- Аутоиммунные заболевания ЦНС

Содержание
- 2. Первую группу составляют заболевания, развивающиеся в результате нарушения сосудисто-тканевых барьеров и высвобождения антигенов из физиологических тканей
- 3. Аутоиммунные заболевания нервной системы. В 2000 г. D. Karussis предложил классификацию аутоиммунных заболеваний нервной системы, согласно
- 4. Аутоиммунные заболевания нервной системы. (продолжение) В группу системных аутоиммунных заболеваний с вторичным поражением нервной системы входят:
- 5. РАССЕЯННЫЙ СКЛЕРОЗ
- 7. The glioneuronal micromilieu regulates immunological mechanisms within the brain. The upper panel illustrates the physiologic situation
- 8. Рассе́янный склеро́з (РС) — хроническое аутоиммунное заболевание— хроническое аутоиммунное заболевание, при котором поражается миелиновая оболочка нервных
- 9. Возникновение рассеянного склероза связано со случайным индивидуальным сочетанием неблагоприятных эндогенных и экзогенных факторов риска. К эндогенным
- 10. В результате многочисленных исследований было установлено, что для рассеянного склероза существуют так называемые «гены рассеянного склероза»,
- 13. Активированные лимфоциты способны проникать через ГЭБ. Проникшие в мозг активированные CD4+ Т-клетки способны вызывать нейротоксический эффект
- 14. B-Cell functions in autoimmunity: Antibody-producing cells–plasma cells. (b) Antigen-presenting cells (autoreactive T cells with a specific
- 15. The immunopathogenesis of MS A limited number of resting T cells may enter the CNS after
- 16. Models of demyelination in multiple sclerosis. Primary autoimmune attack. Autoreactive Th lymphocytes initiate the autoimmune attack
