- Medical Helmintology

Содержание
- 2. Medical helminthology is concerned with the study of helminthes or parasitic worms. Helminthes are trophoblastic metazoa
- 3. Transmission of helmintes: The sources of the parasites are different. Exposure of humans to the parasites
- 4. MEDICALLY IMPORTANT TREMATODES (FLUKES) 1. BLOOD FLUKES
- 5. Schistosomiasis. Shistosoma spp. It is estimated that about 600 million people in 79 countries suffer from
- 6. Definitive host: man, Intermediate host: freshwater snail Infective stage: cercariae (larvae) cercaria Adult male and female
- 7. Morphology Schistosoma mansoni. Habitat - This species lives in the veins of the intestine. Geographical distribution:
- 9. Symptoms Patients infected with S. haematobium suffer from terminal haematuria and painful micturition. There is inflammation
- 10. Diagnosis S. mansoni: ♦ Microscopic examination of the stool for eggs after concentration by sedimentation method.
- 11. Treatment Praziquantel: single oral dose of 40 mg/kg divided into two doses. Metriphonate 7.5 mg/kg. weekly
- 12. 2. LIVER FLUKES
- 13. Clonorchiasis. Clonorchis sinensis Morphology. Chinese liver fluke - adult worms live in bile ducts. Adult worm.
- 14. Symptoms: The migration of the larva up the bile duct induces desquamation, followed by hyperplasia, and
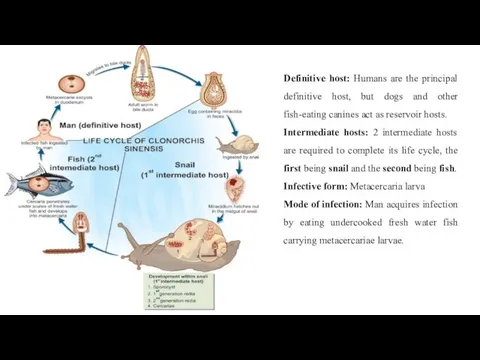
- 15. Definitive host: Humans are the principal definitive host, but dogs and other fish-eating canines act as
- 16. Treatment: Drug of choice is Praziquantel 25 mg/kg, 3 doses in 1 day. Surgical intervention may
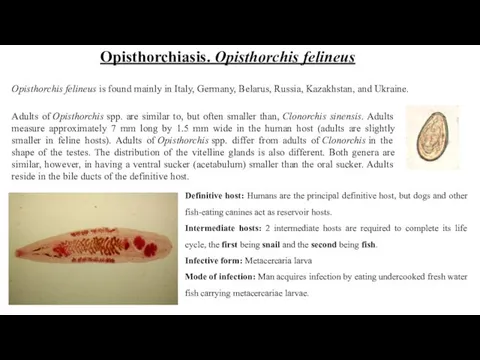
- 17. Adults of Opisthorchis spp. are similar to, but often smaller than, Clonorchis sinensis. Adults measure approximately
- 19. Diagnosis: Microscopic identification of eggs in stool specimens. The adult fluke can also be recovered at
- 20. Diagnosis: stool examinations Imaging (ultrasound, CT, MRI). Serologic testing Treatment: Praziquantel, adults, 75mg/kg/day orally, three doses
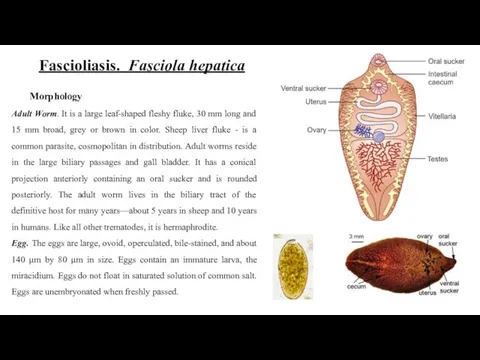
- 21. Fascioliasis. Fasciola hepatica Morphology Adult Worm. It is a large leaf-shaped fleshy fluke, 30 mm long
- 22. Symptoms: In traversing the liver tissue, it causes parenchymal injury. As humans are not its primary
- 23. Diagnosis: Stool Microscopy Blood Picture Serodiagnosis Imaging (USG, CT scan, Endoscopic Retrograde Choangiopancreatography (ERCP) and percutaneous
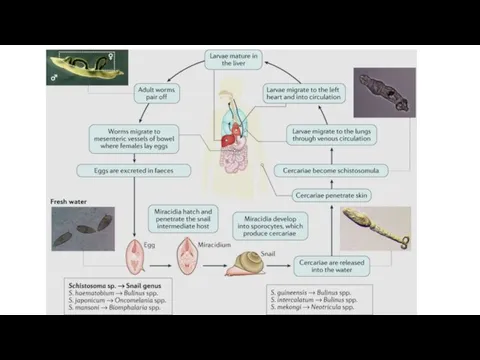
- 24. Life Cycle F. hepatica passes its life cycle in 1 definitive host and 2 intermediate hosts.
- 26. Скачать презентацию
Medical helminthology is concerned with the study of helminthes or parasitic
Medical helminthology is concerned with the study of helminthes or parasitic
Transmission of helmintes:
The sources of the parasites are different. Exposure of
Transmission of helmintes:
The sources of the parasites are different. Exposure of
MEDICALLY IMPORTANT
TREMATODES (FLUKES)
1. BLOOD FLUKES
MEDICALLY IMPORTANT
TREMATODES (FLUKES)
1. BLOOD FLUKES
Schistosomiasis. Shistosoma spp.
It is estimated that about 600 million people in
Schistosomiasis. Shistosoma spp.
It is estimated that about 600 million people in
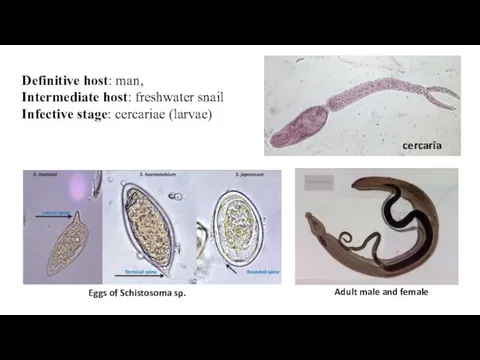
Definitive host: man,
Intermediate host: freshwater snail
Infective stage: cercariae (larvae)
cercaria
Adult male and
Definitive host: man,
Intermediate host: freshwater snail
Infective stage: cercariae (larvae)
cercaria
Adult male and

