- Atherosclerosis. Hypertensive disease. Ischemic heart disease

Содержание
- 2. Atherosclerosis (athere – latin gruel) is a chronic disease which is characterized by formation of vascular
- 3. 1. Age (reducing of sex hormones synthesis and tissue regeneration, i.e. reducing of cholesterol consumption by
- 4. 1. Development of focal regions of chronic endothelial injury leading to increased vascular permeability and increased
- 5. 5. Adhesion of platelets to the focal areas of endothelial injury. 6. Release of biologically active
- 6. 8. Enhanced accumulation of lipids both within cells (macrophages and smooth muscle cells) and extracellularly. 9.
- 7. Aorta is usually the most involved vessel, the aortic lesions tend to be much more prominent
- 8. 1. Pre-lipid stage has no gross appearance; microscopically the changes in intima are equal to mucoid
- 9. 2. In lipidosis stage the accumulation of lipids in the intima leads to formation of fatty
- 10. Atherosclerosis of aorta, lipidosis stage. Fatty streaks
- 11. Lipoidosis stage
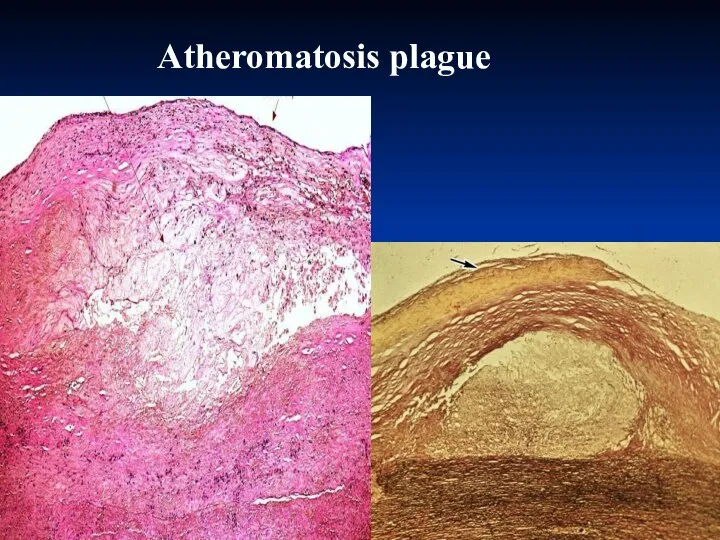
- 12. 3. In atheromatosis stage the characteristic plaques are formed. They appear as raised focal areas within
- 13. Atheromatosis stage
- 14. Atherosclerosis of aorta, three different degrees of damage
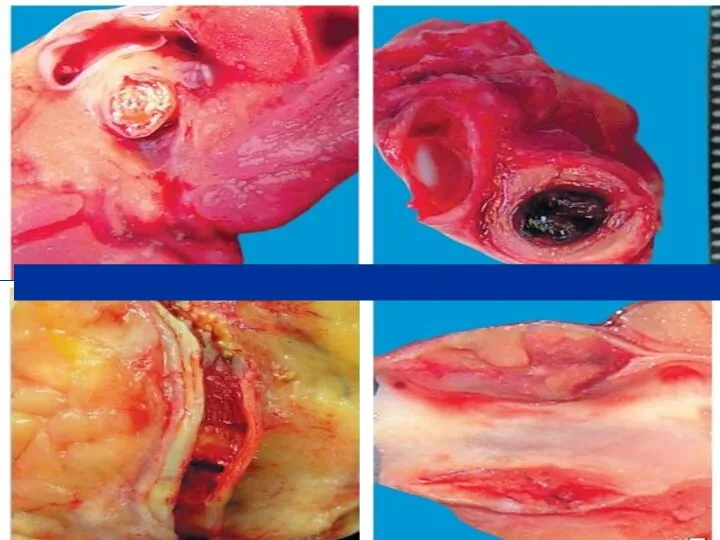
- 15. Atherosclerosis of coronary artery
- 16. АТЕРОСКЛЕРОЗ ВІНЦЕВИХ АРТЕРІЙ СЕРЦЯ
- 17. Atherosclerosis of basilar artery
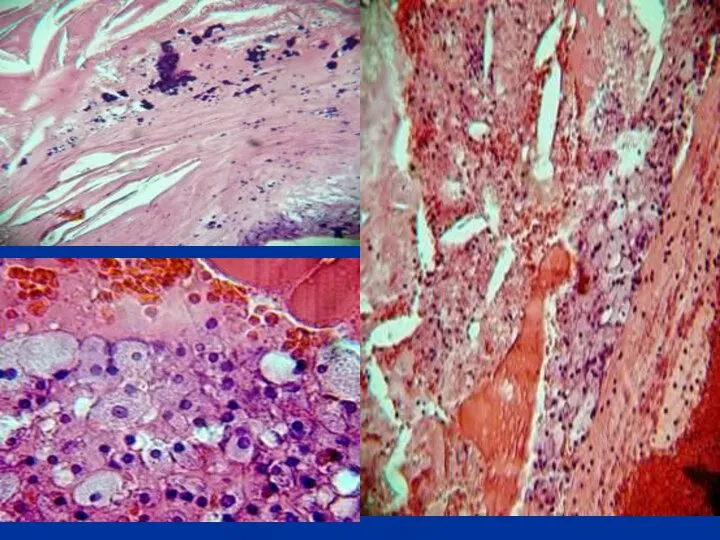
- 18. Atheromatosis plague
- 19. Atherosclerosis of coronary artery, 40 magnification, H&E stain
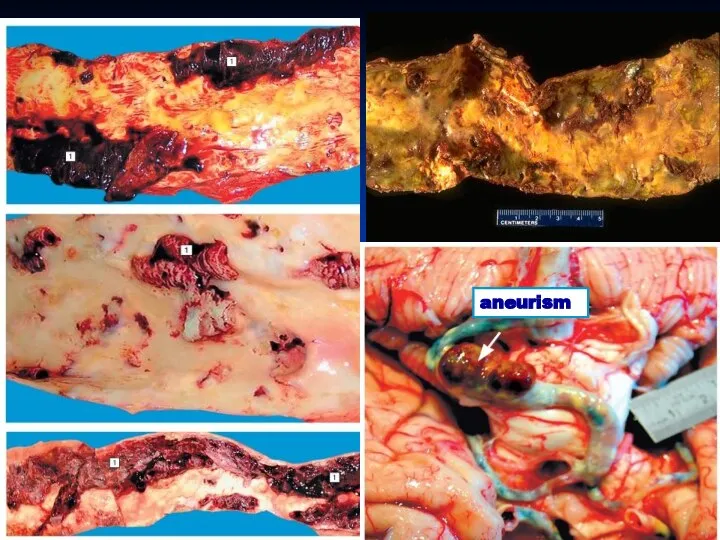
- 20. 4. Stage of complications. Atherosclerotic complications may be acute and chronic. It is believed that prominent
- 21. aneurism
- 23. 1. Focal rupture or gross ulceration, or both, of the luminal surface of atheromatous plaques may
- 24. 3. Superimposed thrombosis usually occurs on disrupted lesions (those with rupture, ulceration, erosion, or hemorrhage). Thrombi
- 25. Dry gangrene of foot Necrosis in heart wall