- 17. Alternative views of the mechanisms of lesion formation in MS. (a) Activated T cells migrate into
- 18. Role of complement activation in the pathogenesis of multiple sclerosis. The immune response is initiated in
- 19. Классическими клиническими критериями диагностики рассеянного склероза являются клинические диагностические критерии достоверного рассеянного склероза (G. Schumacher и
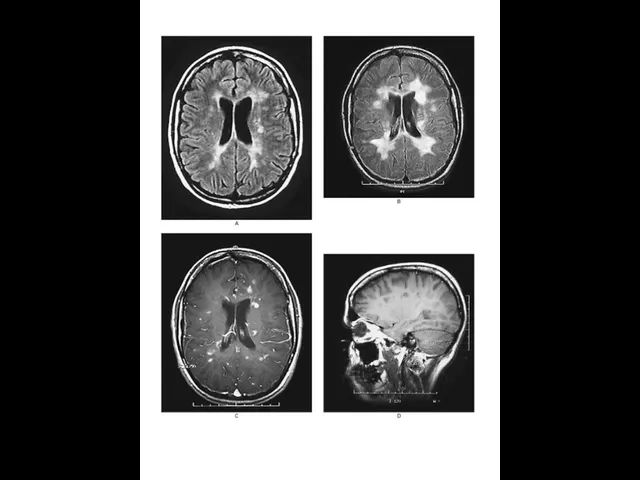
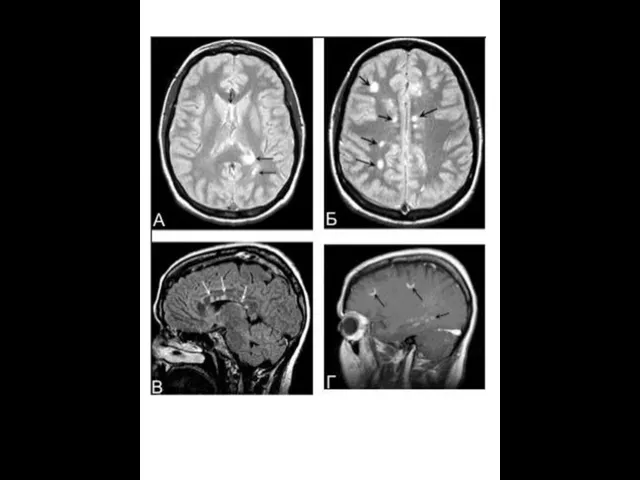
- 20. МРТ в диагностике рассеянного склероза МРТ — метод диагностики, основанный на том, что из-за особенностей белково-липидного
- 21. MRI –Т1 ( left ), MWF – Т2 (middle ) and Luxol fast blue myelin stain
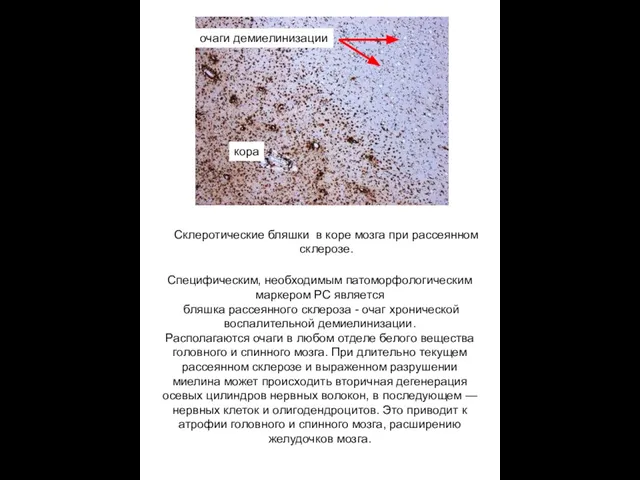
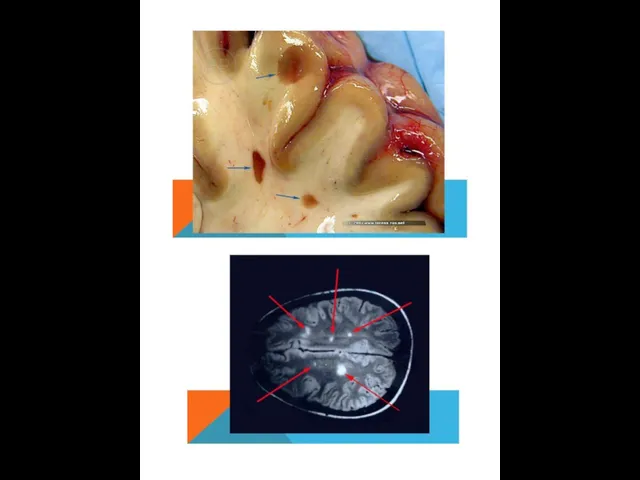
- 24. Склеротические бляшки в коре мозга при рассеянном склерозе. кора Специфическим, необходимым патоморфологическим маркером РС является бляшка
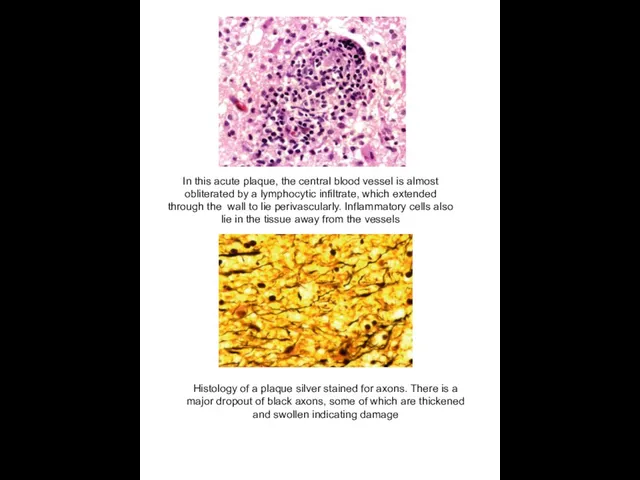
- 25. In this acute plaque, the central blood vessel is almost obliterated by a lymphocytic infiltrate, which
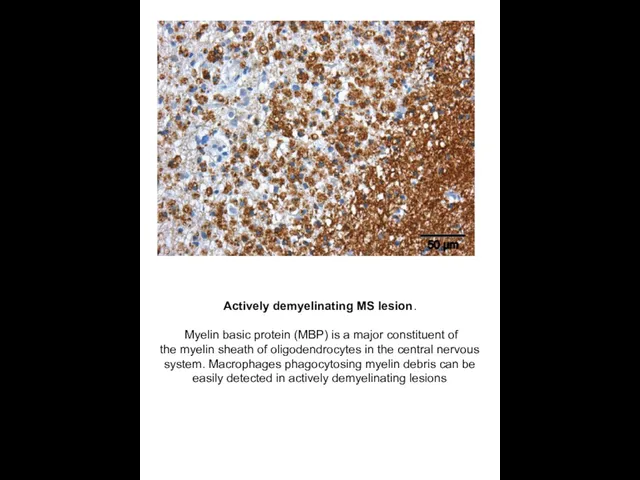
- 26. Actively demyelinating MS lesion. Myelin basic protein (MBP) is a major constituent of the myelin sheath
- 27. Table I. Variable Elements Identified in MS Plaquesa Cellular T cells (CD41, CD81, TcRa/b, and TcR
- 28. MRI from a normal subject (left), a patient with RRMS (middle) and a patient with SPMS
- 30. Electron micrograph showing a field of demyelinated axons. On the right, two remyelinated axons, with thin
- 31. Разрушение нерва цитотоксическими Т-лимфоцитами
