- Renal cell carcinoma

Содержание
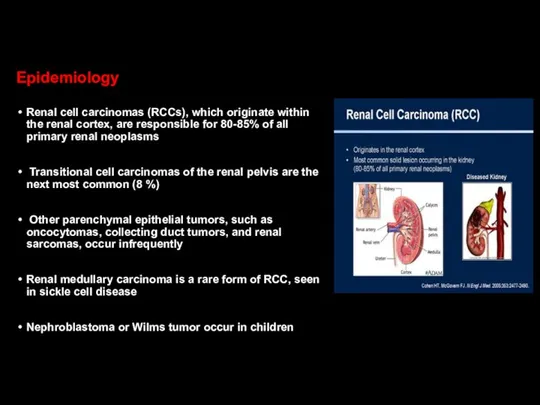
- 2. Epidemiology Renal cell carcinomas (RCCs), which originate within the renal cortex, are responsible for 80-85% of
- 3. Worldwide, in 2018, there were an estimated 403,000 new cases of RCC and 175,000 deaths due
- 4. RCC is approximately twofold more common in men compared with women RCC occurs predominantly in the
- 5. Some notable features of RCC include: Common diagnosis of asymptomatic disease Resistance to cytotoxic agents Relative
- 6. Survival The incidence of RCC has risen threefold higher than the mortality rate The five-year survival
- 7. Risk factors associated with a increased incidence of RCC Smoking Hypertension Obesity…. Otherwise, for patients with
- 8. Other risk factors associated with a increased incidence of RCC Acquired cystic disease of the kidney
- 9. Other risk factors associated with a increased incidence of RCC Occupational exposure to toxic compounds, such
- 10. Other risk factors associated with a increased incidence of RCC Cytotoxic chemotherapy — The use of
- 11. Other risk factors associated with a increased incidence of RCC Kidney stones---A history of kidney stones
- 12. Risk factors for RCC The risk of a second, metachronous RCC is increased in patients who
- 13. Other factors that modify risk Diabetes mellitus Polycystic kidney disease Alcohol (protective effect)? Childhood cancer survivors
- 14. Genetic factors Although most RCCs are sporadic, several syndromes associated with RCC have been described Factors
- 15. Von Hippel-Lindau (VHL) disease Von Hippel-Lindau (VHL) syndrome is characterized by germline mutation of VHL gene
- 16. Hemangioblastomas of CNS (cerebellum, brainstem, spinal cord) Retinal hemangioblastomas ccRCCs Pheochromocytomas Endolymphatic sac tumours of the
- 17. The pathogenesis of VHL disease has been linked to mutations in the VHL gene VHL protein,
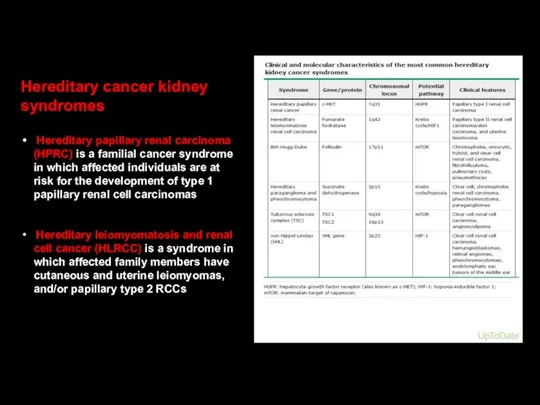
