- Red blood cells pathology. (Subject 10)

Содержание
- 2. Lecture Plan Blood volume changes Anemia classifications Clinical features and specific signs of anemias Erythrocytosis (Polycytemia)
- 3. Hypervolemia transfusion of blood large doses; during intensive physical work Vaquez' disease , hypoxia diseases of
- 4. Hypovolemia dehydration (diarrhoea, vomiting, abundant sweating, burns, overheating), shock in the second stage of acute blood
- 5. Anemia Anemia is a lack of red blood cells and/or hemoglobin. This results in a hypoxia
- 6. Anemia classifications Pathogenic classification. Posthemorrhagic (acute or chronic). Haemolytic - acute and chronic. Chronic haemolytic anaemias
- 7. Anemia classifications Classification due to haemoglobin content in RBC. Normally haemoglobin content in erythrocyte is 0,8—1,05.
- 8. Anemia classifications Classification based on the on the type of RBC maturation. erythroblastic anemias megaloblastic anemias
- 9. Clinical features of anemia olygocythemic normovolemia (in most anemias); hypovolemia (acute posthemorrhagic anaemia, pernicious anaemia); paleness
- 10. Clinical features of anemia Decreased function of endocrine organs (especially thyroid gland); GIT: anorexia, flatulence, nausea,
- 11. Specific signs of anemias Posthemorrhagic anaemia – signs of blood loss from different organs; Iron deficiency
- 12. Regenerative forms of RBC Bone marrow Peripheral blood Normal state Increased demands
- 13. Degenerative forms of RBC Poikilocytosis – abnormal variation in shape target cell sickle cell Anisocytosis –
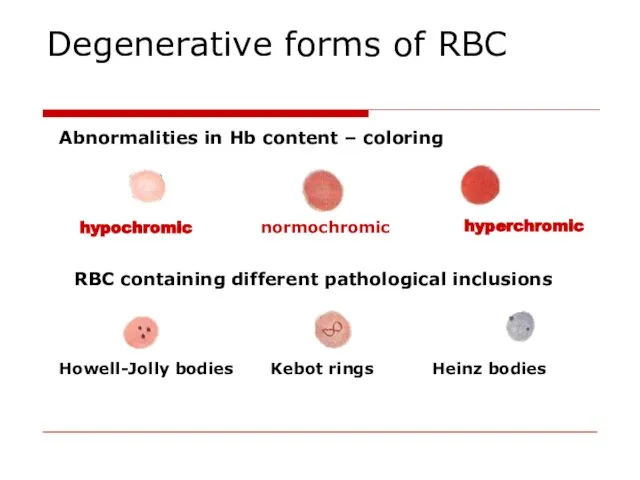
- 14. Degenerative forms of RBC Abnormalities in Hb content – coloring hypochromic normochromic RBC containing different pathological