- 32. Axons are transected during inflammatory demyelination. Confocal image of an actively demyelinating MS lesion stained for
- 33. Cortical demyelination and neuronal pathology. Three types of cortical lesions have been described in MS brains
- 34. Spinal cord demyelination. The spinal cord is a predilection site for MS lesions, and inmany advanced
- 35. Рассеянный склероз: роковая ошибка иммунной системы Причиной рассеянного склероза, вероятно, является широко распространенный вирус, ранее считавшийся
- 36. SUMMARY POINTS Multiple sclerosis is an immune-mediated demyelinating disease of the human central nervous system. 2.
- 37. Рассеянный склероз: иммунные клетки нервной системы (жёлтые) нападают на олигодендроциты,
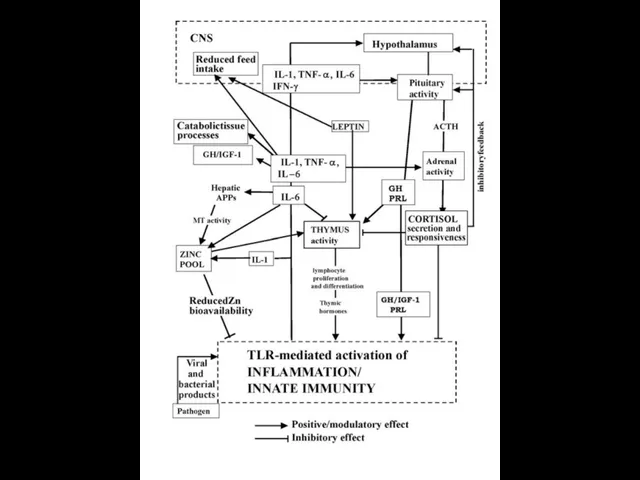
- 38. Network including most of the components of the inflammatory response. Initiating factors of inflammation are represented
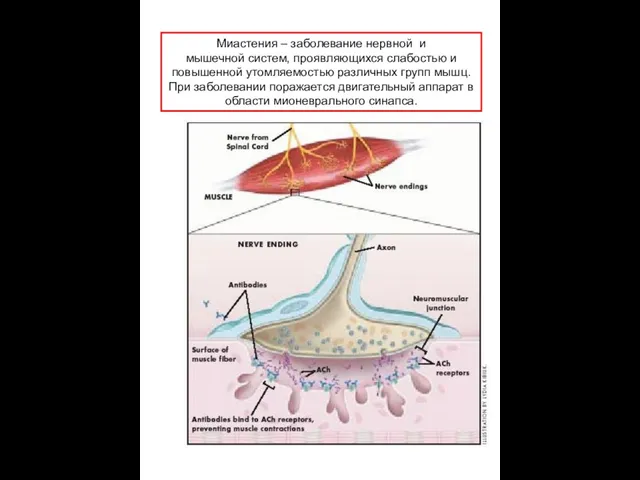
- 41. Миастения – заболевание нервной и мышечной систем, проявляющихся слабостью и повышенной утомляемостью различных групп мышц. При
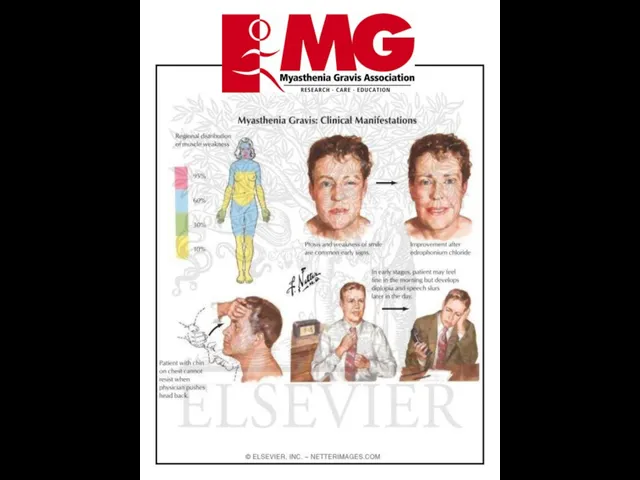
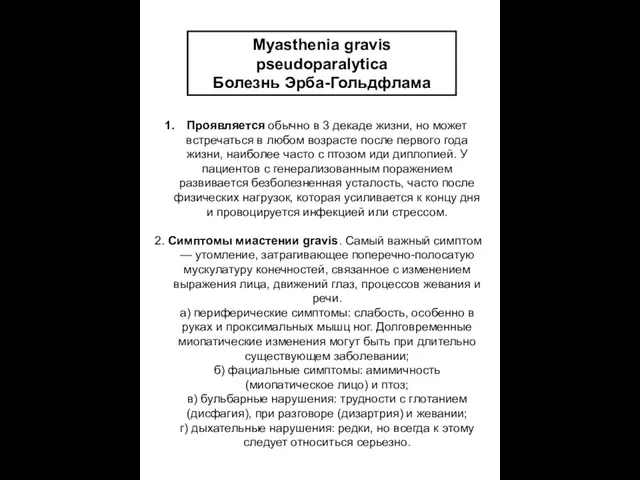
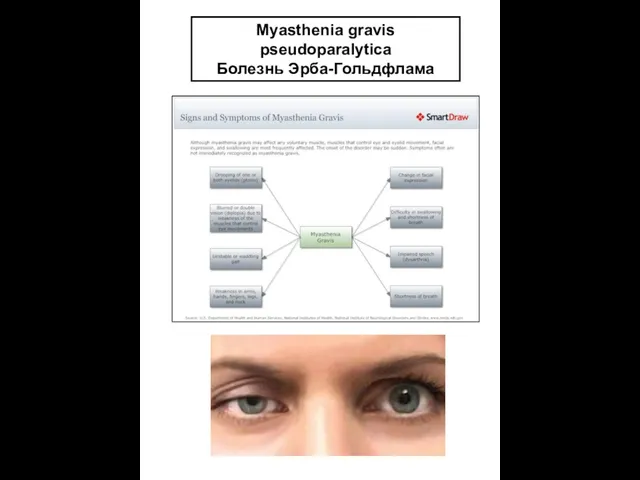
- 42. Myasthenia gravis pseudoparalytica Болезнь Эрба-Гольдфлама Проявляется обычно в 3 декаде жизни, но может встречаться в любом
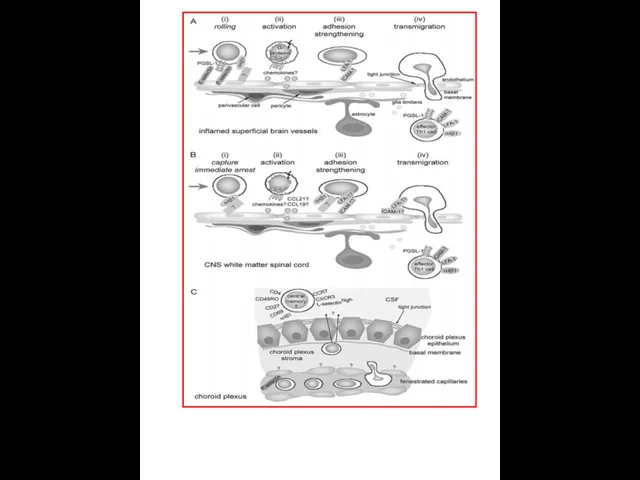
- 43. Cellular and molecular players in the multi-step recruitment of T lymphocytes across the blood-CNS barriers. A
- 44. Myasthenia gravis pseudoparalytica Болезнь Эрба-Гольдфлама
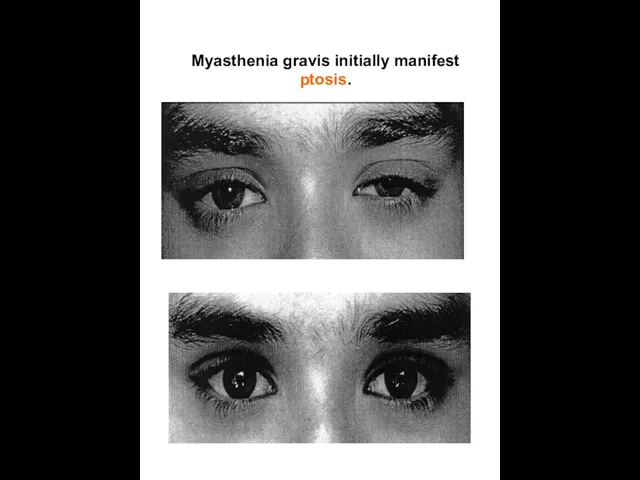
- 45. Myasthenia gravis initially manifest ptosis.