- 26. Gangrene of intestine
- 27. Atherosclerotic nephrosclеrosis
- 28. Infarction of heart
- 29. Infarction of brain
- 30. 1. Atheromas in advanced disease undergo patchy or massive calcification. Arteries may become virtual pipe stems,
- 32. 3. Uncomplicated atherosclerotic lesions usually cause narrowing of vessel lumen leading to decreasing of blood circulation
- 33. Dystrophic calcification of aortic valve leaflets
- 34. Hypertensive disease is a chronic disease which is characterized by chronic elevation of blood pressure that
- 35. Primary (idiopathic, essential) hypertension (90-95%): benign; malignant (or accelerated). Secondary hypertension that may be caused by:
- 36. 1. Age. 2. Environmental factors (e.g. frequent stresses, increased salt intake, increased estrogen level). 3. Genetic
- 37. In hypertensive disease both increased cardiac output and increased peripheral resistance due to constriction of vessel
- 38. In this stage there are periodical elevations of blood pressure. Morphologically this stage is characterized by
- 39. In benign hypertensive diseases the prolonged periods of arterioles constriction lead to narrowing of vessels, decreased
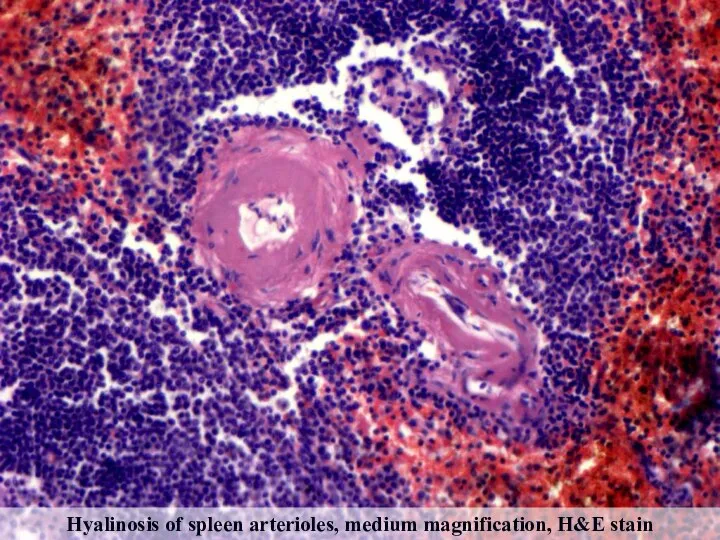
- 40. Hyalinosis of spleen arterioles, medium magnification, H&E stain
- 41. The muscular-elastic arteries firstly show adaptive changes – thickening and reduplication of the intimal elastic lamina
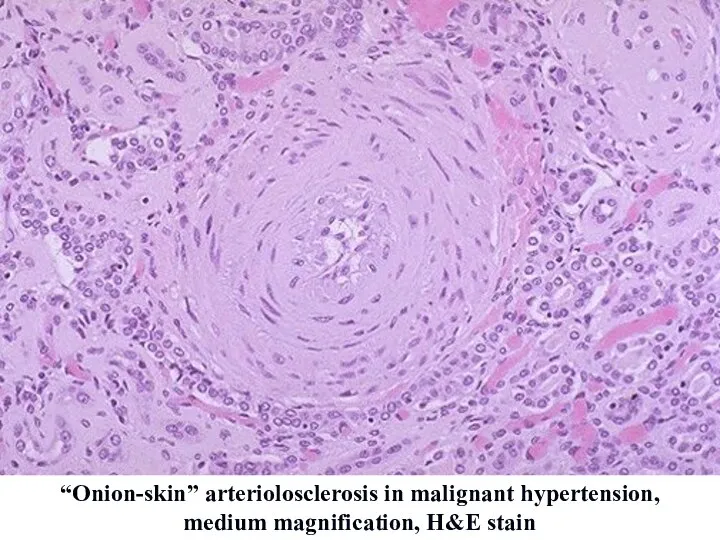
- 42. In malignant hypertension rapid and sharp elevation of blood pressure is caused by extremely severe vasoconstriction
- 43. “Onion-skin” arteriolosclerosis in malignant hypertension, medium magnification, H&E stain
- 44. Fibrinoid necrosis of renal artery in malignant hypertension, medium magnification, H&E stain
- 45. “Onion-skin” arteriole, PAS-stain Fibrinoid necrosis of arteriole, PAS-stain
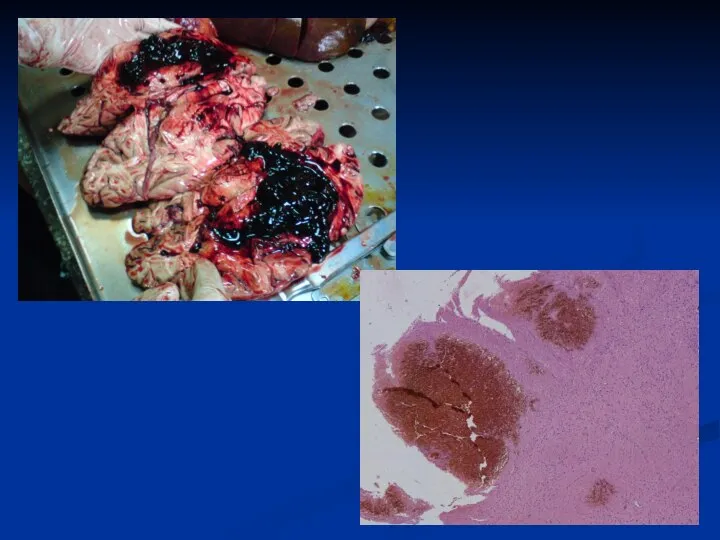
- 46. Acute complications: - infarction (myocardial, brain); - hemorrhages due to rupture of vessels affected with atherosclerosis).
