- VUR, UTI and antibiotic prophylaxis. How to use an article about therapy or prevention

Содержание
- 2. The Case Kali is a 14mo female who presents to WRAMC ED with fever to 102.
- 3. The Case Kali is a 14mo female who presents to WRAMC ED with fever to 102.
- 4. The Case Kali is a 14mo female who presents to WRAMC ED with fever to 102.
- 5. The Question Should we treat her prophylactically? Short-term: Will this decrease recurrent infections? Long-term: Will this
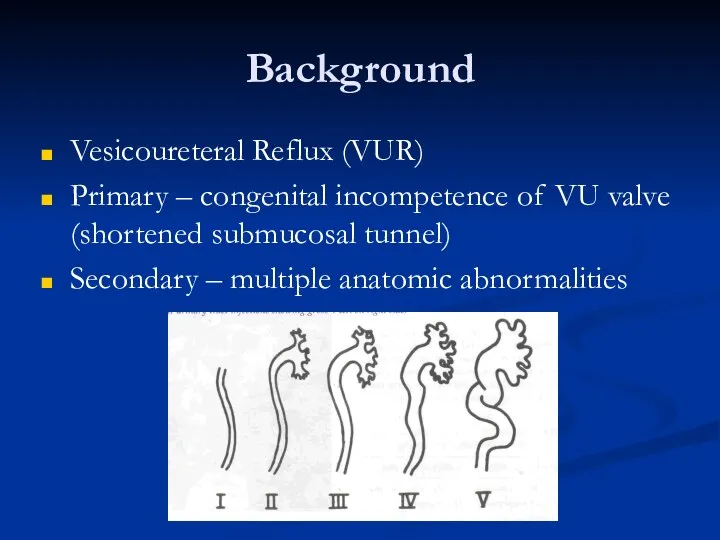
- 6. Background Vesicoureteral Reflux (VUR) Primary – congenital incompetence of VU valve (shortened submucosal tunnel) Secondary –
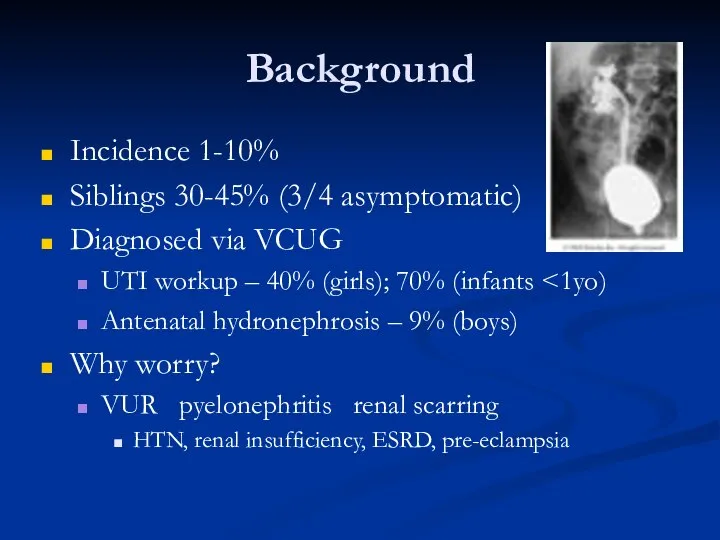
- 7. Background Incidence 1-10% Siblings 30-45% (3/4 asymptomatic) Diagnosed via VCUG UTI workup – 40% (girls); 70%
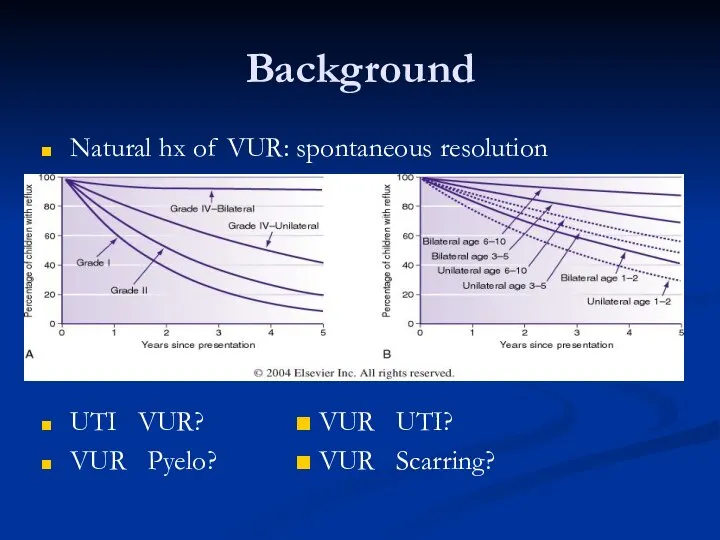
- 8. Background Natural hx of VUR: spontaneous resolution UTI ? VUR? ■ VUR ? UTI? VUR ?
- 9. Current Treatment Recs Workup: Febrile UTI (any age) UTI UTI x2 in school-age girls UTI in
- 10. AUA Treatment Guidelines
- 11. Current Treatment Recs AUA Pediatric VUR Guidelines Panel (1997) “The panel recommendations to offer continuous abx
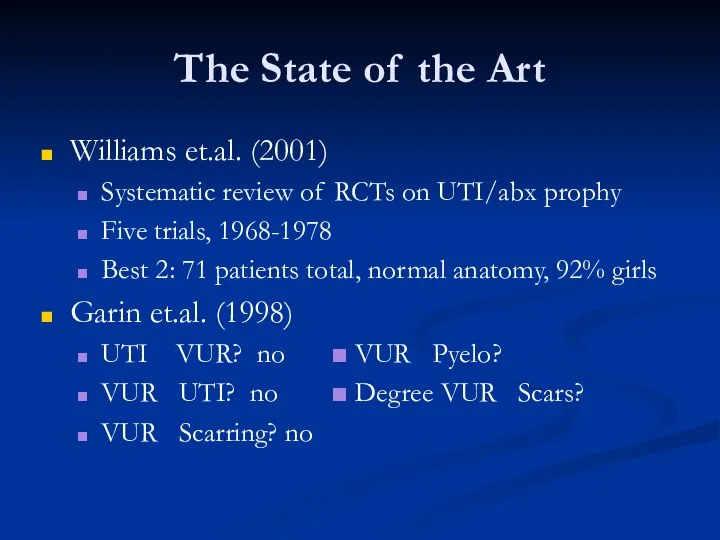
- 12. The State of the Art Williams et.al. (2001) Systematic review of RCTs on UTI/abx prophy Five
- 13. We Need A Study That… Will help us decide whether or not to prophylax this patient
