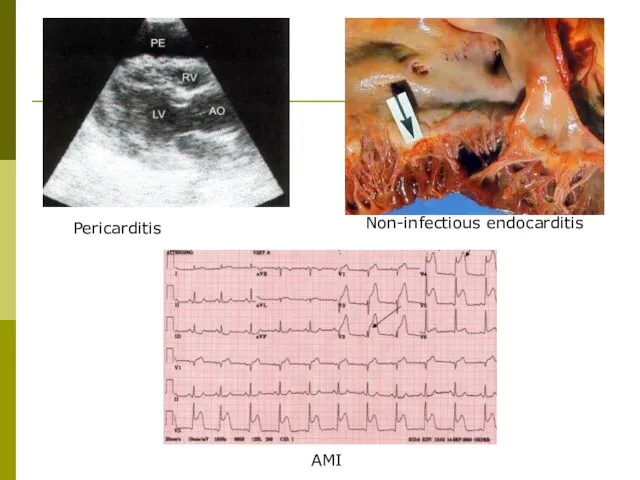
Pericarditis
AMI
Non-infectious endocarditis
Pericarditis
AMI
Non-infectious endocarditis
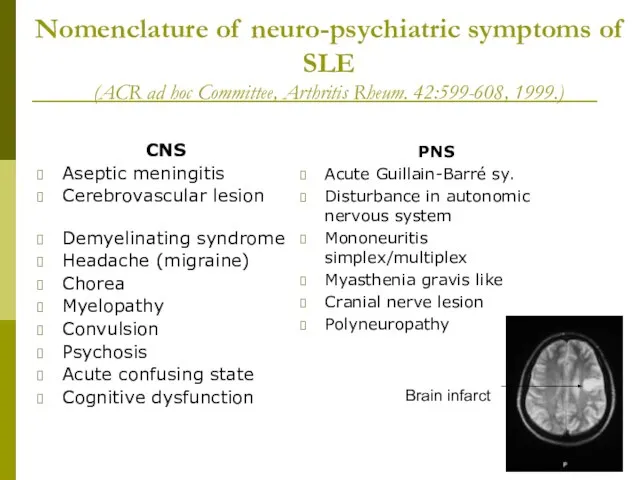
Nomenclature of neuro-psychiatric symptoms of SLE
(ACR ad hoc Committee, Arthritis
Nomenclature of neuro-psychiatric symptoms of SLE (ACR ad hoc Committee, Arthritis
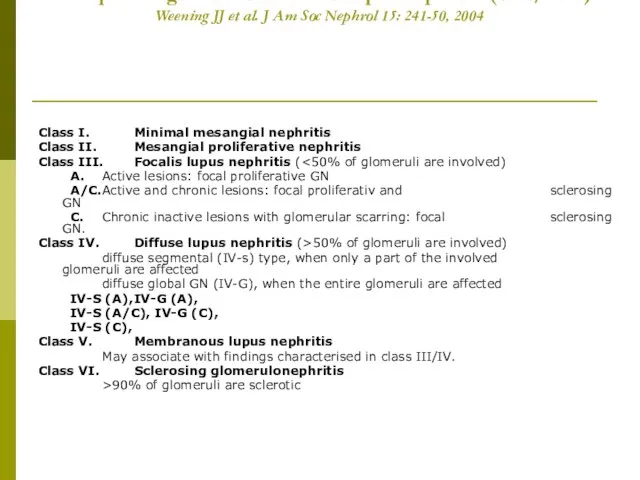
Histopathologic classification of lupus nephritis (ISN/RPS)
Weening JJ et al. J
Histopathologic classification of lupus nephritis (ISN/RPS) Weening JJ et al. J
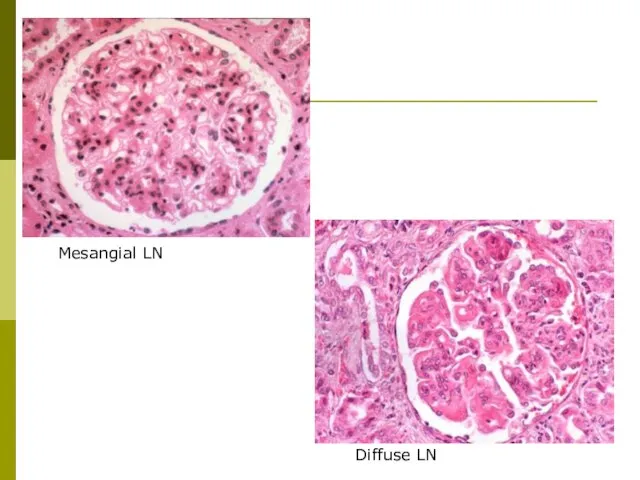
Mesangial LN
Diffuse LN
Mesangial LN
Diffuse LN
Other manifestations
Haematology
Leukopenia, lymphopenia
AIHA/ Thrombocytopenia/Evans sy.