- 46. Патология является результатом выработки антител против альфа-субединицы никотиновых холинорецепторов. Антитела к никотиновым рецепторам подобно кураре затрудняют
- 47. Направления виды лечения миастении 1 — антихолинестеразная терапия, 2 — иммуносупрессивная терапия (глюкокортикостероидная и цитостатическая), 3
- 52. Chronically demyelinated axons degenerate owing to loss of myelin trophic support. A continuous and irreversible loss
- 53. A model of MS immunopathogenesis. Myelin-autoreactive T cells are found in an enhanced state of activation
- 54. Functions of microglia in immune and inflammatory mechanisms in the CNS. Microglia produce a variety of
- 55. Chronology of a newly forming lesion in the relapsing and remitting form of MS. Early pathological
- 56. Pathogenesis of EAE. In the peripheral immune system, antigen‐presenting cells (mainly DCs but also B cells
- 57. The role of lymphoid chemokines in CNS homeostatic and pathogenic states. А. CCL19 and CCL21 are
- 58. Photograph of a brain with well-demarcated gray/pink MS plaques around the ventricles and extending into the
- 59. Neurodegeneration and Neuroprotection – Innate Immune Response. Figure 1 Innate (natural) defensemechanisms in health and diseases
- 61. Use of EAE in neuroimmunology research. Healthy mice are immunized with a subcutaneous injection of strainspecific,
- 62. Schematic drawing representing signal transduction of interleukin-1 and tumor necrosis factor. AA: arachidonic acid; AC: adenylate
- 63. Development of central nervous system inflammation and damage. After antigen recognition by T cells, several cytokines
- 66. Скачать презентацию
Первую группу составляют заболевания, развивающиеся в результате нарушения сосудисто-тканевых барьеров и высвобождения антигенов
Первую группу составляют заболевания, развивающиеся в результате нарушения сосудисто-тканевых барьеров и высвобождения антигенов
Аутоиммунные заболевания нервной системы.
В 2000 г. D. Karussis предложил классификацию аутоиммунных
Аутоиммунные заболевания нервной системы.
В 2000 г. D. Karussis предложил классификацию аутоиммунных
Аутоиммунные заболевания нервной системы.
(продолжение)
В группу системных аутоиммунных заболеваний с
Аутоиммунные заболевания нервной системы.
(продолжение)
В группу системных аутоиммунных заболеваний с
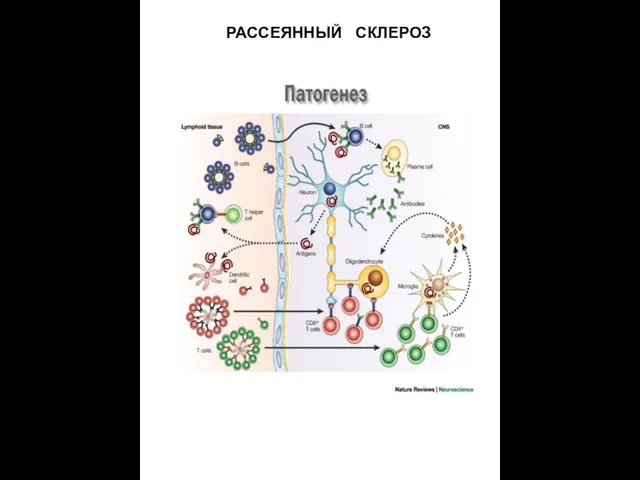
РАССЕЯННЫЙ СКЛЕРОЗ
РАССЕЯННЫЙ СКЛЕРОЗ
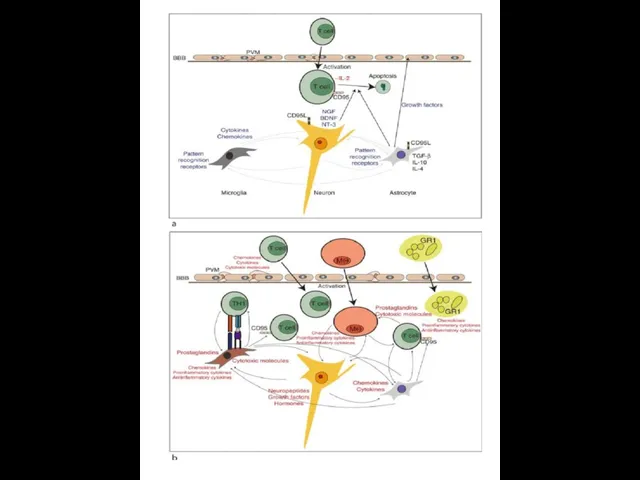
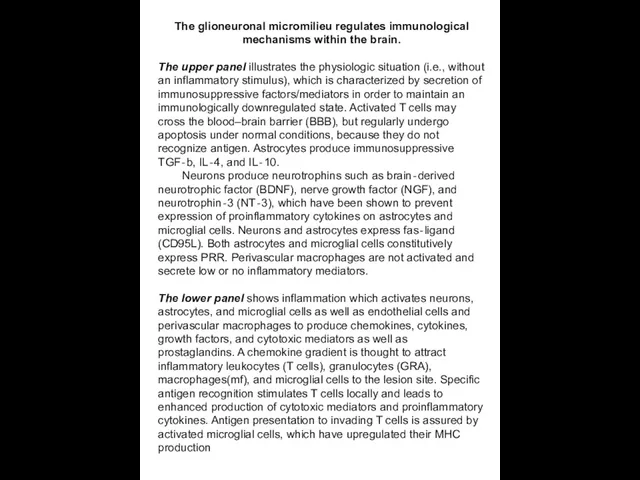
The glioneuronal micromilieu regulates immunological mechanisms within the brain.