- 18. Hereditary cancer kidney syndromes Hereditary papillary renal carcinoma (HPRC) is a familial cancer syndrome in which
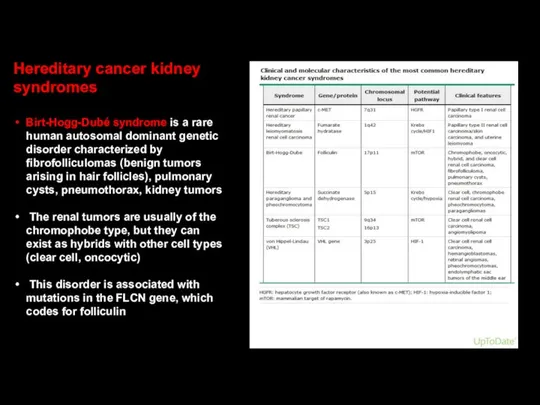
- 19. Hereditary cancer kidney syndromes Birt-Hogg-Dubé syndrome is a rare human autosomal dominant genetic disorder characterized by
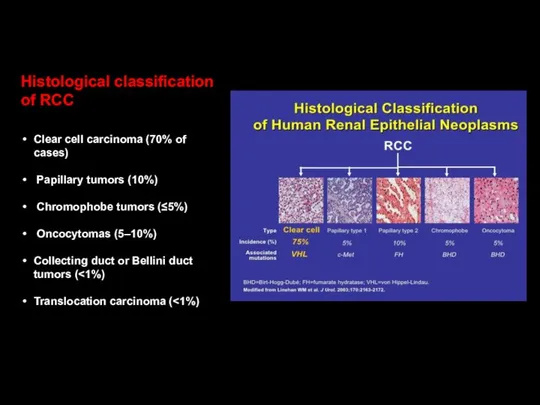
- 20. Histological classification of RCC Clear cell carcinoma (70% of cases) Papillary tumors (10%) Chromophobe tumors (≤5%)
- 21. Pathology RCC Papillary tumors tend to be bilateral and multifocal Chromophobe tumors have a more indolent
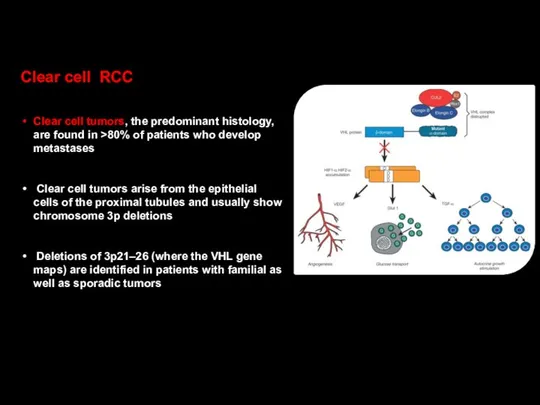
- 22. Clear cell RCC Clear cell tumors, the predominant histology, are found in >80% of patients who
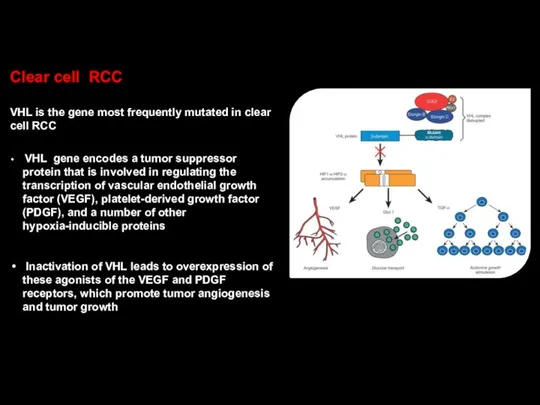
- 23. Clear cell RCC VHL is the gene most frequently mutated in clear cell RCC VHL gene
- 24. Important! Although these tumors have a clear clonal origin and often contain VHL mutations in common,
- 25. While VHL is the gene most frequently mutated in clear cell RCC (52% of cases), other
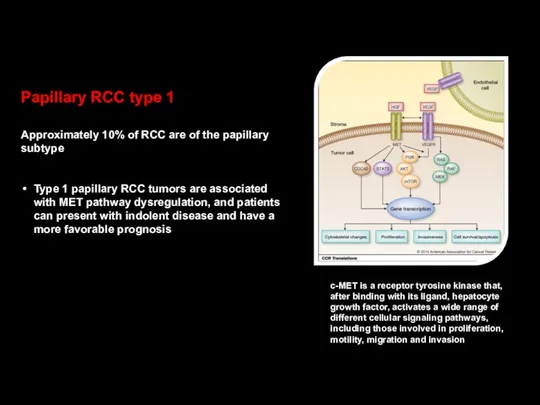
- 26. Papillary RCC type 1 Approximately 10% of RCC are of the papillary subtype Type 1 papillary
- 27. Papillary RCC type 2 ●Type 2 papillary RCC tumors may be characterized by sporadic gene mutations
- 28. Clinical presentation of RCC Hematuria Flank or abdominal pain Fever Weight loss Anemia Varicocele
- 29. The classic triad of RCC (flank pain, hematuria, and a palpable abdominal renal mass) occurs in
- 30. Scrotal varicocele, usually left sided, is observed in as many as 11 % of men with
- 31. Kidney cancer was called the “internist’s tumor” since it was often discovered from the initial presentation
- 32. At present time RCC most commonly detected as an incidental finding on a radiologic imaging Widespread
- 33. The standard evaluation of patients with renal mass CT scan of the abdomen and pelvis Chest
- 34. Any solid renal masses should be suspected malignant until proven otherwise The differential diagnosis of a