- 14. Clinical significance of primary vesicoureteral reflux and urinary antibiotic prophylaxis after acute pyelonephritis: a multicenter, randomized,
- 15. Study Questions Does VUR correlate with ?UTI/renal scarring? Does antibiotic prophylaxis correlate with ?UTI/renal scarring?
- 16. Study Design Randomized, controlled, multicenter trial Inclusion: 3mo-18yo Acute pyelonephritis Exclusion: Grade IV-V VUR Anatomic abnormalities
- 17. Study Design Met inclusion criteria ? VCUG Pyelo treated: IV abx ? po for 14-day course
- 18. Follow Up At entry: UA/UCx, DMSA, VCUG, Renal US At Q3mo clinic visit: UA/UCx At 6mo:
- 19. Study Results
- 20. Analysis of Results Fisher’s Exact Test 2x2 comparison tables Control vs. variable Smaller sample size Gives
- 21. Study Results Recurrence of UTIs Timing Type Recurrent Pyelonephritis & Antibiotics Recurrent Pyelonephritis & VUR Degree
- 22. Study Results Recurrence of UTI Overall – 20.1% VUR not significant No abx (p=.9999) VUR –
- 23. Study Results Recurrent Pyelo and Antibiotics No benefit of abx (p=.0291) 7:1 abx:none Recurrent Pyelo and
- 24. Study Results Renal Scarring No evidence VUR? increased scarring (p=.9999) VUR (6.2%) = No VUR (5.7%)
- 25. Study Conclusions Mild/moderate VUR not associated with ?UTI, pyelonephritis, or scarring Antibiotic prophylaxis not associated with
- 26. Critically Evaluating… (JAMA Users’ Guide) Are the results valid? What were the results? Will the results