The upper
The glioneuronal micromilieu regulates immunological mechanisms within the brain.
The upper
Рассе́янный склеро́з (РС)
— хроническое аутоиммунное заболевание— хроническое аутоиммунное заболевание, при котором
Рассе́янный склеро́з (РС)
— хроническое аутоиммунное заболевание— хроническое аутоиммунное заболевание, при котором
Возникновение рассеянного склероза связано со случайным индивидуальным сочетанием неблагоприятных эндогенных и
Возникновение рассеянного склероза связано со случайным индивидуальным сочетанием неблагоприятных эндогенных и
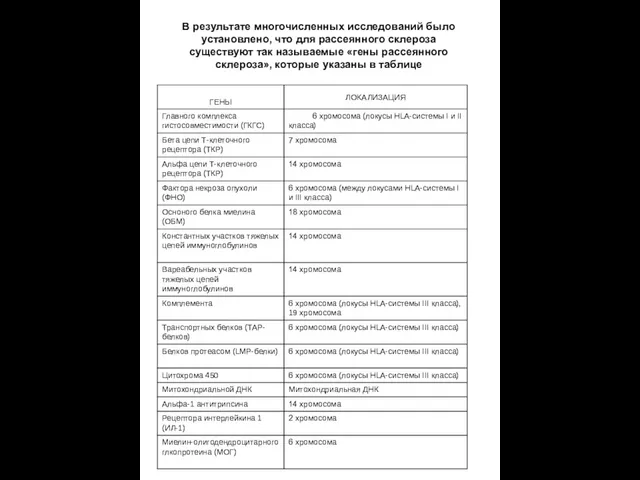
В результате многочисленных исследований было установлено, что для рассеянного склероза существуют
В результате многочисленных исследований было установлено, что для рассеянного склероза существуют

Активированные лимфоциты способны проникать через ГЭБ. Проникшие в мозг активированные CD4+
Активированные лимфоциты способны проникать через ГЭБ. Проникшие в мозг активированные CD4+
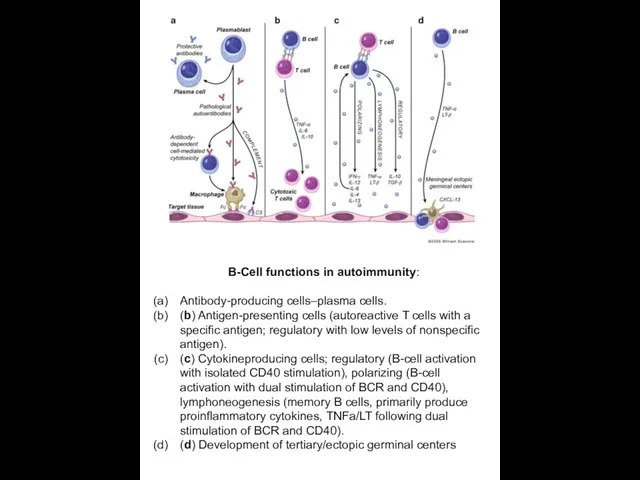
B-Cell functions in autoimmunity:
Antibody-producing cells–plasma cells.
(b) Antigen-presenting cells (autoreactive
B-Cell functions in autoimmunity:
Antibody-producing cells–plasma cells.
(b) Antigen-presenting cells (autoreactive
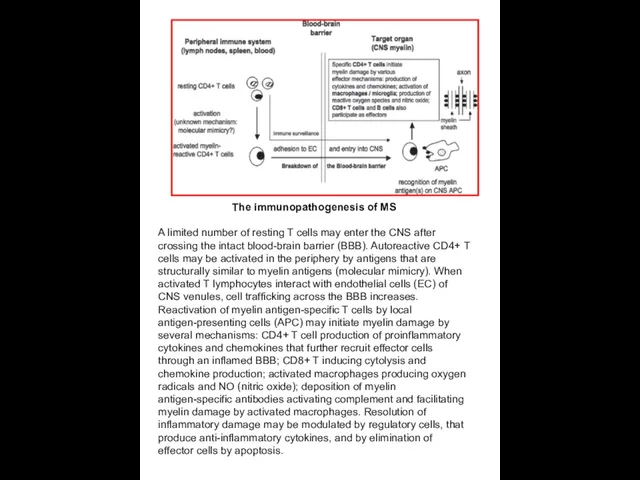
The immunopathogenesis of MS
A limited number of resting T cells may
The immunopathogenesis of MS
A limited number of resting T cells may
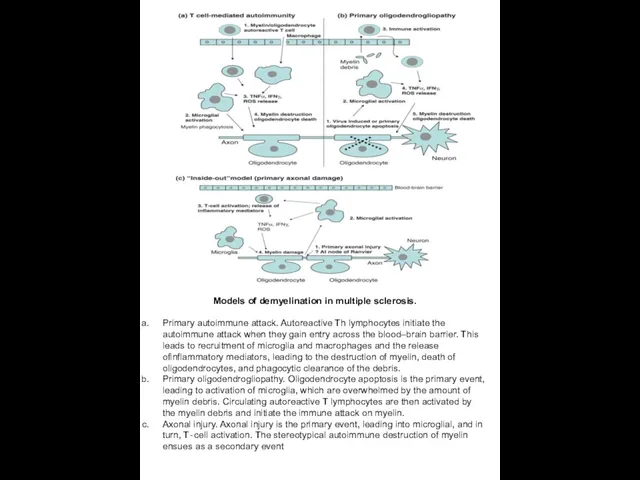
Models of demyelination in multiple sclerosis.
Primary autoimmune attack. Autoreactive Th lymphocytes
Models of demyelination in multiple sclerosis.