- 35. Staging is based on the American Joint Committee on Cancer (AJCC) staging system Stage I tumors
- 36. Staging is based on the American Joint Committee on Cancer (AJCC) staging system Stage III tumors
- 37. Staging and prognosis 65 % of patients present with stage I or II disease 15–20% with
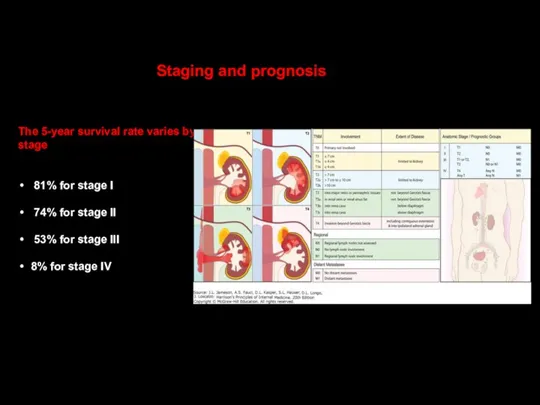
- 38. Staging and prognosis The 5-year survival rate varies by stage 81% for stage I 74% for
- 39. Prognostic risk models are helpful for counseling patients, and for anticipating survival rates when designing a
- 40. Prognostic risk models: IMDS
- 41. Treatment of localized RCC The standard management for stage I or II tumors and selected cases
- 42. Treatment of localized RCC Extension into the renal vein or inferior vena cava (stage III disease)
- 43. Nephron-sparing approaches via open or laparoscopic surgery may be appropriate for patients who have impaired renal
- 44. Radical nephrectomy can lead to an increased risk for chronic kidney disease and is associated with
- 45. Adjuvant therapy with interferon-α or radiation therapy following radical nephrectomy does not improve outcome, even in
- 46. The most common sites of distant metastases are the lungs, lymph nodes, liver, bone, and brain
- 47. Surgery has a limited role for patients with metastatic disease Long-term survival may occur in patients
- 48. Radiation therapy is generally used for palliation of bone or brain metastases The types of radiotherapy
- 49. Metastatic renal cell carcinoma is refractory to cytotoxic chemotherapy The fields of immunology and oncology have
- 50. Removal of primary RCCs can evoke an immune response that occasionally results in spontaneous and dramatic
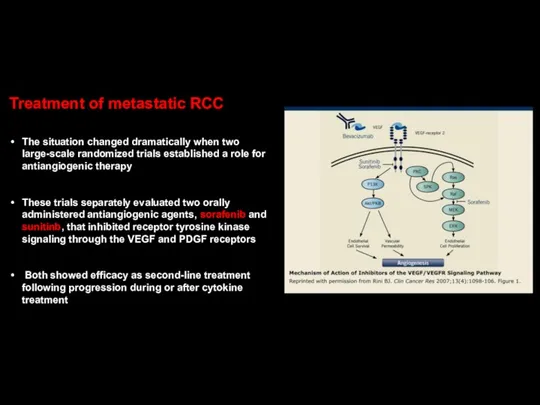
- 51. Treatment of metastatic RCC The situation changed dramatically when two large-scale randomized trials established a role
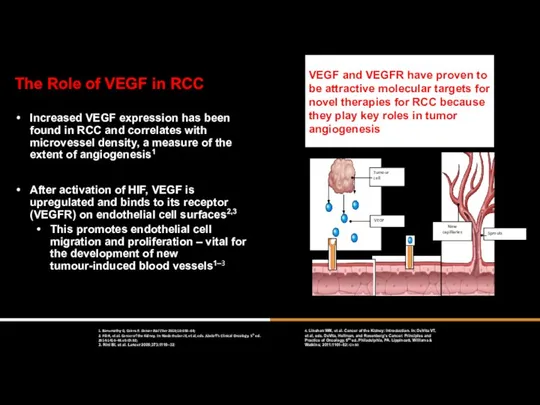
- 52. The Role of VEGF in RCC Increased VEGF expression has been found in RCC and correlates