- 48. Gross appearance: kidneys are smaller than normal and affected bilaterally. The cortical surface exhibits a fine
- 49. Benign nephrosclerosis
- 50. Gross appearance: size of the kidneys varies from small to enlarged, depending on the duration of
- 51. “Flea-bitten” kidney in malignant hypertension
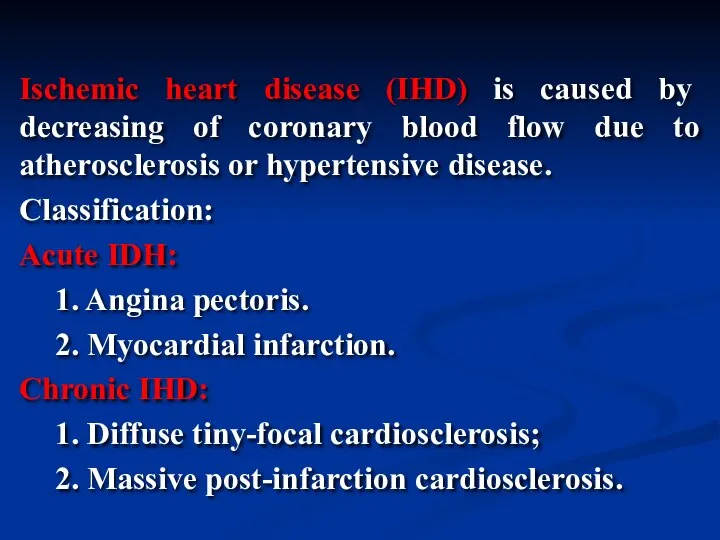
- 52. Ischemic heart disease (IHD) is caused by decreasing of coronary blood flow due to atherosclerosis or
- 53. Transmural infarction
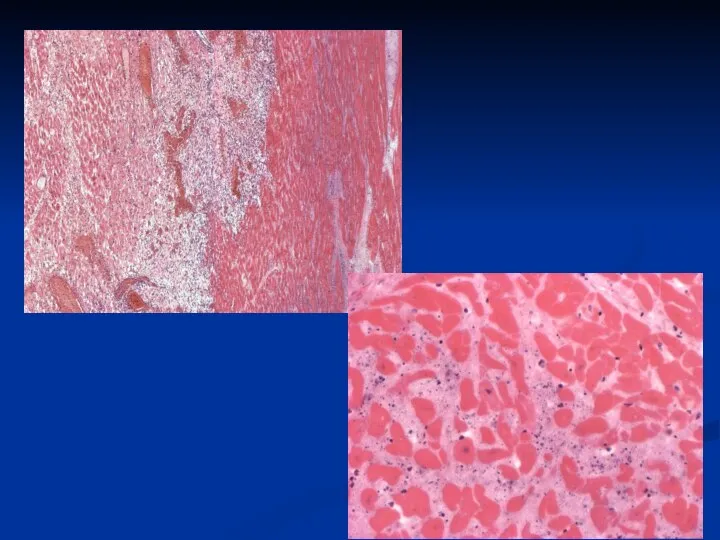
- 54. 18-24 hours ago
- 55. 3 – 4 days ago 1- 2 weeks ago Hemopericardium
- 59. Ischemic brain disease –cerebra-vascular disease
- 61. Скачать презентацию
Atherosclerosis (athere – latin gruel) is a chronic disease which is
Atherosclerosis (athere – latin gruel) is a chronic disease which is
1. Age (reducing of sex hormones synthesis and tissue regeneration, i.e.
1. Age (reducing of sex hormones synthesis and tissue regeneration, i.e.
1. Development of focal regions of chronic endothelial injury leading to
1. Development of focal regions of chronic endothelial injury leading to
5. Adhesion of platelets to the focal areas of endothelial injury.
6.
5. Adhesion of platelets to the focal areas of endothelial injury.
6.
8. Enhanced accumulation of lipids both within cells (macrophages and smooth
8. Enhanced accumulation of lipids both within cells (macrophages and smooth
Aorta is usually the most involved vessel, the aortic lesions tend