- 15. Anemia of blood loss The main reasons of blood loss: blood vessels or heart walls safety
- 16. Acute posthemorrhagic anemia 1st stage – heart rate and blood vessel tonus are increased, centralization of
- 17. Principles of blood loss therapy Etiologic treatment: the increasing of blood coagulation, the reconstruction of vessel
- 18. Chronic posthemorrhagic anaemia RBC number and Hb content is decreased Hypochromic (colour index is 0,6-0,4) This
- 19. Chronic posthemorrhagic anaemia Regeneratory stage: Hb, RBC, colour index are lower that normal. Its duration depends
- 20. Hemolytic Anemias Types of hemolysis Extravascular (common) – occurs in phagocytic cells of the spleen, liver,
- 21. Hemolytic Anemias Classification Acute Chronic Acquired Inherited immune mechanical injury toxic effects RES hyperactivity
- 22. Acquired hemolytic anemias Immune abnormalities due to antibodies production: against own undamaged RBC (autoimmune hemolytic anemia);
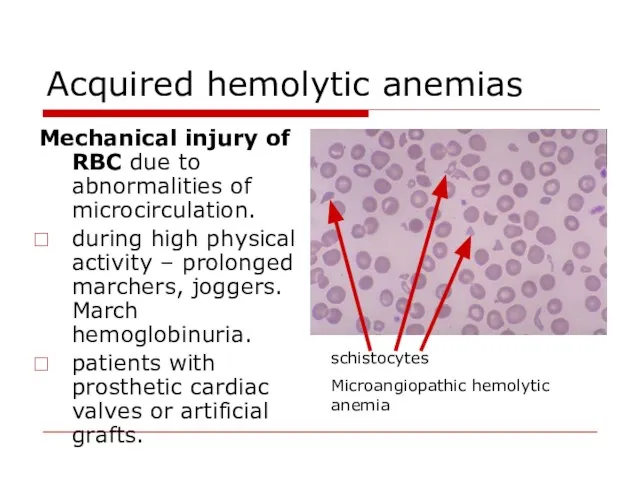
- 23. Acquired hemolytic anemias Mechanical injury of RBC due to abnormalities of microcirculation. during high physical activity
- 24. Acquired hemolytic anemias Direct toxic effect Infectious agents toxic effect (α- or β-hemolytic streptococci, meningococci) Invasion
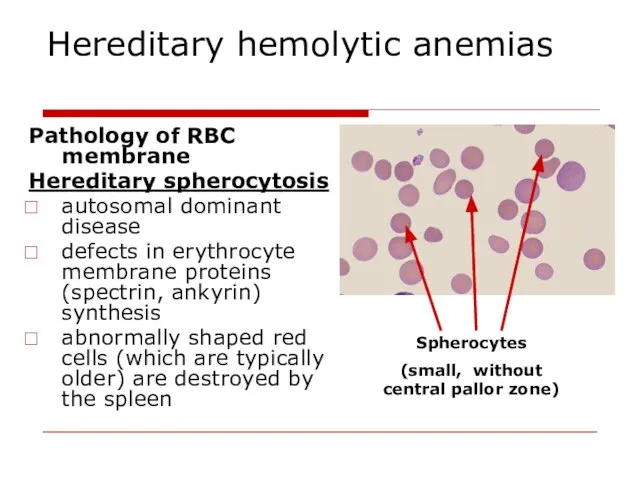
- 25. Hereditary hemolytic anemias Pathology of RBC membrane Hereditary spherocytosis autosomal dominant disease defects in erythrocyte membrane
- 26. Hereditary hemolytic anemias Pathology of RBC enzymes Glucose-6-phosphate dehydrogenase deficiency. X-linked recessive G6PD is necessary for
- 27. Hereditary hemolytic anemias Pathology of haemoglobin Sickle cell disease is a qualitative disorder of Hb (abnormal
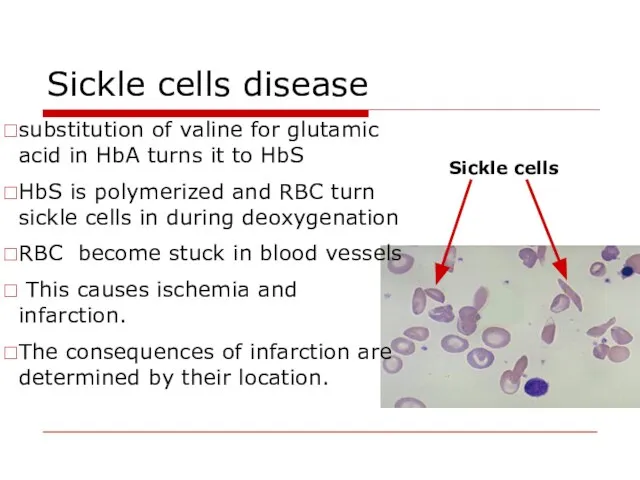