- 27. Are the results valid? Primary Guides Was the assignment of patients to treatment randomized? YES. Were
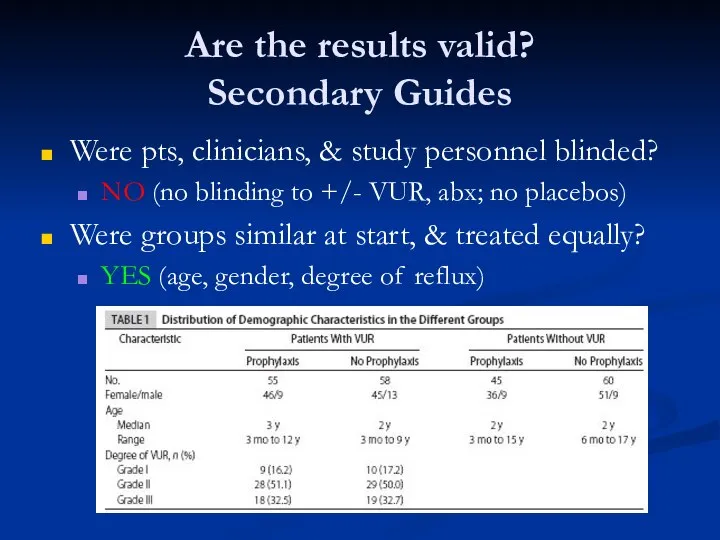
- 28. Are the results valid? Secondary Guides Were pts, clinicians, & study personnel blinded? NO (no blinding
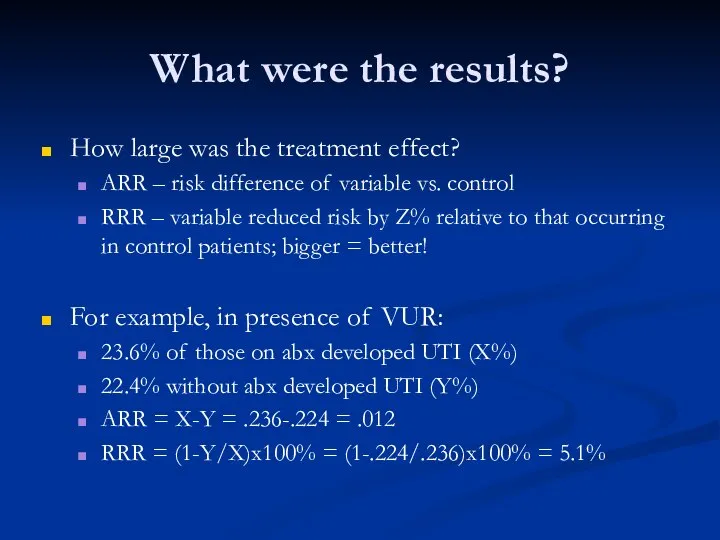
- 29. What were the results? How large was the treatment effect? ARR – risk difference of variable
- 30. What were the results? How large was the treatment effect? ARR/RRR not reported! How precise was
- 31. What were the results? POWER! Ability of a study to detect a true difference Directly related
- 32. Will the results help me take care of my patient? Can the results be applied? YES.
- 33. Criticisms: Study Population What about Present earlier = Higher-grade reflux? Already abx? Included in study? Exclusion
- 34. Criticisms: Study Design DMSA as inclusion criteria (multicenter)? Account for 18 lost before study end? Unknown
- 35. Criticisms: Data Analysis Reporting of CIs, ARR/RRR? Magnitude/precision of treatment effect Rule in/out effect different from
- 36. Further Questions… UTI prophylaxis vs. intermittent therapy? And risk of renal scarring Over time, given resolution
- 37. Back to our patient… What would you do? Call Dr.Cartwright and Dr.Lechner and get those patients
- 38. References Atala A, Keating MA. Vesicoureteral reflux and megaureter. In Campbell’s Urology Vol 2, 7th ed.
- 40. Скачать презентацию