Aorta is usually the most involved vessel, the aortic lesions tend
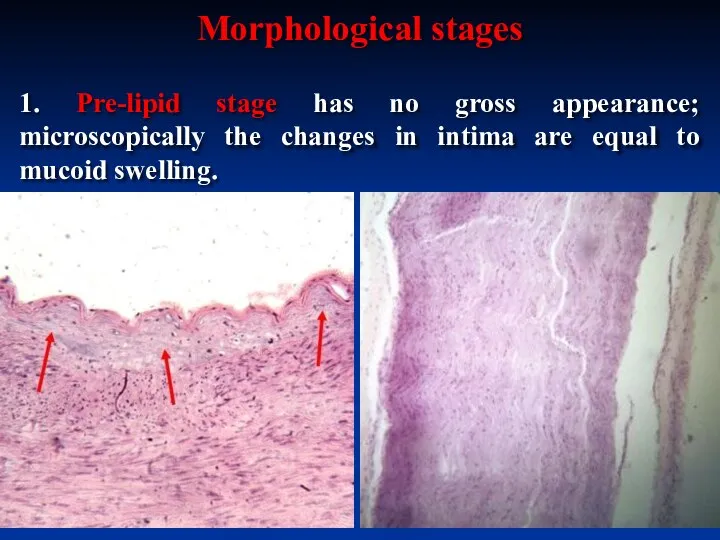
1. Pre-lipid stage has no gross appearance; microscopically the changes in
1. Pre-lipid stage has no gross appearance; microscopically the changes in
2. In lipidosis stage the accumulation of lipids in the intima
2. In lipidosis stage the accumulation of lipids in the intima

Atherosclerosis of aorta, lipidosis stage. Fatty streaks
Atherosclerosis of aorta, lipidosis stage. Fatty streaks
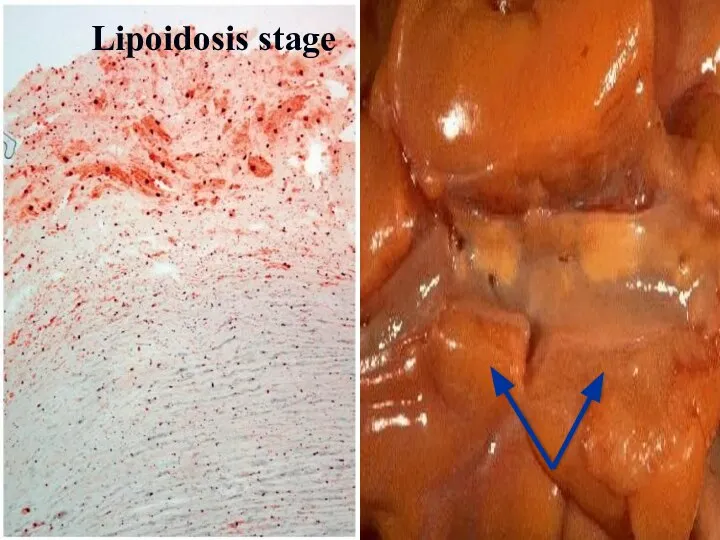
Lipoidosis stage
Lipoidosis stage
3. In atheromatosis stage the characteristic plaques are formed. They
3. In atheromatosis stage the characteristic plaques are formed. They
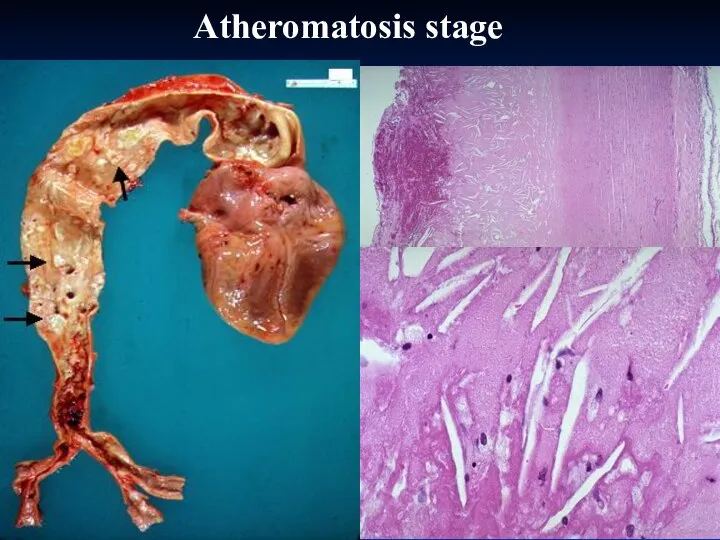
Atheromatosis stage
Atheromatosis stage
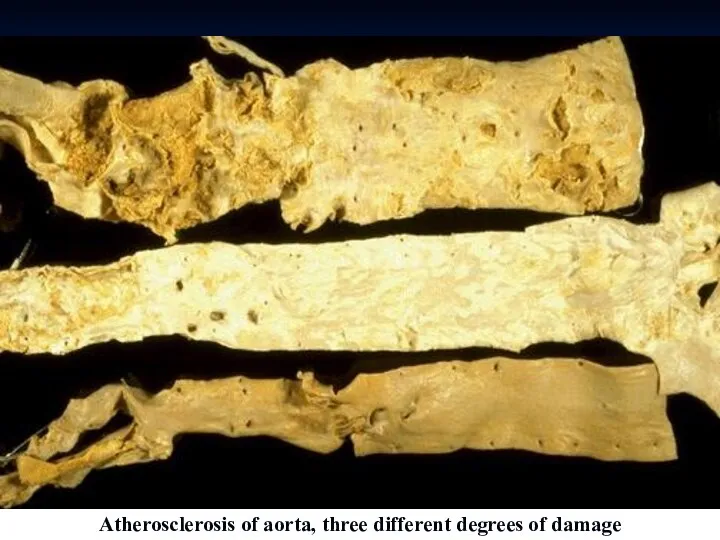
Atherosclerosis of aorta, three different degrees of damage
Atherosclerosis of aorta, three different degrees of damage

Atherosclerosis of coronary artery
Atherosclerosis of coronary artery
АТЕРОСКЛЕРОЗ ВІНЦЕВИХ АРТЕРІЙ СЕРЦЯ
АТЕРОСКЛЕРОЗ ВІНЦЕВИХ АРТЕРІЙ СЕРЦЯ
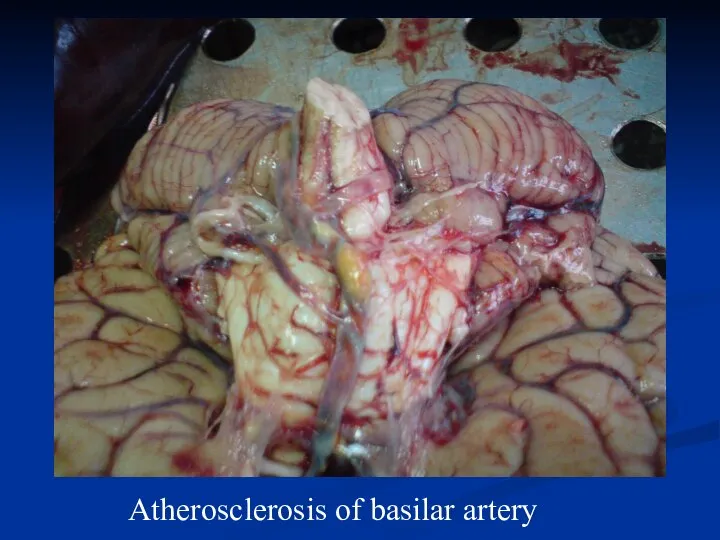
Atherosclerosis of basilar artery
Atherosclerosis of basilar artery
Atheromatosis plague
Atheromatosis plague

Atherosclerosis of coronary artery, 40 magnification, H&E stain
Atherosclerosis of coronary artery, 40 magnification, H&E stain
4. Stage of complications.
Atherosclerotic complications may be acute and chronic.
