- Bronchiectasis

Содержание
- 3. Bronchiectasis - involve the lung in a focal or a diffuse manner . (1) Cylindrical or
- 4. Bronchiectasis with predominant involvement of the : Upper lung fields: Cystic fibrosis (CF) Postradiation fibrosis corresponding
- 5. The incidence of bronchiectasis increases with age. Bronchiectasis is more common among women than among men.
- 6. The most common clinical presentation is a persistent productive cough with ongoing production of thick, tenacious
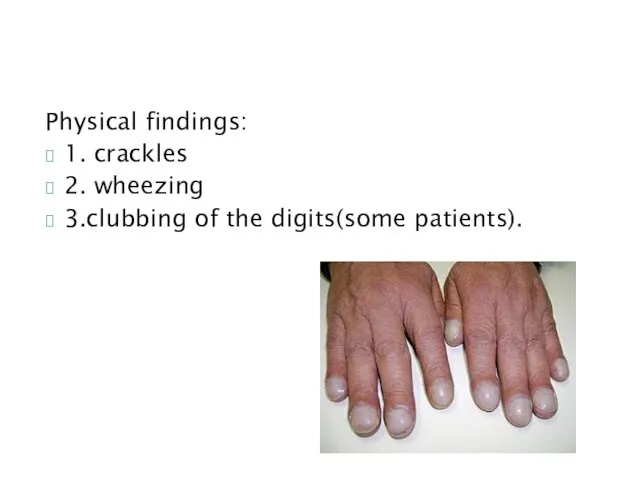
- 7. Physical findings: 1. crackles 2. wheezing 3.clubbing of the digits(some patients).
- 8. Pulmonary function tests: mild to moderate airflow obstruction, overlapping with that seen at presentation with other
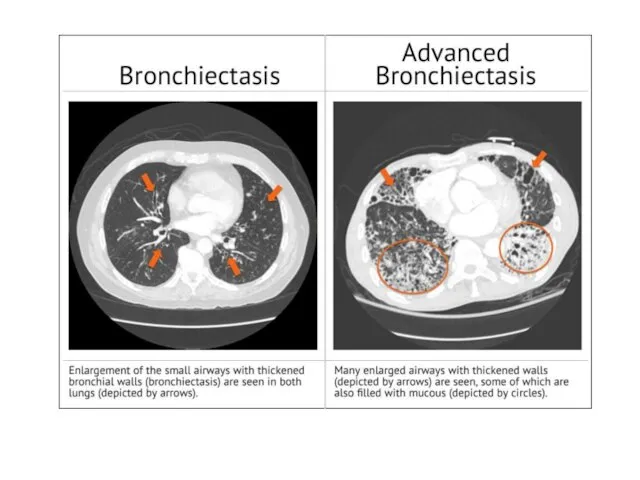
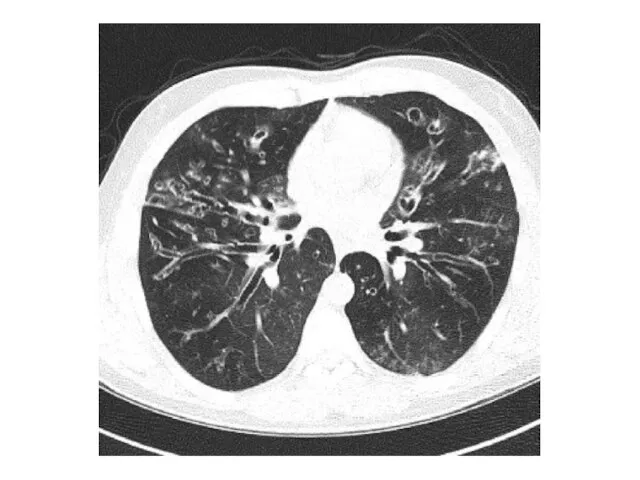
- 9. Airway dilation (detected as parallel "tram tracks" or as the "signet-ring sign" -a cross-sectional area of
- 12. 1. Control of active infection 2. Minimlize the risk of repeated infections by improvements in secretion
- 13. Numerous approaches used to enhance secretion clearance include: hydration mucolytic administration, aerosolization of bronchodilators and hyperosmolar
- 14. In select cases, surgery can be considered, with resection of a focal area of suppuration. In
- 15. Outcomes of bronchiectasis can vary widely with: the underlying etiology the frequency of exacerbations the specific
- 16. Trying to decrease the risk of recurrent infections by: Reversal of an underlying immunodeficient state (e.g.