- 54. A randomized phase III trial comparing sunitinib to interferon-α showed superior efficacy for sunitinib with an
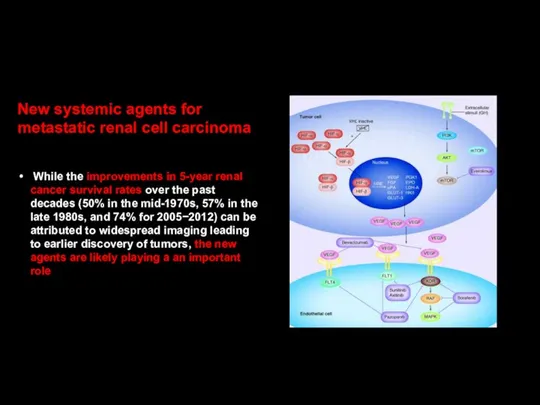
- 55. New systemic agents for metastatic renal cell carcinoma While the improvements in 5-year renal cancer survival
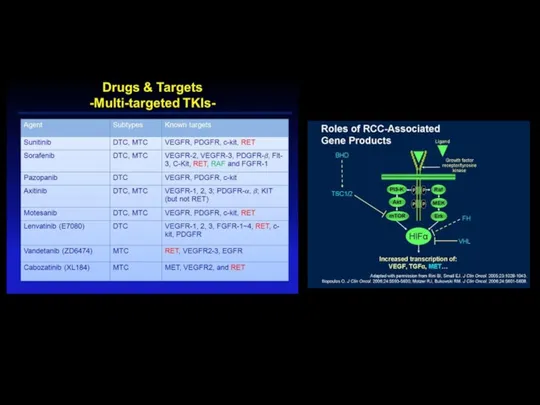
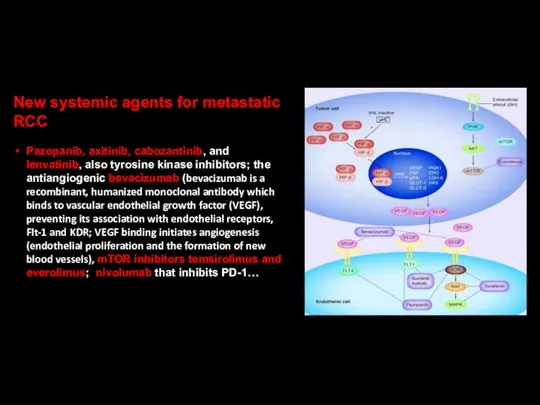
- 56. New systemic agents for metastatic RCC Pazopanib, axitinib, cabozantinib, and lenvatinib, also tyrosine kinase inhibitors; the
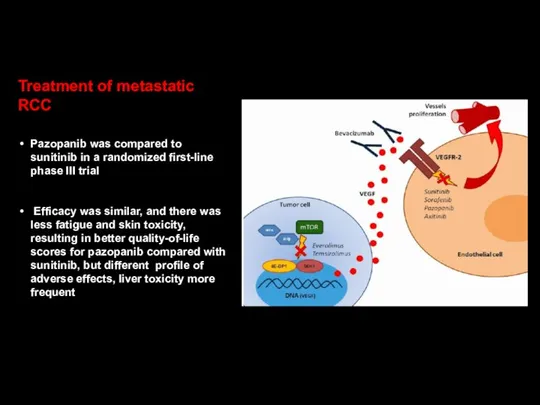
- 57. Treatment of metastatic RCC Pazopanib was compared to sunitinib in a randomized first-line phase III trial
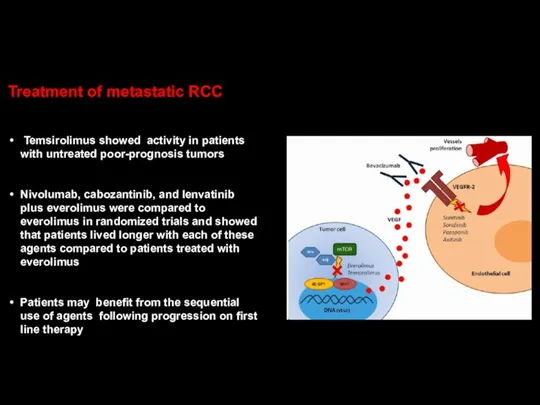
- 58. Treatment of metastatic RCC Temsirolimus showed activity in patients with untreated poor-prognosis tumors Nivolumab, cabozantinib, and
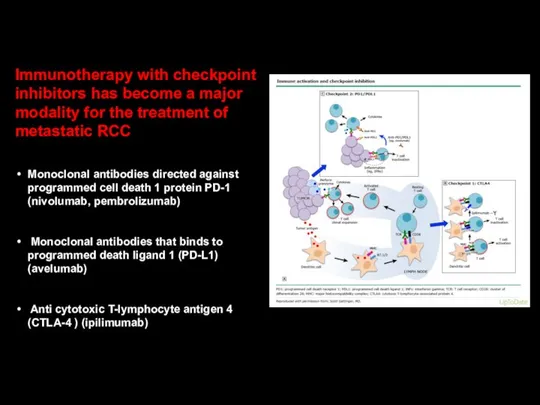
- 59. Immunotherapy with checkpoint inhibitors has become a major modality for the treatment of metastatic RCC Monoclonal
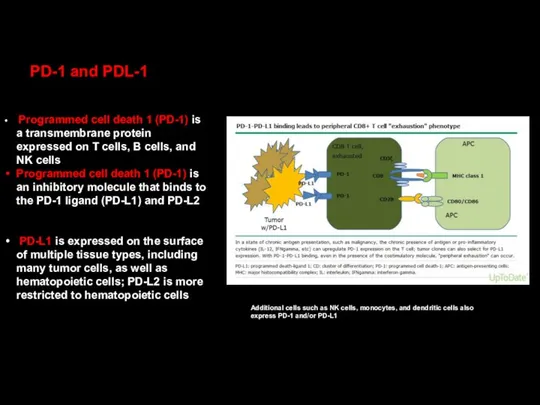
- 60. PD-1 and PDL-1 Programmed cell death 1 (PD-1) is a transmembrane protein expressed on T cells,
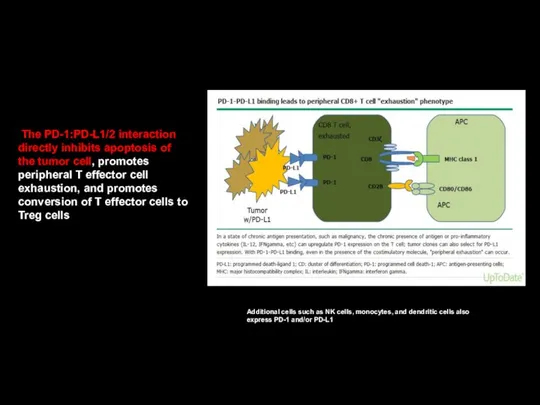
- 61. The PD-1:PD-L1/2 interaction directly inhibits apoptosis of the tumor cell, promotes peripheral T effector cell exhaustion,
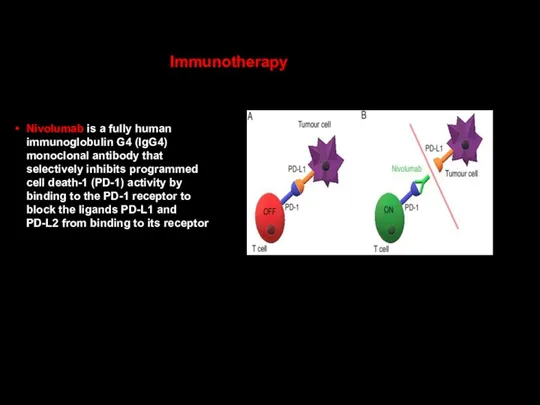
- 62. Nivolumab is a fully human immunoglobulin G4 (IgG4) monoclonal antibody that selectively inhibits programmed cell death-1
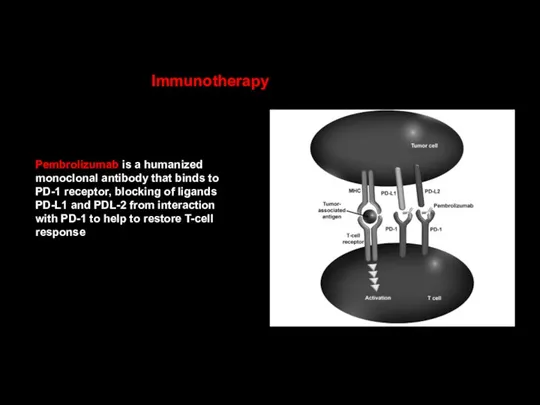
- 63. Pembrolizumab is a humanized monoclonal antibody that binds to PD-1 receptor, blocking of ligands PD-L1 and
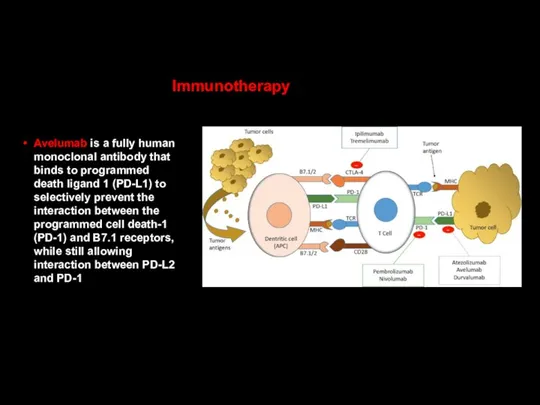
- 64. Avelumab is a fully human monoclonal antibody that binds to programmed death ligand 1 (PD-L1) to
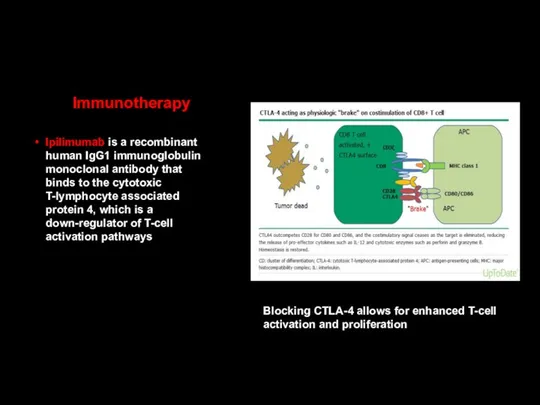
- 65. Immunotherapy Ipilimumab is a recombinant human IgG1 immunoglobulin monoclonal antibody that binds to the cytotoxic T-lymphocyte
- 66. Immunotherapy combinations Combining nivolumab (anti-PD-1) with ipilimumab (anti-CTLA-4) results in enhanced T-cell function, resulting in improved