- 28. Sickle cells disease substitution of valine for glutamic acid in HbA turns it to HbS HbS
- 29. Thalassemia classification α thalassemia, the production of α globin is deficient β thalassemia the production of
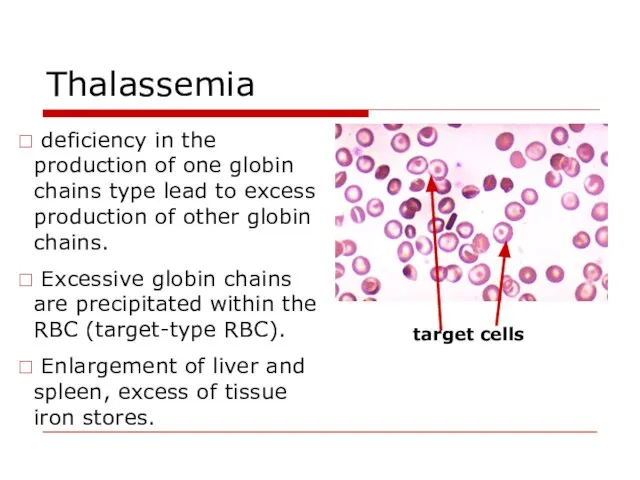
- 30. Thalassemia deficiency in the production of one globin chains type lead to excess production of other
- 31. Anemias caused by disturbances of haemopoiesis Iron deficiency reasons: chronic blood losses due to - excessive
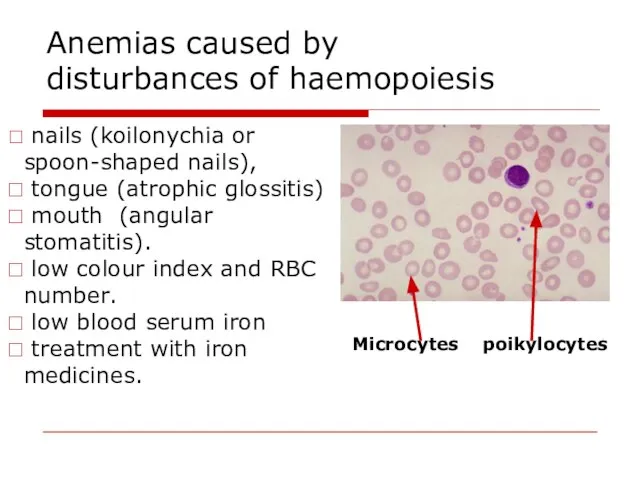
- 32. Anemias caused by disturbances of haemopoiesis nails (koilonychia or spoon-shaped nails), tongue (atrophic glossitis) mouth (angular
- 33. Anemias caused by disturbances of haemopoiesis Syderoblastic anemia (refractory to iron) defect enzymes that include iron
- 34. Anemias caused by disturbances of haemopoiesis Megaloblastic anaemia deficiency of vitamin B12 and folic acid. impaired
- 35. Megaloblastic anemia The reasons of B12 deficiency: inadequate dietary intake (strict vegetarians) inadequate production of intrinsic
- 36. Vitamin B12 metabolism transport by transcobalamin haemopoiesis combines with intrinsic factor absorption myelination of nervous fibers
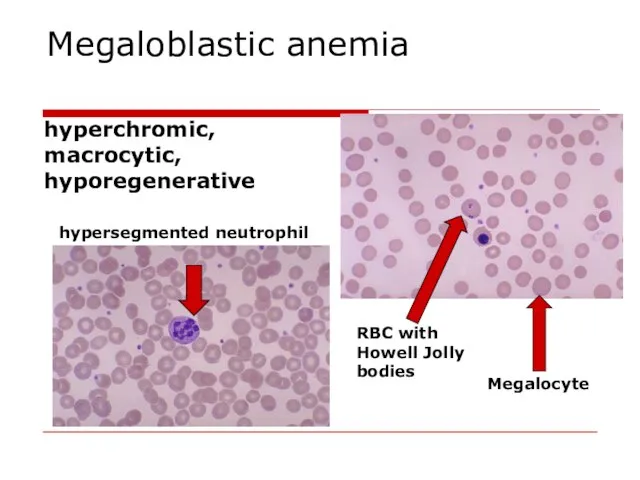
- 37. Megaloblastic anemia hyperchromic, macrocytic, hyporegenerative hypersegmented neutrophil RBC with Howell Jolly bodies Megalocyte
- 38. Megaloblastic anemia Specific clinical features of megaloblastic anemia: glossitis (inflammation of the tongue; smooth, beefy, red
- 39. Anemias caused by disturbances of haemopoiesis Hypoplastic and aplastic anaemias etiology: medicines with myelotoxic effect (amidopyrine,
- 40. Anemias caused by disturbances of haemopoiesis The picture of blood – pancytopenia – decrease of all