4. Stage of complications.
Atherosclerotic complications may be acute and chronic.
aneurism
aneurism
1. Focal rupture or gross ulceration, or both, of the luminal
1. Focal rupture or gross ulceration, or both, of the luminal
3. Superimposed thrombosis usually occurs on disrupted lesions (those with rupture,
3. Superimposed thrombosis usually occurs on disrupted lesions (those with rupture,

Dry gangrene of foot
Necrosis in heart wall
Dry gangrene of foot
Necrosis in heart wall

Gangrene of intestine
Gangrene of intestine
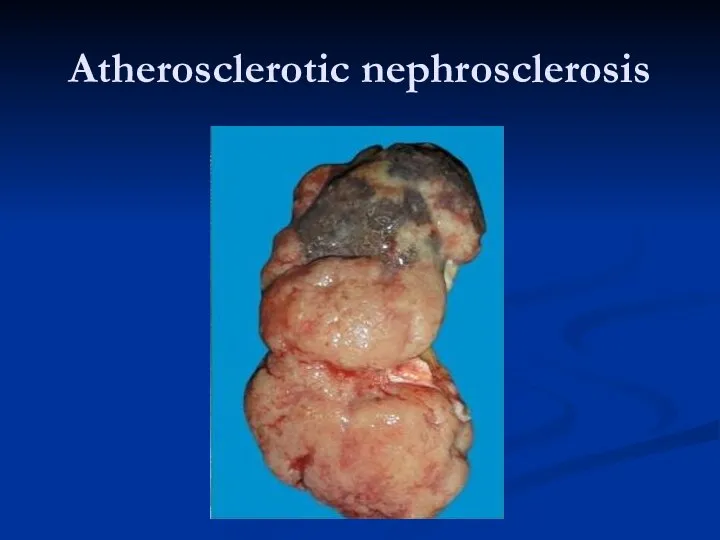
Atherosclerotic nephrosclеrosis
Atherosclerotic nephrosclеrosis
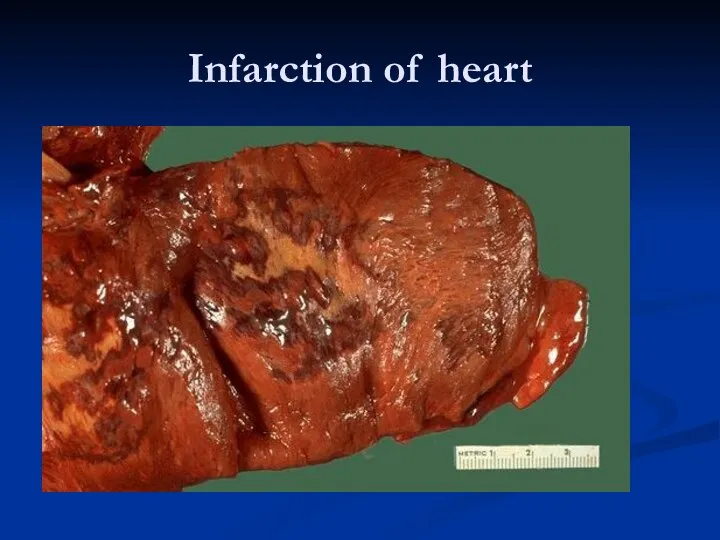
Infarction of heart
Infarction of heart
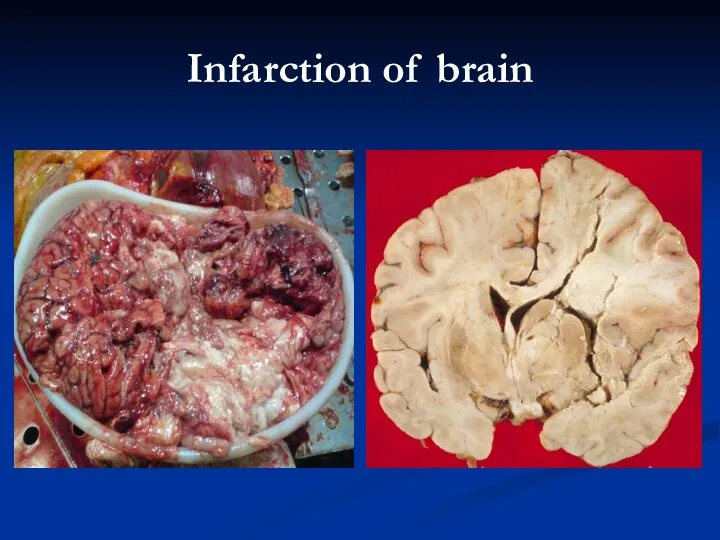
Infarction of brain
Infarction of brain
1. Atheromas in advanced disease undergo patchy or massive calcification. Arteries
1. Atheromas in advanced disease undergo patchy or massive calcification. Arteries

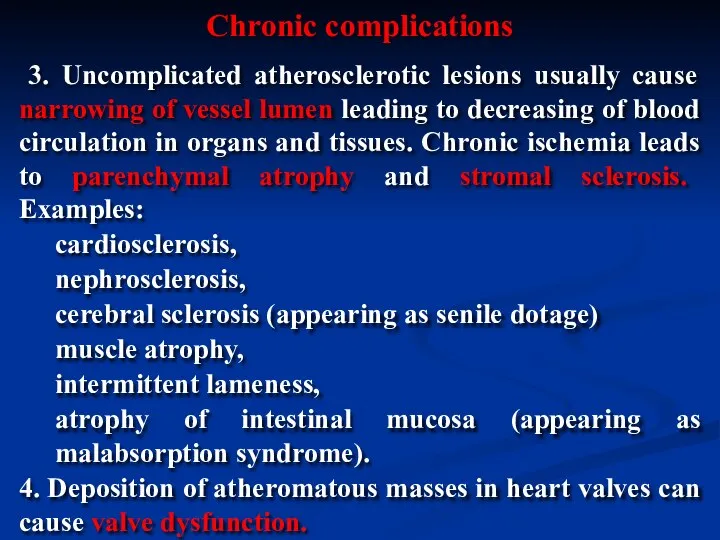
3. Uncomplicated atherosclerotic lesions usually cause narrowing of vessel lumen
3. Uncomplicated atherosclerotic lesions usually cause narrowing of vessel lumen
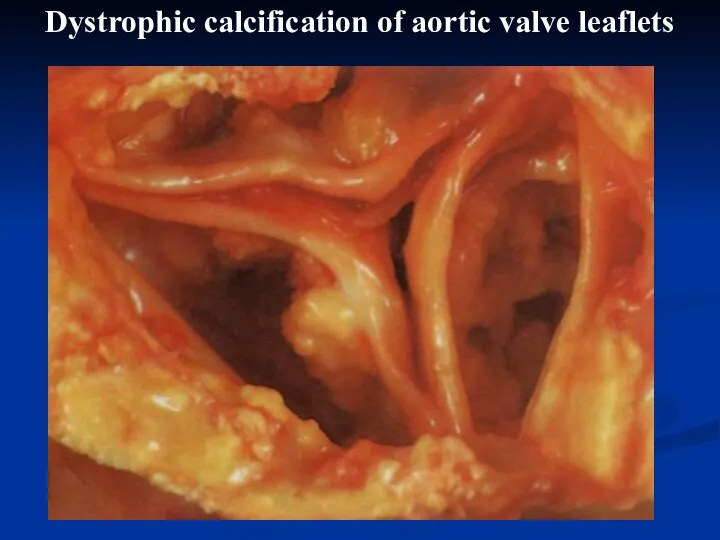
Dystrophic calcification of aortic valve leaflets
Dystrophic calcification of aortic valve leaflets
Hypertensive disease is a chronic disease which is characterized by chronic
Hypertensive disease is a chronic disease which is characterized by chronic
Primary (idiopathic, essential) hypertension (90-95%):
benign;
malignant (or accelerated).