- 67. Nivolumab+cabozantinib Pembrolizumab+lenvatinib Pembrolizumab+axitinib Avelumab+axitinib… Immunotherapy+ tyrosine kinase inhibitors Another effective combinations for treatment of metastatic RCC?
- 68. Patients with advanced or metastatic clear cell RCC are typically treated with systemic therapy as initial
- 70. Скачать презентацию
Epidemiology
Renal cell carcinomas (RCCs), which originate within the renal cortex, are
Renal cell carcinomas (RCCs), which originate within the renal cortex, are
Worldwide, in 2018, there were an estimated 403,000 new cases of
RCC is approximately twofold more common in men compared with women
RCC is approximately twofold more common in men compared with women
Some notable features of RCC include:
Common diagnosis of asymptomatic disease
Resistance
Common diagnosis of asymptomatic disease
Resistance
Survival
The incidence of RCC has risen threefold higher than the mortality
The incidence of RCC has risen threefold higher than the mortality
Risk factors associated with a increased incidence of RCC
Smoking
Hypertension
Obesity….
Otherwise, for patients
Smoking
Hypertension
Obesity….
Otherwise, for patients
Other risk factors associated with a increased incidence of RCC
Acquired cystic
Acquired cystic
Other risk factors associated with a increased incidence of RCC
Occupational exposure
Occupational exposure
Other risk factors associated with a increased incidence of RCC
Cytotoxic chemotherapy — The
Cytotoxic chemotherapy — The
Other risk factors associated with a increased incidence of RCC
Kidney stones---A
Kidney stones---A
Risk factors for RCC
The risk of a second, metachronous RCC is
Risk factors for RCC
The risk of a second, metachronous RCC is
Other factors that modify risk
Diabetes mellitus
Polycystic kidney disease
Alcohol (protective effect)?
Childhood
Other factors that modify risk
Diabetes mellitus
Polycystic kidney disease
Alcohol (protective effect)?