Primary autoimmune attack. Autoreactive Th lymphocytes
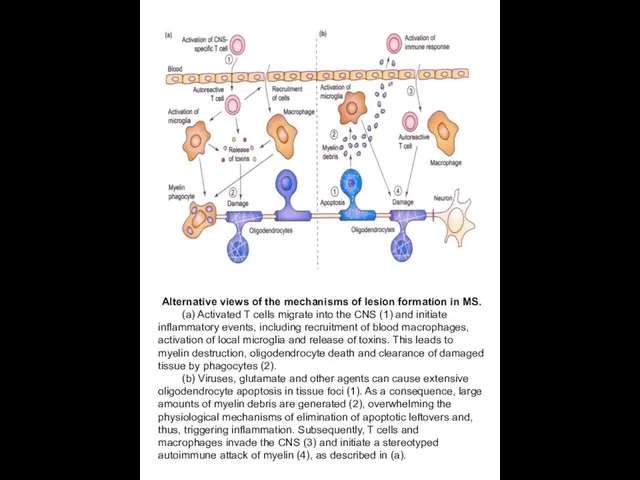
Alternative views of the mechanisms of lesion formation in MS.
(a)
Alternative views of the mechanisms of lesion formation in MS.
(a)
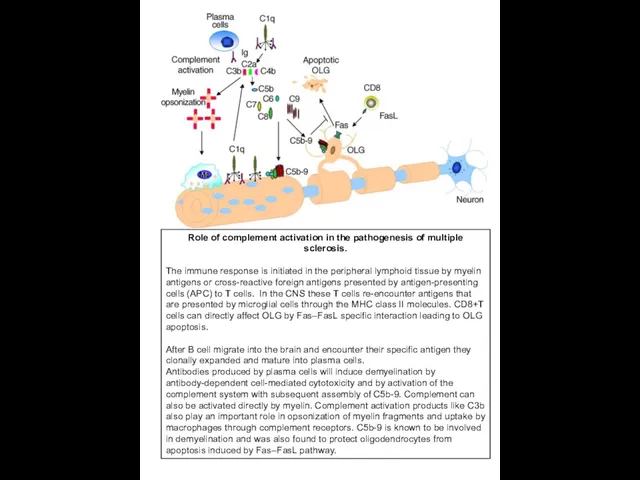
Role of complement activation in the pathogenesis of multiple sclerosis.
The
Role of complement activation in the pathogenesis of multiple sclerosis.
The
Классическими клиническими критериями диагностики рассеянного склероза являются клинические диагностические критерии достоверного
Классическими клиническими критериями диагностики рассеянного склероза являются клинические диагностические критерии достоверного
МРТ в диагностике рассеянного склероза
МРТ — метод диагностики, основанный на том,
МРТ в диагностике рассеянного склероза
МРТ — метод диагностики, основанный на том,

MRI –Т1 ( left ), MWF – Т2 (middle ) and
MRI –Т1 ( left ), MWF – Т2 (middle ) and
Склеротические бляшки в коре мозга при рассеянном
склерозе.
кора
Специфическим, необходимым патоморфологическим маркером РС
Склеротические бляшки в коре мозга при рассеянном
склерозе.
кора
Специфическим, необходимым патоморфологическим маркером РС
In this acute plaque, the central blood vessel is almost obliterated
In this acute plaque, the central blood vessel is almost obliterated
Actively demyelinating MS lesion.