- 41. Anemias caused by disturbances of haemopoiesis Metaplastic anaemias etiology: leukemic metaplasia of bone marrow (it consists
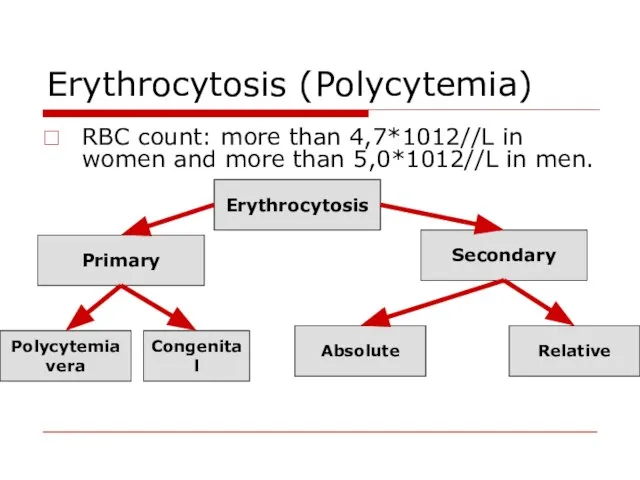
- 42. Erythrocytosis (Polycytemia) RBC count: more than 4,7*1012//L in women and more than 5,0*1012//L in men. Erythrocytosis
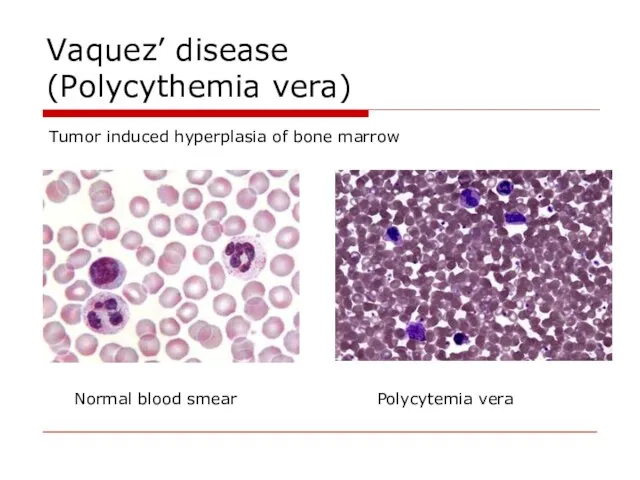
- 43. Vaquez’ disease (Polycythemia vera) Tumor induced hyperplasia of bone marrow Normal blood smear Polycytemia vera
- 44. Vaquez’ disease (Polycythemia vera) Blood count: increased number of RBC, reticulocytes, WBC and platelets. Blood volume
- 45. Vaquez’ disease (Polycythemia vera) Clinical signs arterial hypertension ; plethora with congested mucous membranes conjunctiva and
- 46. Secondary absolute erythrocytosis due to increased erythropoietin production General hypoxia: Chronic lung diseases; Carbon monoxide poisoning;
- 48. Скачать презентацию
Lecture Plan
Blood volume changes
Anemia classifications
Clinical features and specific signs of anemias
Erythrocytosis
Lecture Plan
Blood volume changes
Anemia classifications
Clinical features and specific signs of anemias
Erythrocytosis
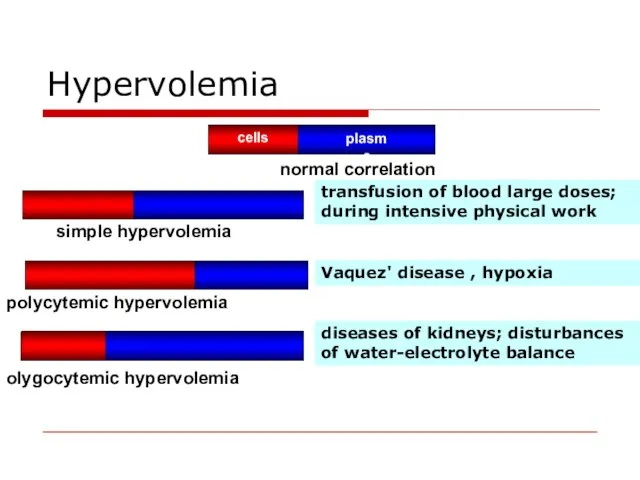
Hypervolemia
transfusion of blood large doses; during intensive physical work
Vaquez' disease
Hypervolemia
transfusion of blood large doses; during intensive physical work
Vaquez' disease
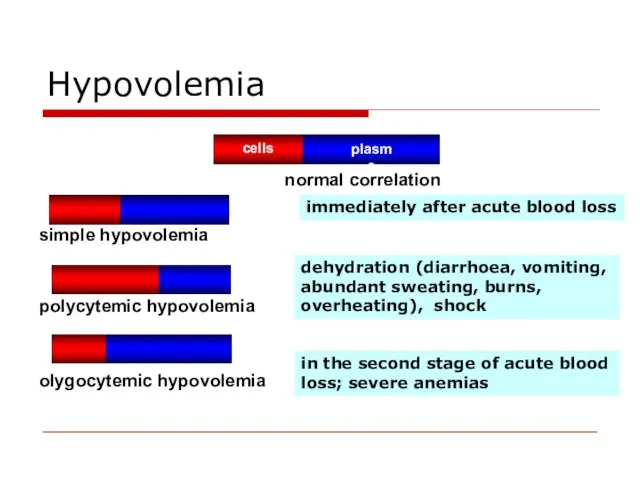
Hypovolemia
dehydration (diarrhoea, vomiting, abundant sweating, burns, overheating), shock
in the second
Hypovolemia
dehydration (diarrhoea, vomiting, abundant sweating, burns, overheating), shock
in the second
Anemia
Anemia is a lack of red blood cells and/or hemoglobin. This
Anemia
Anemia is a lack of red blood cells and/or hemoglobin. This
Anemia classifications
Pathogenic classification.