The Case
Kali is a 14mo female who presents to WRAMC ED
The Case
Kali is a 14mo female who presents to WRAMC ED
The Case
Kali is a 14mo female who presents to WRAMC ED
The Case
Kali is a 14mo female who presents to WRAMC ED
The Case
Kali is a 14mo female who presents to WRAMC ED
The Case
Kali is a 14mo female who presents to WRAMC ED

The Question
Should we treat her prophylactically?
Short-term:
Will this decrease recurrent infections?
Long-term:
Will this
The Question
Should we treat her prophylactically?
Short-term:
Will this decrease recurrent infections?
Long-term:
Will this
Background
Vesicoureteral Reflux (VUR)
Primary – congenital incompetence of VU valve (shortened submucosal
Background
Vesicoureteral Reflux (VUR)
Primary – congenital incompetence of VU valve (shortened submucosal
Background
Incidence 1-10%
Siblings 30-45% (3/4 asymptomatic)
Diagnosed via VCUG
UTI workup – 40%
Background
Incidence 1-10%
Siblings 30-45% (3/4 asymptomatic)
Diagnosed via VCUG
UTI workup – 40%
Background
Natural hx of VUR: spontaneous resolution
UTI ? VUR? ■ VUR ?
Background
Natural hx of VUR: spontaneous resolution
UTI ? VUR? ■ VUR ?

Current Treatment Recs
Workup:
Febrile UTI (any age)
UTI <5yo
UTI x2 in school-age girls
UTI
Current Treatment Recs
Workup:
Febrile UTI (any age)
UTI <5yo
UTI x2 in school-age girls
UTI
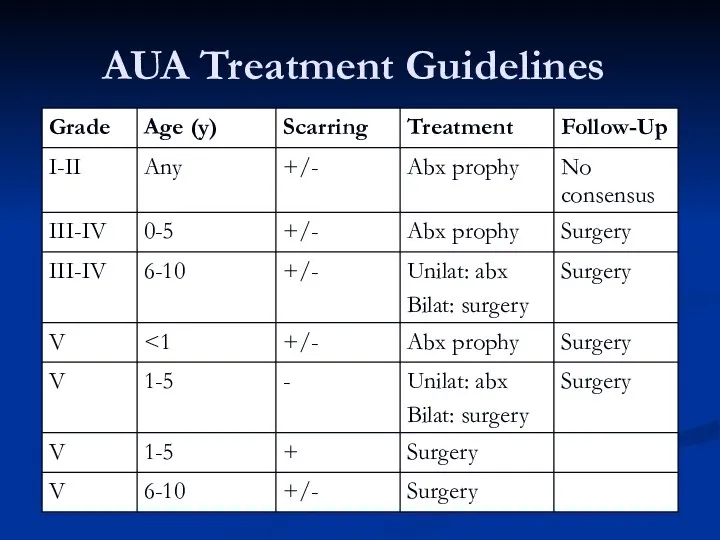
AUA Treatment Guidelines
AUA Treatment Guidelines
Current Treatment Recs
AUA Pediatric VUR Guidelines Panel (1997)
“The panel recommendations to
Current Treatment Recs
AUA Pediatric VUR Guidelines Panel (1997)
“The panel recommendations to
The State of the Art
Williams et.al. (2001)
Systematic review of RCTs on
The State of the Art
Williams et.al. (2001)
Systematic review of RCTs on