Childhood
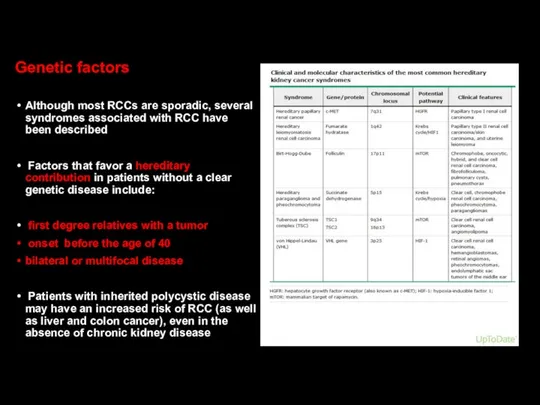
Genetic factors
Although most RCCs are sporadic, several syndromes associated with RCC
Genetic factors
Although most RCCs are sporadic, several syndromes associated with RCC
Von Hippel-Lindau (VHL) disease
Von Hippel-Lindau (VHL) syndrome is characterized by germline
Von Hippel-Lindau (VHL) syndrome is characterized by germline
Hemangioblastomas of CNS (cerebellum, brainstem, spinal cord)
Retinal hemangioblastomas
ccRCCs
Pheochromocytomas
Endolymphatic sac tumours of
Retinal hemangioblastomas
ccRCCs
Pheochromocytomas
Endolymphatic sac tumours of
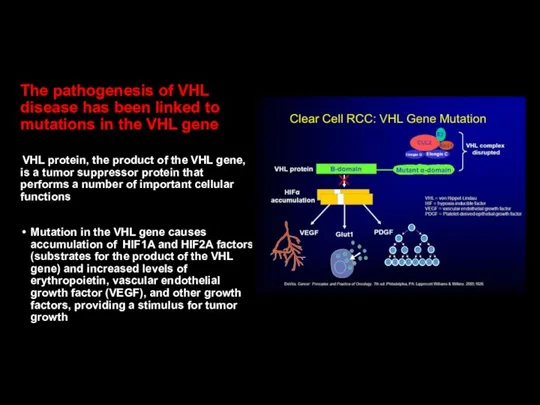
The pathogenesis of VHL disease has been linked to mutations in
Hereditary cancer kidney syndromes
Hereditary papillary renal carcinoma (HPRC) is a familial
Hereditary papillary renal carcinoma (HPRC) is a familial
Hereditary cancer kidney syndromes
Birt-Hogg-Dubé syndrome is a rare human autosomal dominant
Hereditary cancer kidney syndromes
Birt-Hogg-Dubé syndrome is a rare human autosomal dominant
Histological classification of RCC
Clear cell carcinoma (70% of cases)
Papillary tumors
Clear cell carcinoma (70% of cases)
Papillary tumors
Pathology RCC
Papillary tumors tend to be bilateral and multifocal
Chromophobe tumors have
Papillary tumors tend to be bilateral and multifocal
Chromophobe tumors have
Clear cell RCC
Clear cell tumors, the predominant histology, are found in
Clear cell tumors, the predominant histology, are found in
Clear cell RCC
VHL is the gene most frequently mutated in clear
VHL is the gene most frequently mutated in clear
Important!
Although these tumors have a clear clonal origin and often contain
Important!
Although these tumors have a clear clonal origin and often contain
While VHL is the gene most frequently mutated in clear cell
Papillary RCC type 1
Approximately 10% of RCC are of the papillary
Approximately 10% of RCC are of the papillary
Papillary RCC type 2
●Type 2 papillary RCC tumors may be characterized
●Type 2 papillary RCC tumors may be characterized
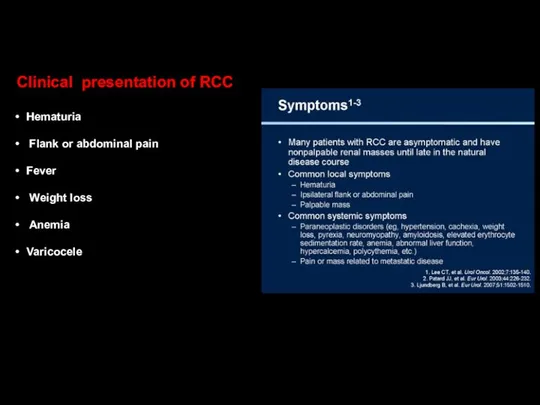
Clinical presentation of RCC
Hematuria
Flank or abdominal pain
Fever
Weight loss
Clinical presentation of RCC
Hematuria
Flank or abdominal pain
Fever
Weight loss
The classic triad of RCC (flank pain, hematuria, and a palpable
Scrotal varicocele, usually left sided, is observed in as many as
Kidney cancer was called the “internist’s tumor” since it was often
Kidney cancer was called the “internist’s tumor” since it was often
At present time RCC most commonly detected as an incidental finding
The standard evaluation of patients with renal mass
CT scan of the
CT scan of the
Any solid renal masses should be suspected malignant until proven otherwise
The
The
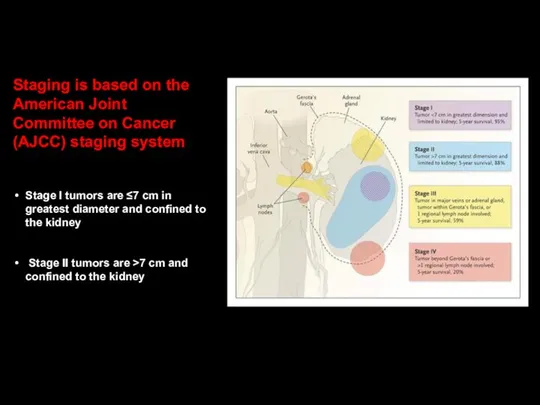
Staging is based on the American Joint Committee on Cancer (AJCC)
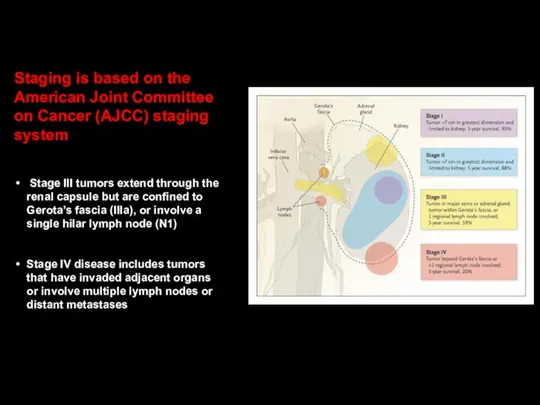
Staging is based on the American Joint Committee on Cancer (AJCC)

Staging and prognosis
65 % of patients present with stage I or
Staging and prognosis
65 % of patients present with stage I or
Staging and prognosis
The 5-year survival rate varies by stage
81% for stage
Staging and prognosis
The 5-year survival rate varies by stage
81% for stage
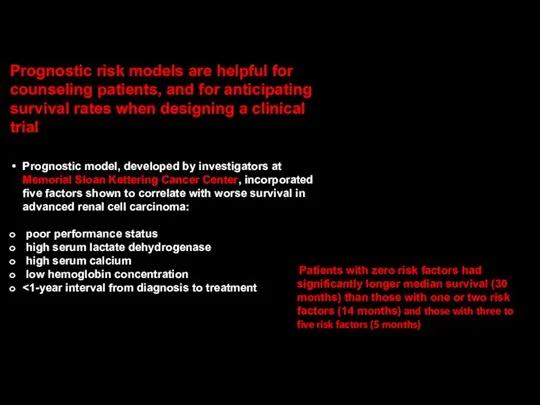
Prognostic risk models are helpful for counseling patients, and for anticipating