Morphology
Schistosoma mansoni. Habitat - This species lives in the veins of
Morphology
Schistosoma mansoni. Habitat - This species lives in the veins of

Symptoms
Patients infected with S. haematobium suffer from terminal haematuria and
Symptoms
Patients infected with S. haematobium suffer from terminal haematuria and

Diagnosis
S. mansoni:
♦ Microscopic examination of the stool for eggs after concentration
Diagnosis
S. mansoni:
♦ Microscopic examination of the stool for eggs after concentration
Treatment
Praziquantel: single oral dose of 40 mg/kg divided into two doses.
Treatment
Praziquantel: single oral dose of 40 mg/kg divided into two doses.

2. LIVER FLUKES
2. LIVER FLUKES
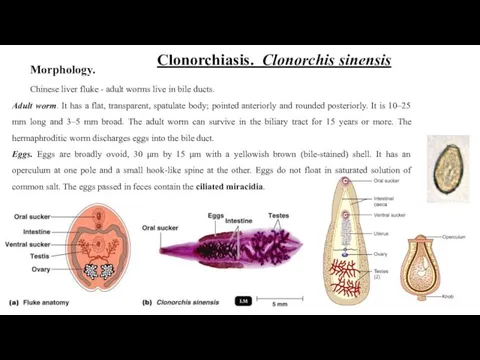
Clonorchiasis. Clonorchis sinensis
Morphology.
Chinese liver fluke - adult worms live in bile
Clonorchiasis. Clonorchis sinensis
Morphology.
Chinese liver fluke - adult worms live in bile
Symptoms:
The migration of the larva up the bile duct induces desquamation,
Symptoms:
The migration of the larva up the bile duct induces desquamation,
Definitive host: Humans are the principal definitive host, but dogs and
Definitive host: Humans are the principal definitive host, but dogs and
Treatment:
Drug of choice is Praziquantel 25 mg/kg, 3 doses in
Treatment:
Drug of choice is Praziquantel 25 mg/kg, 3 doses in
Adults of Opisthorchis spp. are similar to, but often smaller than, Clonorchis sinensis. Adults
Adults of Opisthorchis spp. are similar to, but often smaller than, Clonorchis sinensis. Adults

Diagnosis:
Microscopic identification of eggs in stool specimens.
The adult fluke can also
Diagnosis:
Microscopic identification of eggs in stool specimens.
The adult fluke can also
Diagnosis:
stool examinations
Imaging (ultrasound, CT, MRI).
Serologic testing
Treatment:
Praziquantel,
Diagnosis:
stool examinations
Imaging (ultrasound, CT, MRI).
Serologic testing
Treatment:
Praziquantel,
Fascioliasis. Fasciola hepatica
Morphology
Adult Worm. It is a large leaf-shaped fleshy fluke,
Fascioliasis. Fasciola hepatica
Morphology
Adult Worm. It is a large leaf-shaped fleshy fluke,