We Need A Study That…
Will help us decide whether or not
We Need A Study That…
Will help us decide whether or not
Clinical significance of primary vesicoureteral reflux and urinary antibiotic prophylaxis after
Clinical significance of primary vesicoureteral reflux and urinary antibiotic prophylaxis after
Study Questions
Does VUR correlate with ?UTI/renal scarring?
Does antibiotic prophylaxis correlate with
Study Questions
Does VUR correlate with ?UTI/renal scarring?
Does antibiotic prophylaxis correlate with
Study Design
Randomized, controlled, multicenter trial
Inclusion:
3mo-18yo
Acute pyelonephritis
Exclusion:
Grade IV-V VUR
Anatomic abnormalities
Pregnancy
Study Design
Randomized, controlled, multicenter trial
Inclusion:
3mo-18yo
Acute pyelonephritis
Exclusion:
Grade IV-V VUR
Anatomic abnormalities
Pregnancy
Study Design
Met inclusion criteria ? VCUG
Pyelo treated: IV abx ? po
Study Design
Met inclusion criteria ? VCUG
Pyelo treated: IV abx ? po
Follow Up
At entry: UA/UCx, DMSA, VCUG, Renal US
At Q3mo clinic visit:
Follow Up
At entry: UA/UCx, DMSA, VCUG, Renal US
At Q3mo clinic visit:
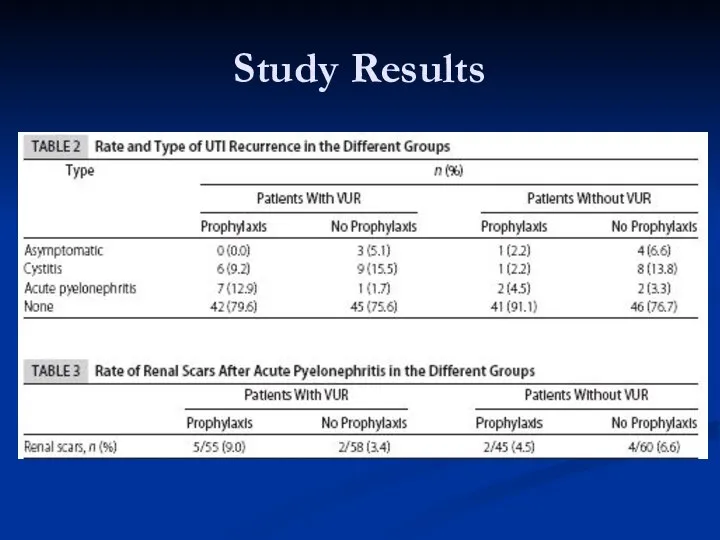
Study Results
Study Results

Analysis of Results
Fisher’s Exact Test
2x2 comparison tables
Control vs. variable
Smaller sample size
Gives
Analysis of Results
Fisher’s Exact Test
2x2 comparison tables
Control vs. variable
Smaller sample size
Gives
Study Results
Recurrence of UTIs
Timing
Type
Recurrent Pyelonephritis & Antibiotics
Recurrent Pyelonephritis & VUR Degree
Renal
Study Results
Recurrence of UTIs
Timing
Type
Recurrent Pyelonephritis & Antibiotics
Recurrent Pyelonephritis & VUR Degree
Renal

Study Results
Recurrence of UTI
Overall – 20.1%
VUR not significant
No abx (p=.9999)
VUR –
Study Results
Recurrence of UTI
Overall – 20.1%
VUR not significant
No abx (p=.9999)
VUR –
Study Results
Recurrent Pyelo and Antibiotics
No benefit of abx (p=.0291)
7:1 abx:none
Recurrent Pyelo
Study Results
Recurrent Pyelo and Antibiotics
No benefit of abx (p=.0291)
7:1 abx:none
Recurrent Pyelo

Study Results
Renal Scarring
No evidence VUR? increased scarring (p=.9999)
VUR (6.2%) = No
Study Results
Renal Scarring
No evidence VUR? increased scarring (p=.9999)
VUR (6.2%) = No
Study Conclusions
Mild/moderate VUR not associated with ?UTI, pyelonephritis, or scarring
Antibiotic prophylaxis
Study Conclusions
Mild/moderate VUR not associated with ?UTI, pyelonephritis, or scarring
Antibiotic prophylaxis

Critically Evaluating…
(JAMA Users’ Guide)
Are the results valid?
What were the results?
Will the
Critically Evaluating…
(JAMA Users’ Guide)
Are the results valid?
What were the results?
Will the
Are the results valid?
Primary Guides
Was the assignment of patients to treatment
Are the results valid?
Primary Guides
Was the assignment of patients to treatment
Are the results valid?
Secondary Guides
Were pts, clinicians, & study personnel blinded?
NO
Are the results valid?
Secondary Guides
Were pts, clinicians, & study personnel blinded?
NO
What were the results?
How large was the treatment effect?
ARR – risk
What were the results?
How large was the treatment effect?
ARR – risk
What were the results?
How large was the treatment effect?
ARR/RRR not reported!
How
What were the results?
How large was the treatment effect?
ARR/RRR not reported!
How
What were the results?
POWER!
Ability of a study to detect a true
What were the results?
POWER!
Ability of a study to detect a true