Posthemorrhagic (acute or chronic).
Haemolytic - acute and chronic.
Anemia classifications
Pathogenic classification.
Posthemorrhagic (acute or chronic).
Haemolytic - acute and chronic.
Anemia classifications
Classification due to haemoglobin content in RBC.
Normally haemoglobin content
Anemia classifications
Classification due to haemoglobin content in RBC.
Normally haemoglobin content
Anemia classifications
Classification based on the on the type of RBC maturation.
Anemia classifications
Classification based on the on the type of RBC maturation.
Clinical features of anemia
olygocythemic normovolemia (in most anemias);
hypovolemia (acute posthemorrhagic
Clinical features of anemia
olygocythemic normovolemia (in most anemias);
hypovolemia (acute posthemorrhagic
Clinical features of anemia
Decreased function of endocrine organs (especially thyroid gland);
GIT:
Clinical features of anemia
Decreased function of endocrine organs (especially thyroid gland);
GIT:
Specific signs of anemias
Posthemorrhagic anaemia – signs of blood loss from
Specific signs of anemias
Posthemorrhagic anaemia – signs of blood loss from
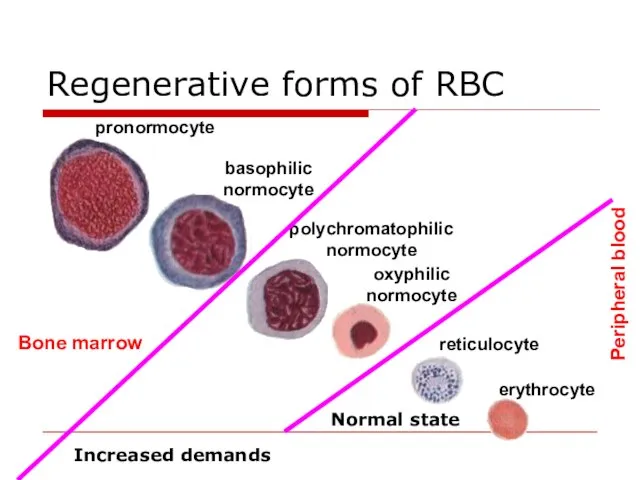
Regenerative forms of RBC
Bone marrow
Peripheral blood
Normal state
Increased demands
Regenerative forms of RBC
Bone marrow
Peripheral blood
Normal state
Increased demands
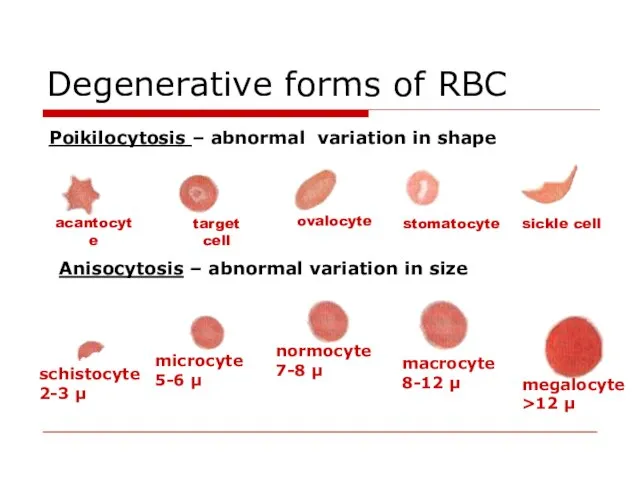
Degenerative forms of RBC
Poikilocytosis – abnormal variation in shape
target cell
sickle cell
Anisocytosis
Degenerative forms of RBC
Poikilocytosis – abnormal variation in shape
target cell
sickle cell
Anisocytosis
Degenerative forms of RBC
Abnormalities in Hb content – coloring
hypochromic
normochromic
RBC containing
Degenerative forms of RBC
Abnormalities in Hb content – coloring
hypochromic
normochromic
RBC containing
Anemia of blood loss
The main reasons of blood loss:
blood vessels or
Anemia of blood loss
The main reasons of blood loss:
blood vessels or
Acute posthemorrhagic anemia
1st stage – heart rate and blood vessel tonus
Acute posthemorrhagic anemia