Pancytopenia
TTP, CAPS
Lymphadenopathy/Splenomegaly
Othe
Vasculitis
Pancreatitis, lupus hepatitis
Pepeticus ulcus/GI-bleeding
Mesenterial thrombosis/vasculitis
A./v. central
Other manifestations
Haematology
Leukopenia, lymphopenia
AIHA/ Thrombocytopenia/Evans sy.
Pancytopenia
TTP, CAPS
Lymphadenopathy/Splenomegaly
Othe
Vasculitis
Pancreatitis, lupus hepatitis
Pepeticus ulcus/GI-bleeding
Mesenterial thrombosis/vasculitis
A./v. central
Laboratory tests and findings in SLE
General inflammatory findings: ESR , normal
Laboratory tests and findings in SLE
General inflammatory findings: ESR , normal
Radiology and other examinations in SLE
Chest X ray, CT (HRCT), breath
Radiology and other examinations in SLE
Chest X ray, CT (HRCT), breath
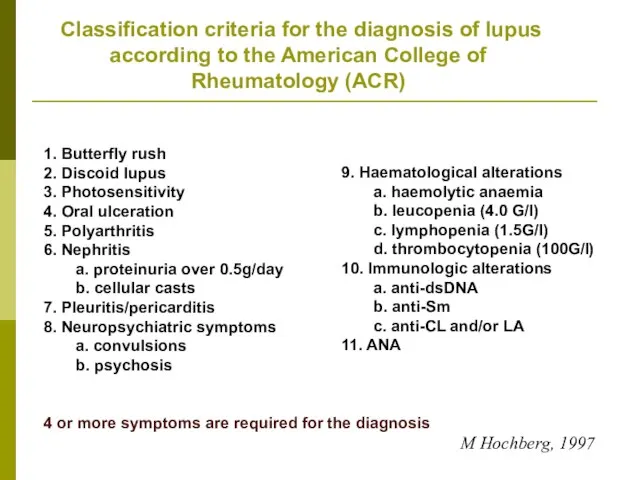
Classification criteria for the diagnosis of lupus according to
Classification criteria for the diagnosis of lupus according to
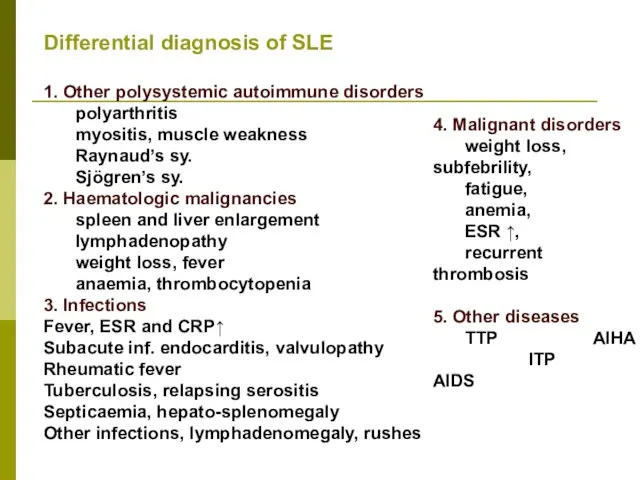
Differential diagnosis of SLE
1. Other polysystemic autoimmune disorders
polyarthritis
myositis, muscle weakness
Raynaud’s
Differential diagnosis of SLE
1. Other polysystemic autoimmune disorders
polyarthritis
myositis, muscle weakness
Raynaud’s
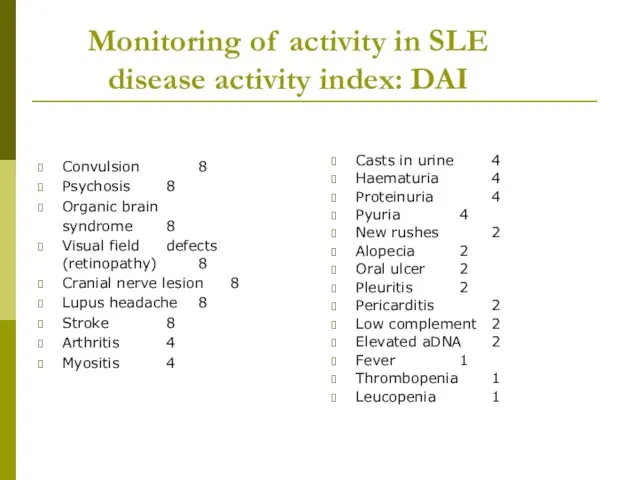
Monitoring of activity in SLE
disease activity index: DAI
Convulsion 8
Psychosis 8
Organic brain
syndrome 8
Visual field
Monitoring of activity in SLE
disease activity index: DAI
Convulsion 8
Psychosis 8
Organic brain
syndrome 8
Visual field
Subgroups in SLE
Subacute cutan lupus erythematosus
Neonatal lupus erythematosus
Drug-induced lupus
SLE in elderly
SLE
Subgroups in SLE
Subacute cutan lupus erythematosus
Neonatal lupus erythematosus
Drug-induced lupus
SLE in elderly
SLE
SUBGROUPS IN SLE
1. SUBACUTE CUTAN LUPUS (SCLE)
Clinical characteristics:
annular/psoriasiform skin eruptions
photosensitivity (60-70%)
less
SUBGROUPS IN SLE
1. SUBACUTE CUTAN LUPUS (SCLE)
Clinical characteristics:
annular/psoriasiform skin eruptions
photosensitivity (60-70%)
less
SLE SUBGROUPS
2. NEONATAL LUPUS (NLE)
Frequency: rare
Cause: maternal autoantibodies
passing through the placenta
Clinical
SLE SUBGROUPS