Secondary hypertension that may be
Primary (idiopathic, essential) hypertension (90-95%):
benign;
malignant (or accelerated).
Secondary hypertension that may be
1. Age.
2. Environmental factors (e.g. frequent stresses, increased salt intake, increased
1. Age.
2. Environmental factors (e.g. frequent stresses, increased salt intake, increased
In hypertensive disease both increased cardiac output and increased peripheral resistance
In hypertensive disease both increased cardiac output and increased peripheral resistance
In this stage there are periodical elevations of blood pressure. Morphologically
In this stage there are periodical elevations of blood pressure. Morphologically
In benign hypertensive diseases the prolonged periods of arterioles constriction lead
In benign hypertensive diseases the prolonged periods of arterioles constriction lead
Hyalinosis of spleen arterioles, medium magnification, H&E stain
Hyalinosis of spleen arterioles, medium magnification, H&E stain
The muscular-elastic arteries firstly show adaptive changes – thickening and reduplication
The muscular-elastic arteries firstly show adaptive changes – thickening and reduplication
In malignant hypertension rapid and sharp elevation of blood pressure is
In malignant hypertension rapid and sharp elevation of blood pressure is
“Onion-skin” arteriolosclerosis in malignant hypertension,
medium magnification, H&E stain
“Onion-skin” arteriolosclerosis in malignant hypertension,
medium magnification, H&E stain
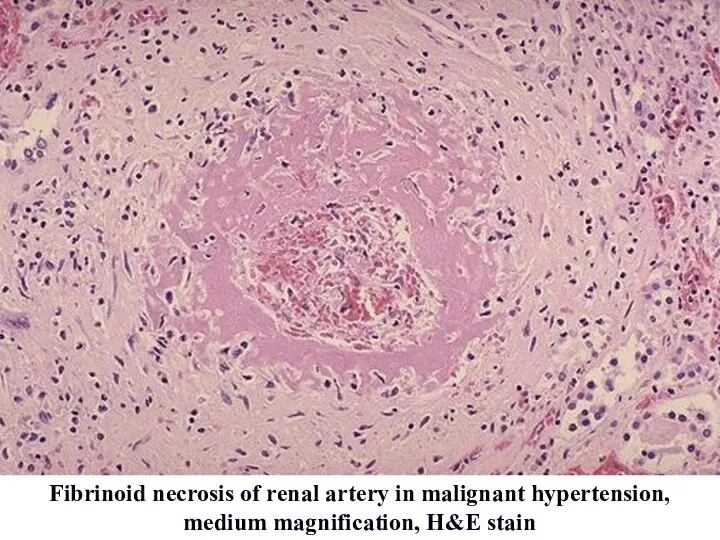
Fibrinoid necrosis of renal artery in malignant hypertension, medium magnification, H&E
Fibrinoid necrosis of renal artery in malignant hypertension, medium magnification, H&E
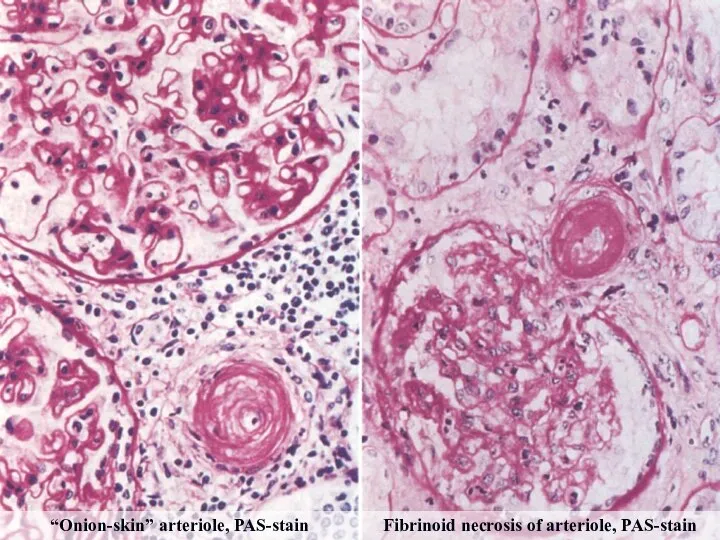
“Onion-skin” arteriole, PAS-stain
Fibrinoid necrosis of arteriole, PAS-stain
“Onion-skin” arteriole, PAS-stain
Fibrinoid necrosis of arteriole, PAS-stain