Myelin basic protein (MBP) is a major
Actively demyelinating MS lesion.
Myelin basic protein (MBP) is a major
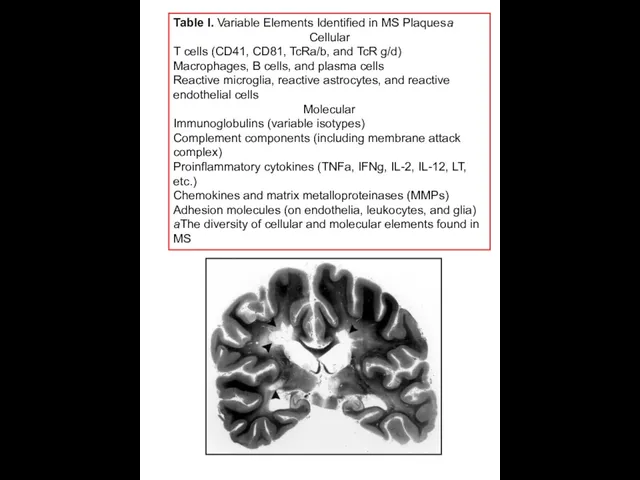
Table I. Variable Elements Identified in MS Plaquesa
Cellular
T cells (CD41, CD81,
Table I. Variable Elements Identified in MS Plaquesa
Cellular
T cells (CD41, CD81,
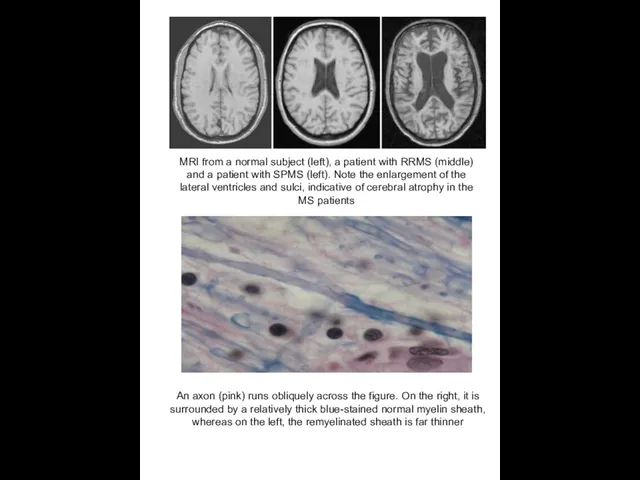
MRI from a normal subject (left), a patient with RRMS (middle)
MRI from a normal subject (left), a patient with RRMS (middle)
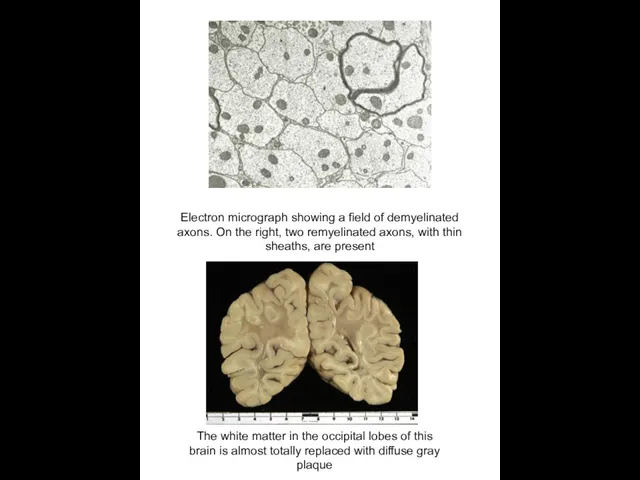
Electron micrograph showing a field of demyelinated axons. On the right,
Electron micrograph showing a field of demyelinated axons. On the right,
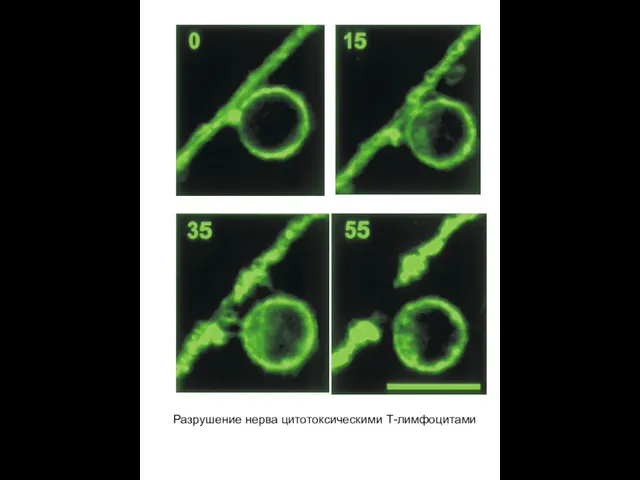
Разрушение нерва цитотоксическими Т-лимфоцитами
Разрушение нерва цитотоксическими Т-лимфоцитами
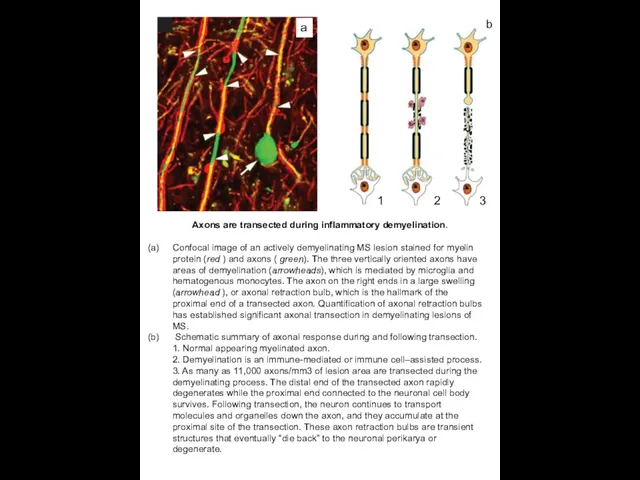
Axons are transected during inflammatory demyelination.
Confocal image of an actively
Axons are transected during inflammatory demyelination.
Confocal image of an actively
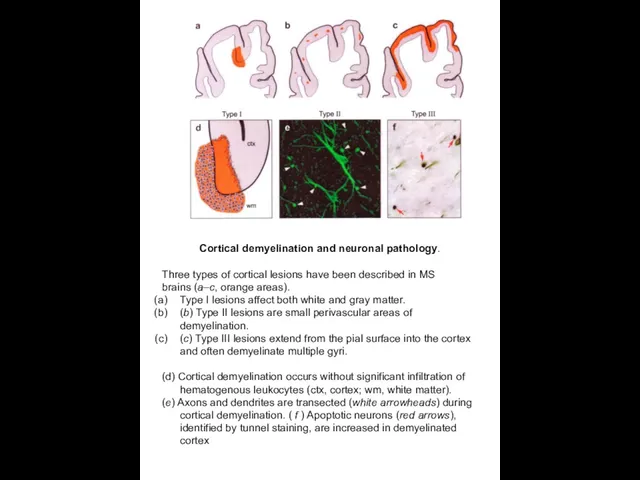
Cortical demyelination and neuronal pathology.
Three types of cortical lesions have
Cortical demyelination and neuronal pathology.
Three types of cortical lesions have
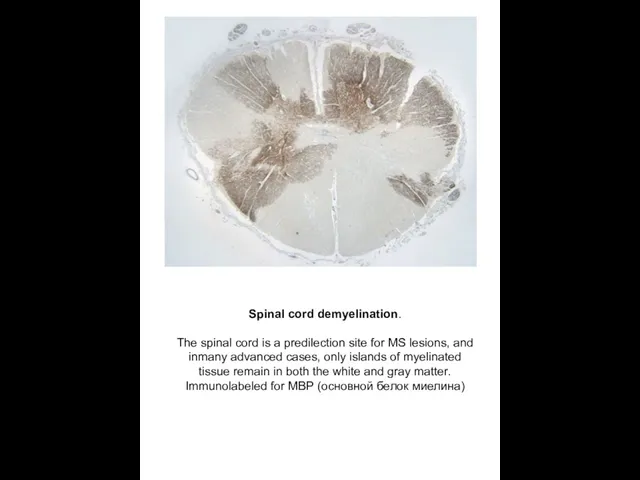
Spinal cord demyelination.
The spinal cord is a predilection site for MS
Spinal cord demyelination.