1st stage – heart rate and blood vessel tonus
Principles of blood loss therapy
Etiologic treatment: the increasing of blood coagulation,
Principles of blood loss therapy
Etiologic treatment: the increasing of blood coagulation,
Chronic posthemorrhagic anaemia
RBC number and Hb content is decreased
Hypochromic (colour
Chronic posthemorrhagic anaemia
RBC number and Hb content is decreased
Hypochromic (colour
Chronic posthemorrhagic anaemia
Regeneratory stage: Hb, RBC, colour index are lower that
Chronic posthemorrhagic anaemia
Regeneratory stage: Hb, RBC, colour index are lower that
Hemolytic Anemias
Types of hemolysis
Extravascular (common) – occurs in phagocytic cells of
Hemolytic Anemias
Types of hemolysis
Extravascular (common) – occurs in phagocytic cells of
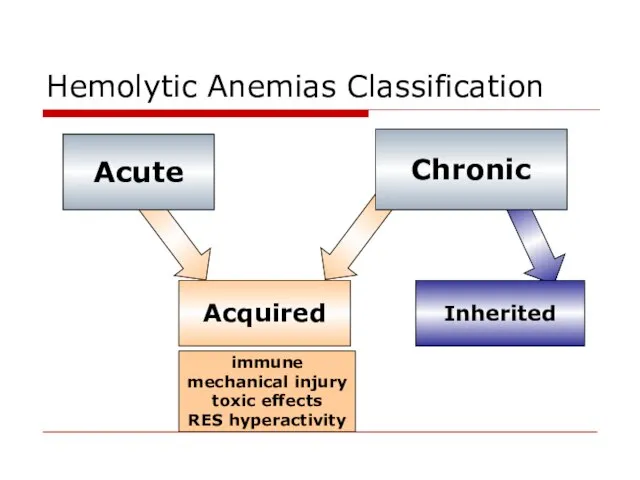
Hemolytic Anemias Classification
Acute
Chronic
Acquired
Inherited
immune
mechanical injury
toxic effects
RES hyperactivity
Hemolytic Anemias Classification
Acute
Chronic
Acquired
Inherited
immune
mechanical injury
toxic effects
RES hyperactivity
Acquired hemolytic anemias
Immune abnormalities due to antibodies production:
against own undamaged
Acquired hemolytic anemias
Immune abnormalities due to antibodies production:
against own undamaged
Acquired hemolytic anemias
Mechanical injury of RBC due to abnormalities of microcirculation.
Acquired hemolytic anemias
Mechanical injury of RBC due to abnormalities of microcirculation.
Acquired hemolytic anemias
Direct toxic effect
Infectious agents toxic effect (α- or
Acquired hemolytic anemias
Direct toxic effect
Infectious agents toxic effect (α- or
Hereditary hemolytic anemias
Pathology of RBC membrane
Hereditary spherocytosis
autosomal dominant disease
Hereditary hemolytic anemias
Pathology of RBC membrane
Hereditary spherocytosis
autosomal dominant disease
Hereditary hemolytic anemias
Pathology of RBC enzymes
Glucose-6-phosphate dehydrogenase deficiency.
X-linked recessive
G6PD
Hereditary hemolytic anemias
Pathology of RBC enzymes
Glucose-6-phosphate dehydrogenase deficiency.