Acute complications:
- infarction (myocardial, brain);
- hemorrhages due to rupture of vessels
Acute complications:
- infarction (myocardial, brain);
- hemorrhages due to rupture of vessels
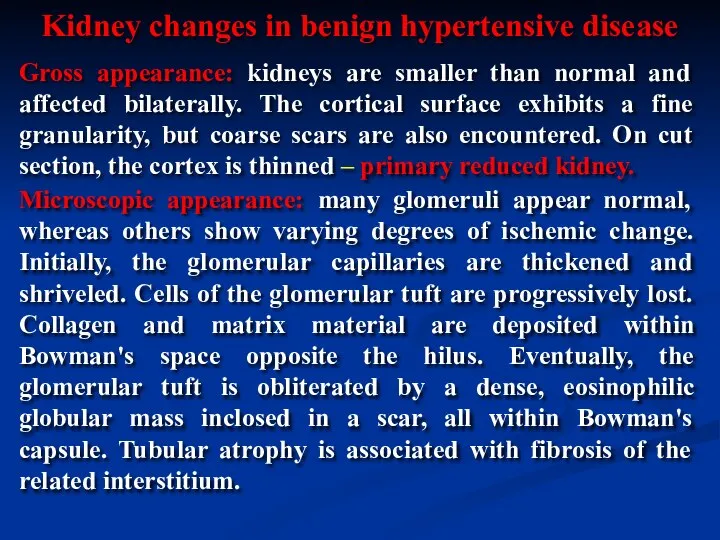
Gross appearance: kidneys are smaller than normal and affected bilaterally. The
Gross appearance: kidneys are smaller than normal and affected bilaterally. The
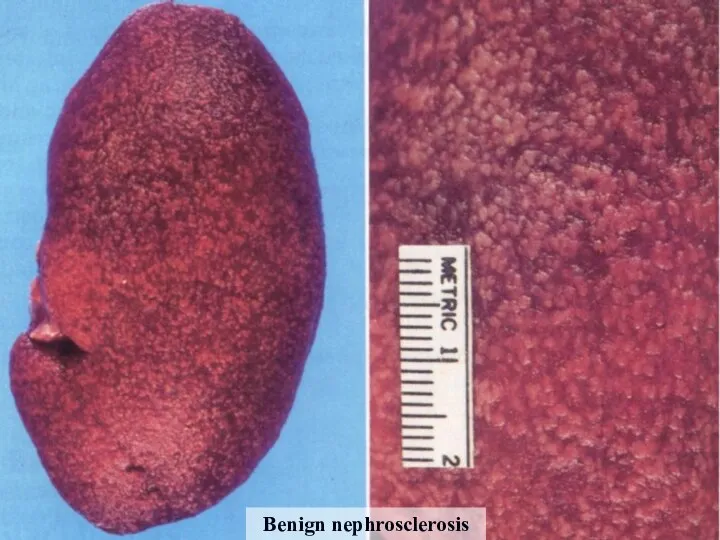
Benign nephrosclerosis
Benign nephrosclerosis
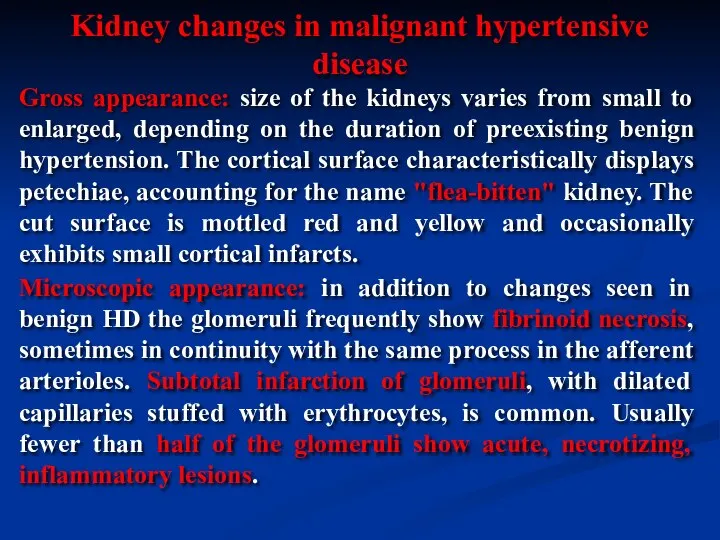
Gross appearance: size of the kidneys varies from small to enlarged,
Gross appearance: size of the kidneys varies from small to enlarged,
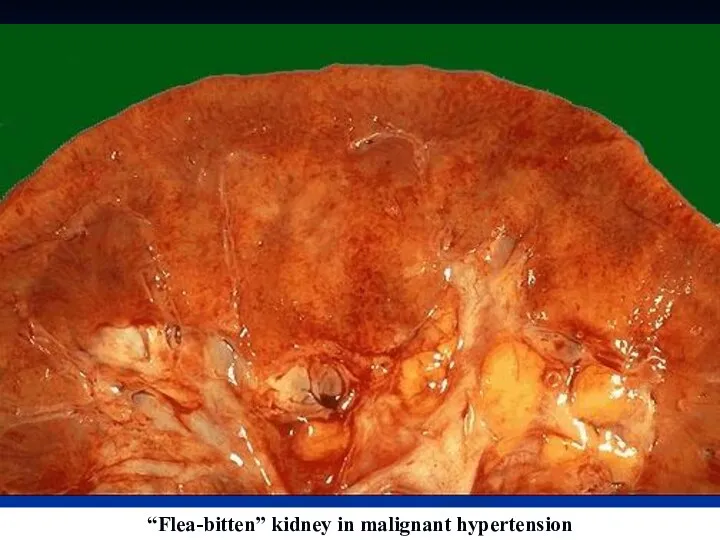
“Flea-bitten” kidney in malignant hypertension
“Flea-bitten” kidney in malignant hypertension
Ischemic heart disease (IHD) is caused by decreasing of coronary blood
Ischemic heart disease (IHD) is caused by decreasing of coronary blood
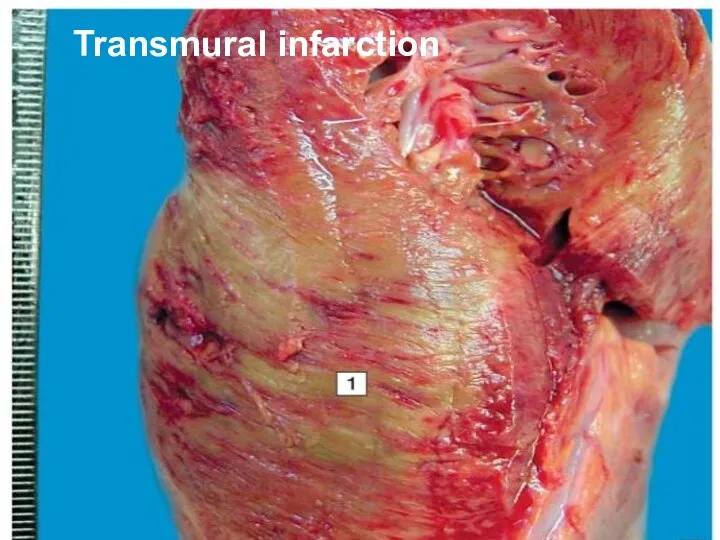
Transmural infarction
Transmural infarction

18-24 hours ago
18-24 hours ago
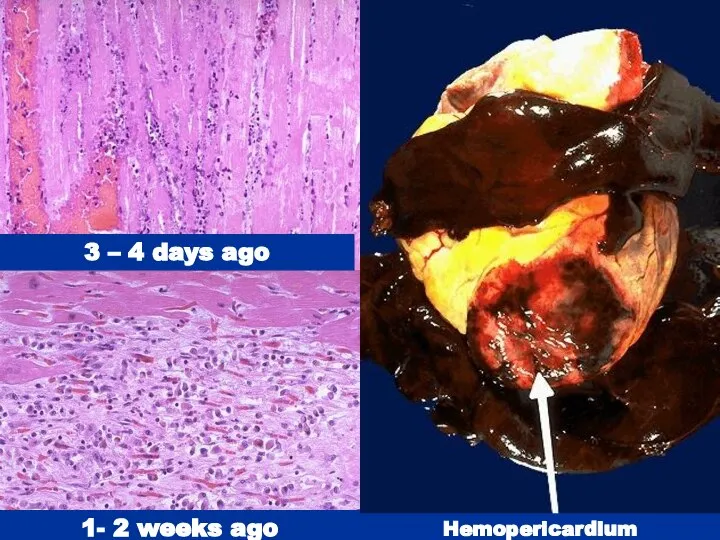
3 – 4 days ago
1- 2 weeks ago
Hemopericardium
3 – 4 days ago
1- 2 weeks ago
Hemopericardium


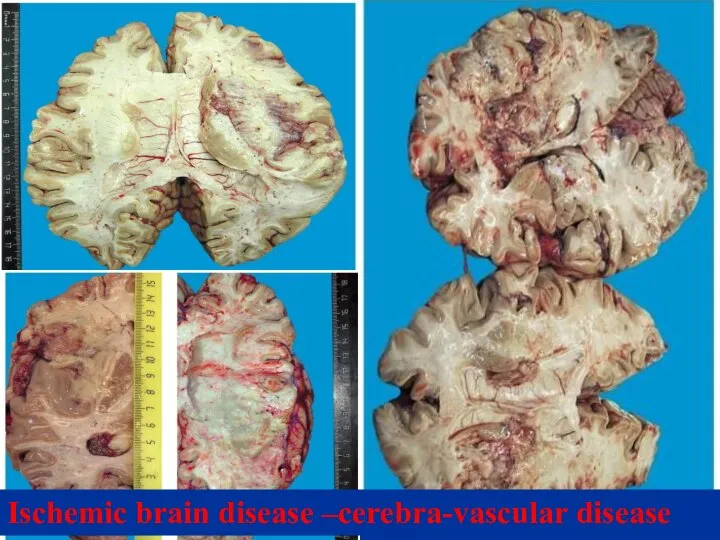
Ischemic brain disease –cerebra-vascular disease
Ischemic brain disease –cerebra-vascular disease
 "Акме" в професійному розвитку людини
"Акме" в професійному розвитку людини Нарушение гемостаза
Нарушение гемостаза Ингаляционная анестезия
Ингаляционная анестезия Рак толстого кишечника
Рак толстого кишечника Качества жизни в современной медицине
Качества жизни в современной медицине Каноны этических требований к моральному облику врача
Каноны этических требований к моральному облику врача Ишемический инсульт
Ишемический инсульт Эпикриз. Часть 2
Эпикриз. Часть 2 Основы рационального питания. Принципы формирования диет. Кормление пациента