- 17. Administration of an oral antibiotic (e.g. ciprofloxacin) daily for 1-2 weeks per month. Use of a
- 29. ARDS
- 30. ARDS is an acute, diffuse, inflammatory form of lung injury that is associated with a variety
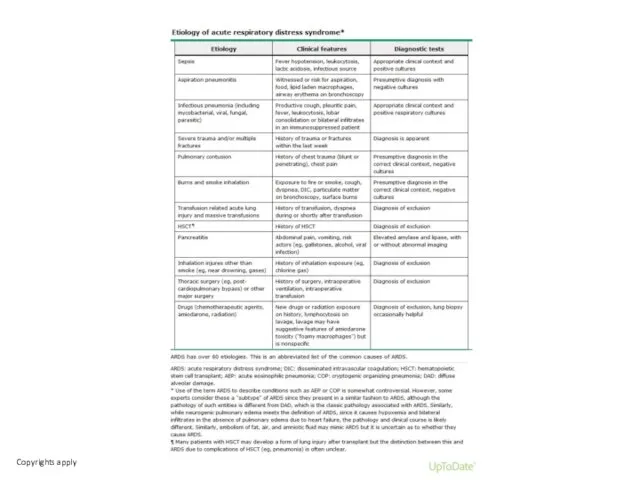
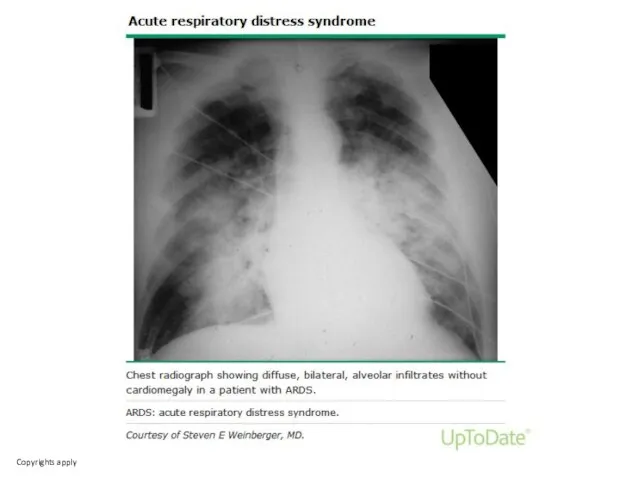
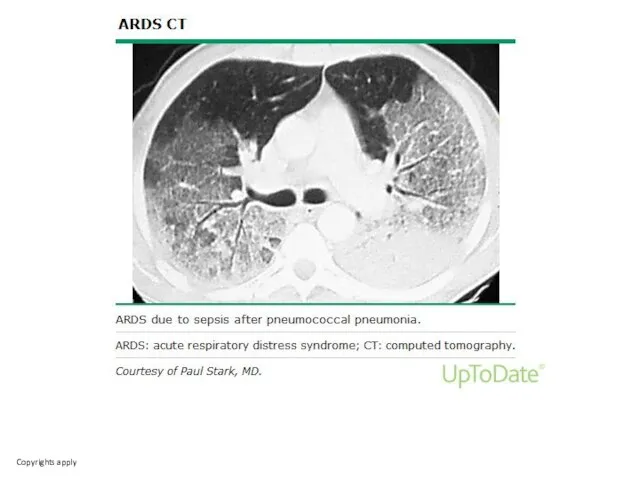
- 34. A variety of conditions may present as acute hypoxemic respiratory failure with bilateral alveolar opacities. Acute
- 36. Скачать презентацию
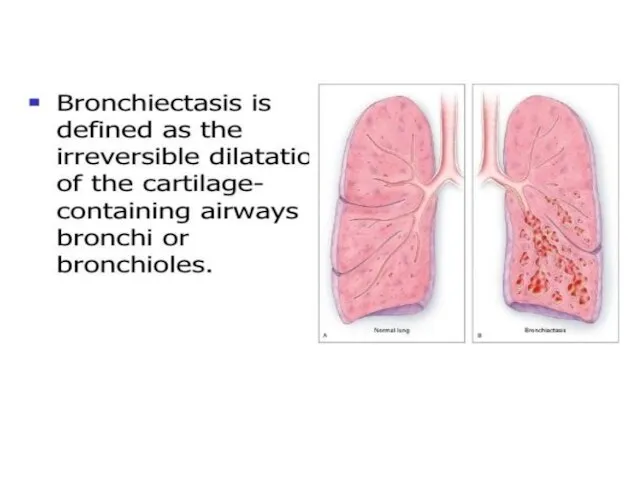
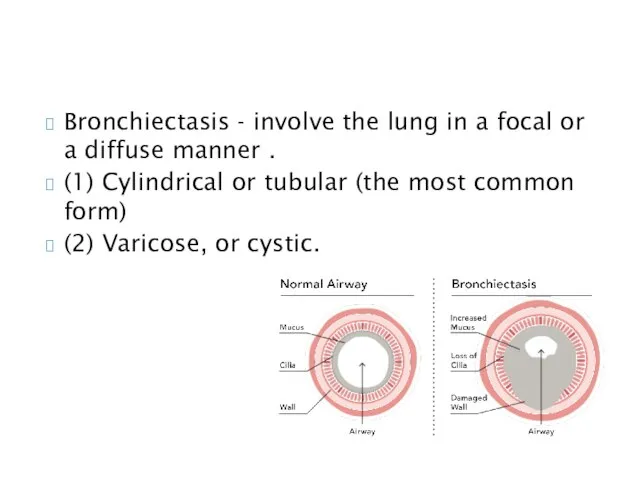
Bronchiectasis - involve the lung in a focal or a diffuse
Bronchiectasis - involve the lung in a focal or a diffuse
Bronchiectasis with predominant involvement of the :
Upper lung fields:
Cystic fibrosis (CF)
Bronchiectasis with predominant involvement of the :
Upper lung fields:
Cystic fibrosis (CF)
The incidence of bronchiectasis increases with age.