X-linked recessive
G6PD
Hereditary hemolytic anemias
Pathology of haemoglobin
Sickle cell disease is a qualitative
Hereditary hemolytic anemias
Pathology of haemoglobin
Sickle cell disease is a qualitative
Sickle cells disease
substitution of valine for glutamic acid in HbA turns
Sickle cells disease
substitution of valine for glutamic acid in HbA turns
Thalassemia classification
α thalassemia, the production of α globin is deficient
β thalassemia
Thalassemia classification
α thalassemia, the production of α globin is deficient
β thalassemia
Thalassemia
deficiency in the production of one globin chains type lead
Thalassemia
deficiency in the production of one globin chains type lead
Anemias caused by
disturbances of haemopoiesis
Iron deficiency reasons:
chronic blood losses
Anemias caused by
disturbances of haemopoiesis
Iron deficiency reasons:
chronic blood losses
Anemias caused by
disturbances of haemopoiesis
nails (koilonychia or spoon-shaped nails),
Anemias caused by
disturbances of haemopoiesis
nails (koilonychia or spoon-shaped nails),
Anemias caused by
disturbances of haemopoiesis
Syderoblastic anemia (refractory to iron)
defect enzymes
Anemias caused by
disturbances of haemopoiesis
Syderoblastic anemia (refractory to iron)
defect enzymes
Anemias caused by
disturbances of haemopoiesis
Megaloblastic anaemia
deficiency of vitamin B12
Anemias caused by
disturbances of haemopoiesis
Megaloblastic anaemia
deficiency of vitamin B12
Megaloblastic anemia
The reasons of B12 deficiency:
inadequate dietary intake (strict vegetarians)
inadequate production
Megaloblastic anemia
The reasons of B12 deficiency:
inadequate dietary intake (strict vegetarians)
inadequate production
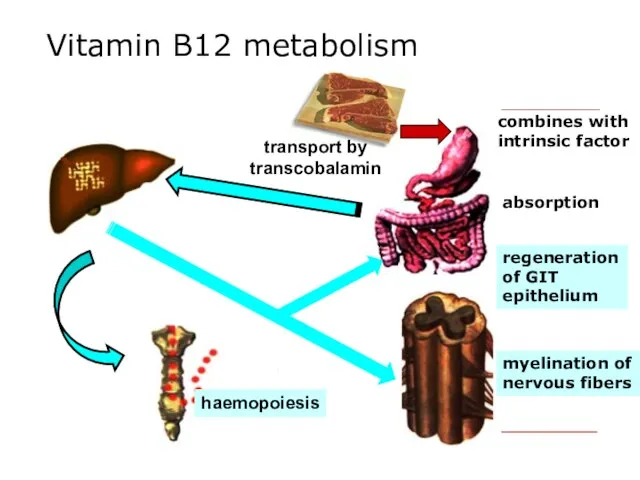
Vitamin B12 metabolism
transport by transcobalamin
haemopoiesis
combines with intrinsic factor
absorption
myelination of nervous
Vitamin B12 metabolism
transport by transcobalamin
haemopoiesis
combines with intrinsic factor
absorption
myelination of nervous
Megaloblastic anemia
hyperchromic, macrocytic, hyporegenerative
hypersegmented neutrophil
RBC with Howell Jolly bodies
Megalocyte
Megaloblastic anemia
hyperchromic, macrocytic, hyporegenerative
hypersegmented neutrophil
RBC with Howell Jolly bodies
Megalocyte
Megaloblastic anemia
Specific clinical features of megaloblastic anemia:
glossitis (inflammation of the
Megaloblastic anemia
Specific clinical features of megaloblastic anemia:
glossitis (inflammation of the
Anemias caused by
disturbances of haemopoiesis
Hypoplastic and aplastic anaemias etiology:
medicines with
Anemias caused by
disturbances of haemopoiesis
Hypoplastic and aplastic anaemias etiology:
medicines with
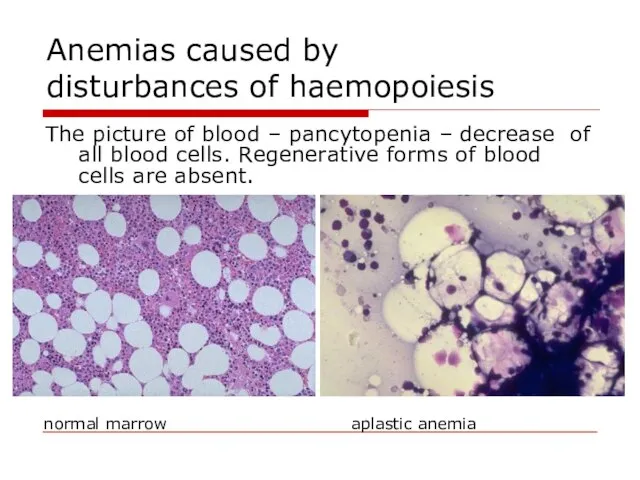
Anemias caused by
disturbances of haemopoiesis
The picture of blood – pancytopenia
Anemias caused by
disturbances of haemopoiesis
The picture of blood – pancytopenia
Anemias caused by
disturbances of haemopoiesis
Metaplastic anaemias etiology:
leukemic metaplasia of bone
Anemias caused by
disturbances of haemopoiesis
Metaplastic anaemias etiology:
leukemic metaplasia of bone
Erythrocytosis (Polycytemia)
RBC count: more than 4,7*1012//L in women and more than
Erythrocytosis (Polycytemia)
RBC count: more than 4,7*1012//L in women and more than
Vaquez’ disease
(Polycythemia vera)