Основы рационального питания. Принципы формирования диет. Кормление пациента Наркозные средства. Спирт этиловый
Наркозные средства. Спирт этиловый Человеческие зависимости
Человеческие зависимости Ғылым және ғылыми зерттеулер. Ғылым және олардың жіктеулері. Ғылыми зерттеулер және олардың мәні
Ғылым және ғылыми зерттеулер. Ғылым және олардың жіктеулері. Ғылыми зерттеулер және олардың мәні Адаптация. Степени тяжести адаптации
Адаптация. Степени тяжести адаптации Основные характеристики ВИЧ - инфекции
Основные характеристики ВИЧ - инфекции Функциональные заболевания желудочно-кишечного тракта у детей
Функциональные заболевания желудочно-кишечного тракта у детей СП при колитах
СП при колитах Роль рентгеновского излучения в медицине
Роль рентгеновского излучения в медицине Возрастные особенности строения и топографии лор-органов у взрослых
Возрастные особенности строения и топографии лор-органов у взрослых Герпетический энцефалит
Герпетический энцефалит Правильное питание и последствия его нарушения
Правильное питание и последствия его нарушения Антисекреторные препараты (ингибиторы протонной помпы, блокаторы гистаминовых Н2-рецепторов)
Антисекреторные препараты (ингибиторы протонной помпы, блокаторы гистаминовых Н2-рецепторов) Пороки сердца (продолжение). Лекция 2
Пороки сердца (продолжение). Лекция 2 История сердечно-сосудистой хирургии и интервенционной кардиоангиологии
История сердечно-сосудистой хирургии и интервенционной кардиоангиологии Современная инсулинотерапия
Современная инсулинотерапия Общие сведения о ядах и отравлениях (основы судебной токсикологии)
Общие сведения о ядах и отравлениях (основы судебной токсикологии) Здоровьесберегающие технологии в условиях загородного лагеря
Здоровьесберегающие технологии в условиях загородного лагеря Виды психокоррекционных групп
Виды психокоррекционных групп Клиническая история болезни
Клиническая история болезни