Prognostic risk models are helpful for counseling patients, and for anticipating
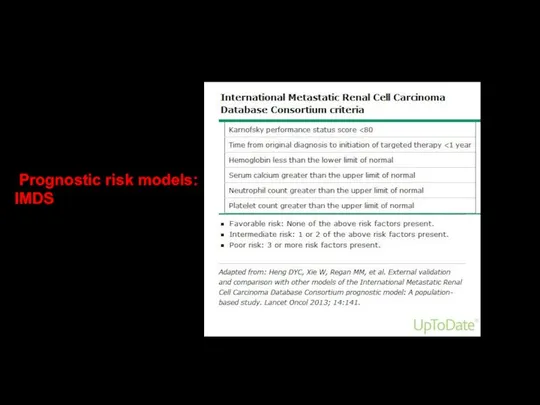
Prognostic risk models:
IMDS
IMDS
Treatment of localized RCC
The standard management for stage I or II
The standard management for stage I or II
Treatment of localized RCC
Extension into the renal vein or inferior vena
Extension into the renal vein or inferior vena
Nephron-sparing approaches via open or laparoscopic surgery may be appropriate for
Radical nephrectomy can lead to an increased risk for chronic
Radical nephrectomy can lead to an increased risk for chronic
Adjuvant therapy with interferon-α or radiation therapy following radical nephrectomy does
The most common sites of distant metastases are the lungs, lymph
The most common sites of distant metastases are the lungs, lymph
Surgery has a limited role for patients with metastatic disease
Long-term survival
Long-term survival
Radiation therapy is generally used for palliation of bone or brain
Metastatic renal cell carcinoma is refractory to cytotoxic chemotherapy
The fields of
The fields of
Removal of primary RCCs can evoke an immune response that occasionally
Treatment of metastatic RCC
The situation changed dramatically when two large-scale randomized
The situation changed dramatically when two large-scale randomized
The Role of VEGF in RCC
Increased VEGF expression has been found
The Role of VEGF in RCC
Increased VEGF expression has been found
A randomized phase III trial comparing sunitinib to interferon-α showed superior
New systemic agents for metastatic renal cell carcinoma
While the improvements in
While the improvements in
New systemic agents for metastatic RCC
Pazopanib, axitinib, cabozantinib, and lenvatinib, also
Pazopanib, axitinib, cabozantinib, and lenvatinib, also
Treatment of metastatic RCC
Pazopanib was compared to sunitinib in a randomized
Pazopanib was compared to sunitinib in a randomized
Treatment of metastatic RCC
Temsirolimus showed activity in patients with untreated poor-prognosis
Temsirolimus showed activity in patients with untreated poor-prognosis
Immunotherapy with checkpoint inhibitors has become a major modality for the
PD-1 and PDL-1
Programmed cell death 1 (PD-1) is a transmembrane
Programmed cell death 1 (PD-1) is a transmembrane
The PD-1:PD-L1/2 interaction directly inhibits apoptosis of the tumor cell,
The PD-1:PD-L1/2 interaction directly inhibits apoptosis of the tumor cell,
Nivolumab is a fully human immunoglobulin G4 (IgG4) monoclonal antibody
Nivolumab is a fully human immunoglobulin G4 (IgG4) monoclonal antibody
Pembrolizumab is a humanized monoclonal antibody that binds to PD-1 receptor,
Pembrolizumab is a humanized monoclonal antibody that binds to PD-1 receptor,
Avelumab is a fully human monoclonal antibody that binds to
Avelumab is a fully human monoclonal antibody that binds to
Immunotherapy
Ipilimumab is a recombinant human IgG1 immunoglobulin monoclonal antibody that binds
Ipilimumab is a recombinant human IgG1 immunoglobulin monoclonal antibody that binds
Immunotherapy combinations
Combining nivolumab (anti-PD-1) with ipilimumab (anti-CTLA-4) results in enhanced
Combining nivolumab (anti-PD-1) with ipilimumab (anti-CTLA-4) results in enhanced
Nivolumab+cabozantinib
Pembrolizumab+lenvatinib
Pembrolizumab+axitinib
Avelumab+axitinib…
Immunotherapy+
tyrosine kinase inhibitors
Another effective combinations for treatment of metastatic RCC?