2. NEONATAL LUPUS (NLE)
Frequency: rare
Cause: maternal autoantibodies
passing through the placenta
Clinical
SUBGROUPS IN SLE
3. SLE IN ELDERLY
Onset: over the age of 60
Frequency: around 10%
Clinical
SUBGROUPS IN SLE
3. SLE IN ELDERLY
Onset: over the age of 60
Frequency: around 10%
Clinical
SLE SUBGOUPS
4. DRUG-INDUCED LUPUS (DIL)
Clinical characteristics: more frequent in elderly
reversible
milder
kidney and CNS
SLE SUBGOUPS
4. DRUG-INDUCED LUPUS (DIL)
Clinical characteristics: more frequent in elderly
reversible
milder
kidney and CNS
Negative prognostic factors in SLE
Sex:male
Age under 20 or above 50
Diffuse proliferative
Negative prognostic factors in SLE
Sex:male
Age under 20 or above 50
Diffuse proliferative
Causes of death
In the early phase of the disease process
Kidney failer
Neurology
Causes of death
In the early phase of the disease process
Kidney failer
Neurology
Therapy of lupus
-
General procedures
Avoidance of UV lights
Sunscreens
Termination of the use of
Therapy of lupus
-
General procedures
Avoidance of UV lights
Sunscreens
Termination of the use of
Therapy of SLE
Antimalarial drugs: hydroxichlorouin, chloroquin (Delagil)
In the cases of arthralgia,
Therapy of SLE
Antimalarial drugs: hydroxichlorouin, chloroquin (Delagil)
In the cases of arthralgia,
Therapy of SLE
Steroids: methylpednisolon (Solu-Medrol, Medrol, Methypred)
In acute flares and relapses
in neonatal
Therapy of SLE
Steroids: methylpednisolon (Solu-Medrol, Medrol, Methypred)
In acute flares and relapses
in neonatal
Immunosupressives
Methotrexat (Trexan)
7.5-20 mg/week, treatment of polyarthritis, vasculitis
CAVE: bonemarrow and liver
Immunosupressives
Methotrexat (Trexan)
7.5-20 mg/week, treatment of polyarthritis, vasculitis
CAVE: bonemarrow and liver
Immunmodulation
Cyclosporin A (Sandimmun Neoral)
In the cases of haematology involvement, membranous
Immunmodulation
Cyclosporin A (Sandimmun Neoral)
In the cases of haematology involvement, membranous
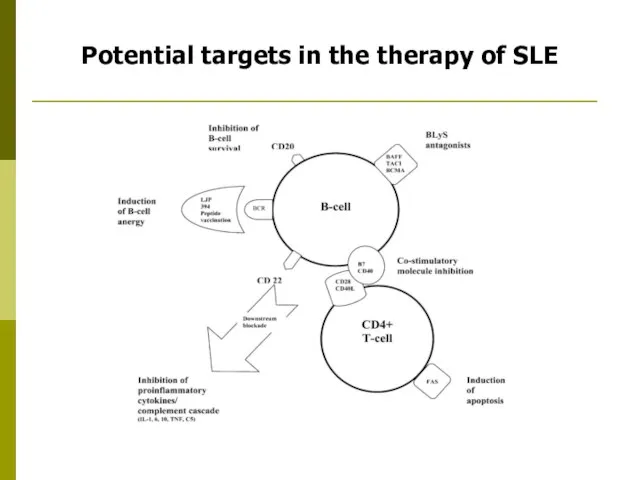
Potential targets in the therapy of SLE
Potential targets in the therapy of SLE
 С Днём учителя!
С Днём учителя! Golf GTI