Will the results help me take care of my patient?
Can the
Will the results help me take care of my patient?
Can the
Criticisms:
Study Population
What about <3mo?
Present earlier = Higher-grade reflux? Already abx?
Included
Criticisms:
Study Population
What about <3mo?
Present earlier = Higher-grade reflux? Already abx?
Included
Criticisms:
Study Design
DMSA as inclusion criteria (multicenter)?
Account for 18 lost before study
Criticisms:
Study Design
DMSA as inclusion criteria (multicenter)?
Account for 18 lost before study
Criticisms:
Data Analysis
Reporting of CIs, ARR/RRR?
Magnitude/precision of treatment effect
Rule in/out effect different
Criticisms:
Data Analysis
Reporting of CIs, ARR/RRR?
Magnitude/precision of treatment effect
Rule in/out effect different

Further Questions…
UTI prophylaxis vs. intermittent therapy?
And risk of renal scarring
Over time,
Further Questions…
UTI prophylaxis vs. intermittent therapy?
And risk of renal scarring
Over time,
Back to our patient…
What would you do?
Call Dr.Cartwright and Dr.Lechner and
Back to our patient…
What would you do?
Call Dr.Cartwright and Dr.Lechner and

References
Atala A, Keating MA. Vesicoureteral reflux and megaureter. In Campbell’s Urology
References
Atala A, Keating MA. Vesicoureteral reflux and megaureter. In Campbell’s Urology
 Спленэктомия. Техникасы
Спленэктомия. Техникасы Танымдық психикалық процестер: түйсік, қабылдау
Танымдық психикалық процестер: түйсік, қабылдау Рак яичника
Рак яичника Сбор и сушка растительного сырья. Оформление гербария. Тема 1.9
Сбор и сушка растительного сырья. Оформление гербария. Тема 1.9 Вегетативная нервная система. Методы обследования в неврологии. (Занятие 8)
Вегетативная нервная система. Методы обследования в неврологии. (Занятие 8) Диагностика и лечение варикозной болезни вен нижних конечностей
Диагностика и лечение варикозной болезни вен нижних конечностей Анатомо-физиологические особенности строения полости рта в возрастном аспекте
Анатомо-физиологические особенности строения полости рта в возрастном аспекте Беременность и ВПЧ-инфекция
Беременность и ВПЧ-инфекция Чувства, эмоции
Чувства, эмоции Проект Бережливая поликлиника
Проект Бережливая поликлиника Ведение беременности и родов при туберкулёзе
Ведение беременности и родов при туберкулёзе Изучение причин возникновения и профилактика пищевых отравлений и инфекционных заболеваний
Изучение причин возникновения и профилактика пищевых отравлений и инфекционных заболеваний Массовые истерии
Массовые истерии Систематические обзоры и мета-анализ статей
Систематические обзоры и мета-анализ статей Первичные бактериальные менингиты. Диагностика и лечение
Первичные бактериальные менингиты. Диагностика и лечение Пухлини органів травлення
Пухлини органів травлення Научно-исследовательская работа: Шумовые загрязнения влияющие на здоровье человека.
Научно-исследовательская работа: Шумовые загрязнения влияющие на здоровье человека. Резиденттің өзіндік жұмысы
Резиденттің өзіндік жұмысы Основы эргономики и безопасности перемещения пациента
Основы эргономики и безопасности перемещения пациента Массаж. Илеу
Массаж. Илеу Basic life support
Basic life support Міопатії. Невральні аміотрофії. Міотонія Томпсона
Міопатії. Невральні аміотрофії. Міотонія Томпсона Общая рецептура твердые и мягкие лекарственные формы/ /жидкие лекарственные формы
Общая рецептура твердые и мягкие лекарственные формы/ /жидкие лекарственные формы Морфологические и физиологические особенности плода в разные периоды внутриутробного развития
Морфологические и физиологические особенности плода в разные периоды внутриутробного развития Внимание и воля
Внимание и воля Медицина эпохи Возрождения
Медицина эпохи Возрождения Лекарственные растения и лекарственное сырье, применяемое при лечении и профилактики атеросклероза
Лекарственные растения и лекарственное сырье, применяемое при лечении и профилактики атеросклероза Аллергия - проблема XXI века
Аллергия - проблема XXI века