Nivolumab+cabozantinib
Pembrolizumab+lenvatinib
Pembrolizumab+axitinib
Avelumab+axitinib…
Immunotherapy+
tyrosine kinase inhibitors
Another effective combinations for treatment of metastatic RCC?
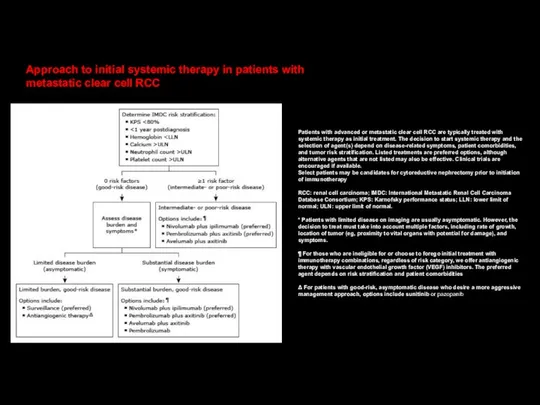
Patients with advanced or metastatic clear cell RCC are typically treated
Patients with advanced or metastatic clear cell RCC are typically treated
 Девиантное поведение. Устойчивое поведение личности, отклоняющееся от общепринятых, наиболее распространённых
Девиантное поведение. Устойчивое поведение личности, отклоняющееся от общепринятых, наиболее распространённых Современные методы исследования пищеварительного тракта
Современные методы исследования пищеварительного тракта Личная гигиена тяжелобольного пациента
Личная гигиена тяжелобольного пациента Цели и задачи ухода за больными детьми
Цели и задачи ухода за больными детьми Формирование и поддержание корпоративной культуры фармацевтической организации
Формирование и поддержание корпоративной культуры фармацевтической организации Костная онкология
Костная онкология Паренхиматозды мүшелердің жабық жарақаты
Паренхиматозды мүшелердің жабық жарақаты Гормондық заттардың жіктелуі. Гормондармен емдеудің принциптері. Гипо-, гипертиреозда қолданылатын препараттар
Гормондық заттардың жіктелуі. Гормондармен емдеудің принциптері. Гипо-, гипертиреозда қолданылатын препараттар Организация ухода за больными гастроэнтерологического профиля
Организация ухода за больными гастроэнтерологического профиля Консультирование бесплодной пары
Консультирование бесплодной пары Роль пожилого и старческого возраста в развитии патологии
Роль пожилого и старческого возраста в развитии патологии CAD/CAM система в ортопедической стоматологии
CAD/CAM система в ортопедической стоматологии Состав грудного молока
Состав грудного молока Проксемика – это пространственное расположение и ориентация партнеров по общению, дистанция между ними
Проксемика – это пространственное расположение и ориентация партнеров по общению, дистанция между ними Отёк Рейнке - причины, диагностика, подходы к лечению
Отёк Рейнке - причины, диагностика, подходы к лечению ИБС. Стенокардия. Инфаркт миокарда
ИБС. Стенокардия. Инфаркт миокарда Энурез. Эпидемиология
Энурез. Эпидемиология Основы рационального питания. Ожирение. Целлюлит
Основы рационального питания. Ожирение. Целлюлит ВМФ-дистанционный
ВМФ-дистанционный Клинико-иммунологические особенности пациентов с хроническим генерализованным пародонтитом
Клинико-иммунологические особенности пациентов с хроническим генерализованным пародонтитом Побочные действия. Антибиотики
Побочные действия. Антибиотики Дыхательная недостаточность
Дыхательная недостаточность Нефротический синдром
Нефротический синдром Диаскинтест. Методы ранней диагностики туберкулеза
Диаскинтест. Методы ранней диагностики туберкулеза Лекарства и беременность
Лекарства и беременность Патологическая анатомия отдельных врождённых пороков сердца
Патологическая анатомия отдельных врождённых пороков сердца Интубация трахеи. Виды, техника, осложнения. Алгоритм трудной интубации
Интубация трахеи. Виды, техника, осложнения. Алгоритм трудной интубации ОРВИ. Этиология, клинические проявления, диагностика. Тактика медицинского работника
ОРВИ. Этиология, клинические проявления, диагностика. Тактика медицинского работника