Tumor induced hyperplasia of bone marrow
Normal blood
Vaquez’ disease
(Polycythemia vera)
Tumor induced hyperplasia of bone marrow
Normal blood
Vaquez’ disease
(Polycythemia vera)
Blood count:
increased number of RBC, reticulocytes, WBC
Vaquez’ disease
(Polycythemia vera)
Blood count:
increased number of RBC, reticulocytes, WBC
Vaquez’ disease
(Polycythemia vera)
Clinical signs
arterial hypertension ;
plethora with congested mucous membranes
Vaquez’ disease
(Polycythemia vera)
Clinical signs
arterial hypertension ;
plethora with congested mucous membranes
Secondary absolute erythrocytosis
due to increased erythropoietin production
General hypoxia:
Chronic lung diseases;
Carbon
Secondary absolute erythrocytosis
due to increased erythropoietin production
General hypoxia:
Chronic lung diseases;
Carbon
 Всемирная неделя иммунизации, 2019 г
Всемирная неделя иммунизации, 2019 г Әкелерді қатыстыру
Әкелерді қатыстыру Медициналық этика мен деонтология
Медициналық этика мен деонтология Микробиология холеры
Микробиология холеры Рациональная антимикробная терапия
Рациональная антимикробная терапия Приобретенные пороки сердца
Приобретенные пороки сердца Заболевания щитовидной железы
Заболевания щитовидной железы Детские инфекции у детей: дифтерия, менингококковая инфекция
Детские инфекции у детей: дифтерия, менингококковая инфекция Механизм опухолевой трансформации клетки
Механизм опухолевой трансформации клетки Мочевые органы мочевыделительной системы
Мочевые органы мочевыделительной системы Проблемы межполушарной асимметрии и межполушарного взаимодействия
Проблемы межполушарной асимметрии и межполушарного взаимодействия Дыхательная гимнастика, разработанная А.Н. Стрельниковой. Применение в ЛФК
Дыхательная гимнастика, разработанная А.Н. Стрельниковой. Применение в ЛФК Иерсиниозы. Клиника и современные методы диагностики
Иерсиниозы. Клиника и современные методы диагностики Ауыл тұрғындарына ,бастапқы медико – санитарлық көмекті ұйымдастыру
Ауыл тұрғындарына ,бастапқы медико – санитарлық көмекті ұйымдастыру Familial Mediterranean fever (FMF)
Familial Mediterranean fever (FMF) Взаимосвязь уровня тревожности и акцентуаций характера у студентов ВУЗа
Взаимосвязь уровня тревожности и акцентуаций характера у студентов ВУЗа Современные проблемы многоплодной беременности
Современные проблемы многоплодной беременности Система и задачи судебной медицины
Система и задачи судебной медицины АИВ инфекциясымен ауыратын науқастағы вирусты гепатиттердің алдын алу және емдеудің ерекшеліктері
АИВ инфекциясымен ауыратын науқастағы вирусты гепатиттердің алдын алу және емдеудің ерекшеліктері Малярия
Малярия Ми қан айналым бұзылыс синдромдары
Ми қан айналым бұзылыс синдромдары Отбасыны сипаттау жүйесі
Отбасыны сипаттау жүйесі Здоровый образ жизни
Здоровый образ жизни Мутацияның молекулалық негіздері
Мутацияның молекулалық негіздері Болезнь Паркинсона
Болезнь Паркинсона Песочная терапия и её возможности в логопедической практике (часть 2)
Песочная терапия и её возможности в логопедической практике (часть 2) Ортопедиялық стоматологиядағы минимальды интервенция тұжырымдамасы
Ортопедиялық стоматологиядағы минимальды интервенция тұжырымдамасы Жүрек қарыншалары мен жүрекшелердің гипертрофиялық визуальді диагностика әдістері
Жүрек қарыншалары мен жүрекшелердің гипертрофиялық визуальді диагностика әдістері