Golf GTI Как я отдыхала летом в Одессе
Как я отдыхала летом в Одессе Mystic Places
Mystic Places Здания высоких технологий
Здания высоких технологий 20161029_pravovoy_turnir
20161029_pravovoy_turnir Электроснабжение объектов агропромышленного комплекса
Электроснабжение объектов агропромышленного комплекса Классный час Школьный этикет
Классный час Школьный этикет Супергидрофобты беттің мұздануға қарсы жүйеге әсері
Супергидрофобты беттің мұздануға қарсы жүйеге әсері Многоэтажные жилые дома
Многоэтажные жилые дома Измерительная система регистрации аварийных режимов полета самолета (вертолета) типа МСРП-12
Измерительная система регистрации аварийных режимов полета самолета (вертолета) типа МСРП-12 Теоретические основы технологического образования школьников
Теоретические основы технологического образования школьников Растровая и векторная анимация
Растровая и векторная анимация bezudarnye_okonchaniya_imen_prilagatelnyh
bezudarnye_okonchaniya_imen_prilagatelnyh космос группа №1
космос группа №1 Диафильм Серая Шейка
Диафильм Серая Шейка Информационное проектирование стратегических бизнес-процессов предприятия
Информационное проектирование стратегических бизнес-процессов предприятия Общежитие №7 Ул. Профессора Дедюкина, дом 22
Общежитие №7 Ул. Профессора Дедюкина, дом 22 Очень просто про самозанятость
Очень просто про самозанятость Виды оборудования для упаковки хлебобулочных изделий
Виды оборудования для упаковки хлебобулочных изделий Приближённые решения алгебраических и трансцендентных уравнений
Приближённые решения алгебраических и трансцендентных уравнений Свойства транспортируемых грузов
Свойства транспортируемых грузов 20150224_prezentatsiya_dekabristy_na_kubani
20150224_prezentatsiya_dekabristy_na_kubani Зашумлённый текст
Зашумлённый текст Stadii_i_zakony_razvitia_kollektiva_narodnogo_khudozhestvennogo
Stadii_i_zakony_razvitia_kollektiva_narodnogo_khudozhestvennogo 20160316_issled.rab_tradeskantsiya
20160316_issled.rab_tradeskantsiya The shades and ceiling lamps are made from natural materials
The shades and ceiling lamps are made from natural materials Ноутбук у нашому житті
Ноутбук у нашому житті