Symptoms:
In traversing the liver tissue, it causes parenchymal injury.
As humans are
Symptoms:
In traversing the liver tissue, it causes parenchymal injury.
As humans are
Diagnosis:
Stool Microscopy
Blood Picture
Serodiagnosis
Imaging (USG, CT scan, Endoscopic Retrograde Choangiopancreatography (ERCP) and
Diagnosis:
Stool Microscopy
Blood Picture
Serodiagnosis
Imaging (USG, CT scan, Endoscopic Retrograde Choangiopancreatography (ERCP) and
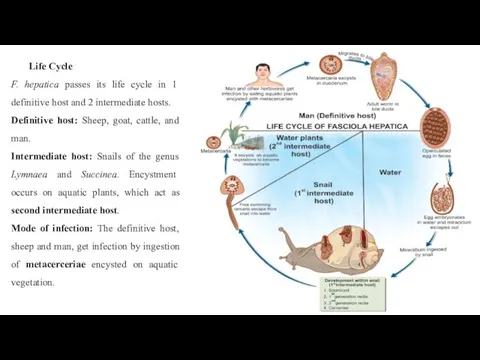
Life Cycle
F. hepatica passes its life cycle in 1 definitive host
Life Cycle
F. hepatica passes its life cycle in 1 definitive host
 Болезни рыб. Диагностика и лечение
Болезни рыб. Диагностика и лечение Невропатология и дефектология
Невропатология и дефектология Situația epidemiologică privind infecția covid-19
Situația epidemiologică privind infecția covid-19 Науқастың жеке бас гигиенасы
Науқастың жеке бас гигиенасы Инфекции, передающиеся парентеральным путем (вирусные гепатиты В,С,Д, ВИЧ-инфекция)
Инфекции, передающиеся парентеральным путем (вирусные гепатиты В,С,Д, ВИЧ-инфекция) Қала және ауыл тұрғындары арасында. Созылмалы жүрек жеткіліксіздігі бар науқастардың
Қала және ауыл тұрғындары арасында. Созылмалы жүрек жеткіліксіздігі бар науқастардың Методики обогащения биологического материала(методы седиментации и флотации)
Методики обогащения биологического материала(методы седиментации и флотации) Сахарный диабет
Сахарный диабет Терінің вирусты аурулары
Терінің вирусты аурулары Аномалии конституции. Синдром внезапной смерти
Аномалии конституции. Синдром внезапной смерти Патофизиология клетки
Патофизиология клетки Туберкулез
Туберкулез Дуглас Дж. Ри Глаукома
Дуглас Дж. Ри Глаукома Аритмиялар
Аритмиялар Неотложные состояния при эндокринных заболеваниях (часть I)
Неотложные состояния при эндокринных заболеваниях (часть I) Строение и пластика черепа
Строение и пластика черепа Асқынған босану және кесар тілігі операциясынан кейінгі босанғаннан кейінгі кезеңді жүргізудің ерекшеліктері
Асқынған босану және кесар тілігі операциясынан кейінгі босанғаннан кейінгі кезеңді жүргізудің ерекшеліктері Bronchitis
Bronchitis Острая дыхательная недостаточность
Острая дыхательная недостаточность Дополнительные методы диагностики при черепно-мозговой травме. Показания к оперативному лечению
Дополнительные методы диагностики при черепно-мозговой травме. Показания к оперативному лечению Стресс. Виды стресса. Эмоциональный стресс. Клинические проявления стресса
Стресс. Виды стресса. Эмоциональный стресс. Клинические проявления стресса Эндокринная система
Эндокринная система Презентация 1
Презентация 1 Профилактика психических заболеваний
Профилактика психических заболеваний Миотония. Пароксизмальная миоплегия
Миотония. Пароксизмальная миоплегия Перефкрическая сенсо-моторная нейропатия у больных сахарным диабетом 2 типа
Перефкрическая сенсо-моторная нейропатия у больных сахарным диабетом 2 типа Внебольничная остановка сердца: комплекс кардиопульмональной реанимации на догоспитальном этапе у взрослого пациента
Внебольничная остановка сердца: комплекс кардиопульмональной реанимации на догоспитальном этапе у взрослого пациента Стратегические направления деятельности больницы
Стратегические направления деятельности больницы