Bronchiectasis is more common among
The incidence of bronchiectasis increases with age.
Bronchiectasis is more common among
The most common clinical presentation is a persistent productive cough with
The most common clinical presentation is a persistent productive cough with
Physical findings:
1. crackles
2. wheezing
3.clubbing of the digits(some patients).
Physical findings:
1. crackles
2. wheezing
3.clubbing of the digits(some patients).
Pulmonary function tests: mild to moderate airflow obstruction, overlapping with that
Pulmonary function tests: mild to moderate airflow obstruction, overlapping with that
Airway dilation (detected as parallel "tram tracks" or as the "signet-ring
Airway dilation (detected as parallel "tram tracks" or as the "signet-ring
1. Control of active infection
2. Minimlize the risk of repeated
1. Control of active infection
2. Minimlize the risk of repeated
Numerous approaches used to enhance
secretion clearance include:
hydration
mucolytic administration,
aerosolization of bronchodilators
Numerous approaches used to enhance
secretion clearance include:
hydration
mucolytic administration,
aerosolization of bronchodilators
In select cases, surgery can be considered, with resection of a
In select cases, surgery can be considered, with resection of a
Outcomes of bronchiectasis can vary widely with:
the underlying etiology
the frequency
Outcomes of bronchiectasis can vary widely with:
the underlying etiology
the frequency
Trying to decrease the risk of recurrent infections by:
Reversal of an
Trying to decrease the risk of recurrent infections by:
Reversal of an
Administration of an oral antibiotic (e.g. ciprofloxacin) daily for 1-2 weeks
ARDS
ARDS
ARDS is an acute, diffuse, inflammatory form of lung injury that
ARDS is an acute, diffuse, inflammatory form of lung injury that
A variety of conditions may present as acute hypoxemic respiratory failure
A variety of conditions may present as acute hypoxemic respiratory failure
 АИВ-инфекциясының терапиясы және алдын алуы
АИВ-инфекциясының терапиясы және алдын алуы Брюшина. Брюшная полость
Брюшина. Брюшная полость Отравление рыбой
Отравление рыбой Ступени развития любви к себе
Ступени развития любви к себе Цереброваскулярлы аурулар. Жіктелуі, патогенезі, жедел бас ми қан айналымының клиникасы
Цереброваскулярлы аурулар. Жіктелуі, патогенезі, жедел бас ми қан айналымының клиникасы Врожденные пороки сердца у детей
Врожденные пороки сердца у детей Патология щитовидной железы. Тиреотоксикоз
Патология щитовидной железы. Тиреотоксикоз Лекарства
Лекарства Preventive measures of neurological diseases
Preventive measures of neurological diseases Первая медицинская помощь при поражении электрическим током
Первая медицинская помощь при поражении электрическим током Тубулоинтерстициальные нефропатии
Тубулоинтерстициальные нефропатии Адамды клондаудың моральды мәселелері
Адамды клондаудың моральды мәселелері Temporary fillings
Temporary fillings Дети с нарушением речи
Дети с нарушением речи Мотивация. Успех любого намерения зависит от цели. Урок №2
Мотивация. Успех любого намерения зависит от цели. Урок №2 Периферическая нервная система. Спинномозговые нервы
Периферическая нервная система. Спинномозговые нервы Психосоматика
Психосоматика Хронические лимфопролиферативные заболевания
Хронические лимфопролиферативные заболевания Дезинфекция растворами, газами, аэрозолями
Дезинфекция растворами, газами, аэрозолями Особенности питания детей, нуждающихся в паллиативной медицинской помощи
Особенности питания детей, нуждающихся в паллиативной медицинской помощи Рецептура (receptum). Образец рецепта
Рецептура (receptum). Образец рецепта Логопедическая ритмика в системе коррекционно – речевой работы с детьми - дошкольниками
Логопедическая ритмика в системе коррекционно – речевой работы с детьми - дошкольниками Рациональное питание
Рациональное питание Сестринский уход при объемных процессах центральной нервной системы. Эпилепсия. Судорожный синдром
Сестринский уход при объемных процессах центральной нервной системы. Эпилепсия. Судорожный синдром Бактеріальні хвороби риб
Бактеріальні хвороби риб Глобальная регуляция экспрессии генов
Глобальная регуляция экспрессии генов Балалардағы мальабсорбция синдромы. Целиакия. Дисахаридазды жетіспеушілік. Экссудативті энтеропатия
Балалардағы мальабсорбция синдромы. Целиакия. Дисахаридазды жетіспеушілік. Экссудативті энтеропатия Культура питания. Примерные рекомендации пациентам по правильному питанию
Культура питания. Примерные рекомендации пациентам по правильному питанию