The spinal cord is a predilection site for MS
Рассеянный склероз: роковая ошибка
иммунной системы
Причиной рассеянного склероза, вероятно, является
Рассеянный склероз: роковая ошибка
иммунной системы
Причиной рассеянного склероза, вероятно, является
SUMMARY POINTS
Multiple sclerosis is an immune-mediated demyelinating disease of the human
SUMMARY POINTS
Multiple sclerosis is an immune-mediated demyelinating disease of the human
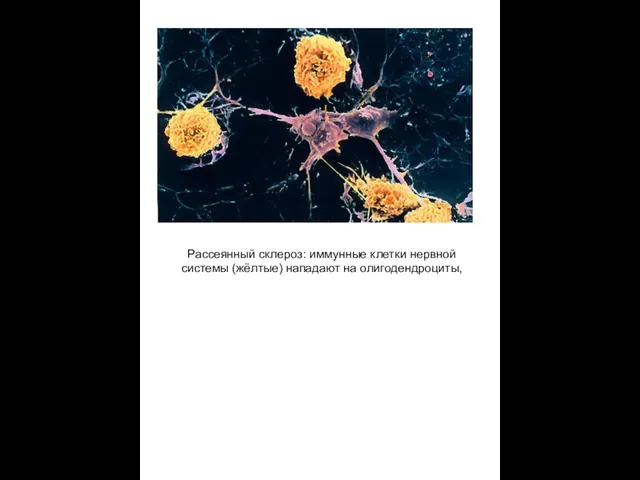
Рассеянный склероз: иммунные клетки нервной системы (жёлтые) нападают на олигодендроциты,
Рассеянный склероз: иммунные клетки нервной системы (жёлтые) нападают на олигодендроциты,
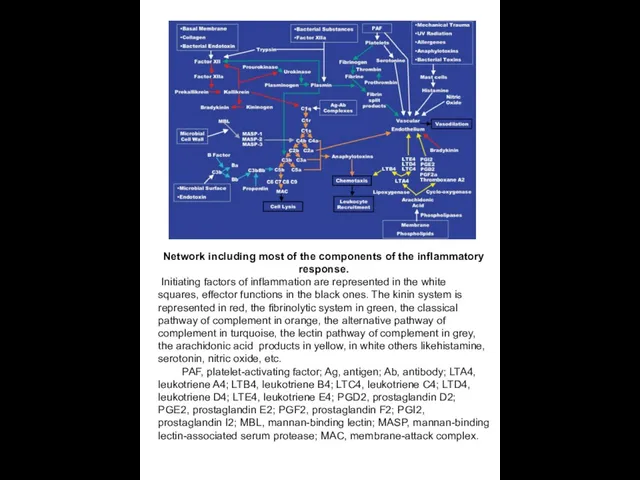
Network including most of the components of the inflammatory response.
Initiating
Network including most of the components of the inflammatory response.
Initiating
Миастения – заболевание нервной и
мышечной систем, проявляющихся слабостью и
повышенной
Миастения – заболевание нервной и
мышечной систем, проявляющихся слабостью и
повышенной
Myasthenia gravis pseudoparalytica
Болезнь Эрба-Гольдфлама
Проявляется обычно в 3 декаде жизни, но может
Myasthenia gravis pseudoparalytica
Болезнь Эрба-Гольдфлама
Проявляется обычно в 3 декаде жизни, но может
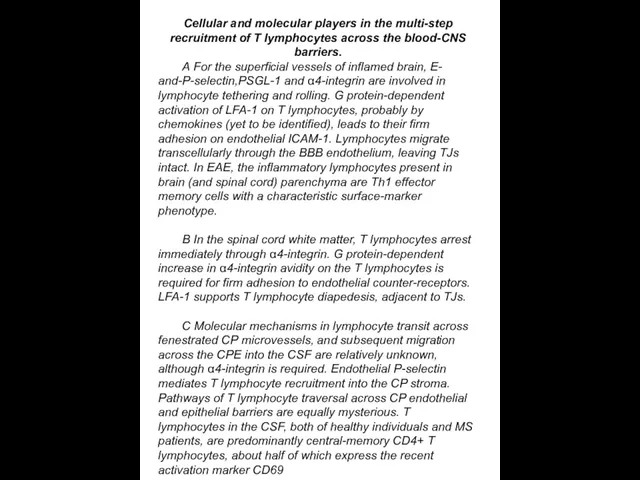
Cellular and molecular players in the multi-step recruitment of T lymphocytes
Cellular and molecular players in the multi-step recruitment of T lymphocytes
Myasthenia gravis pseudoparalytica
Болезнь Эрба-Гольдфлама
Myasthenia gravis pseudoparalytica
Болезнь Эрба-Гольдфлама
Myasthenia gravis initially manifest ptosis.
Myasthenia gravis initially manifest ptosis.
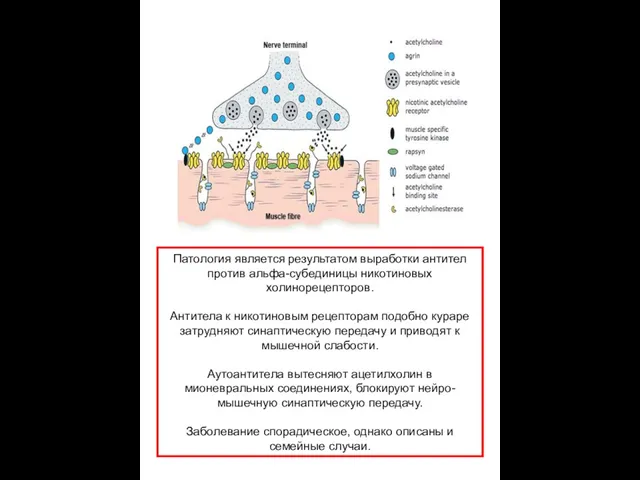
Патология является результатом выработки антител против альфа-субединицы никотиновых холинорецепторов.
Антитела к
Патология является результатом выработки антител против альфа-субединицы никотиновых холинорецепторов.
Антитела к
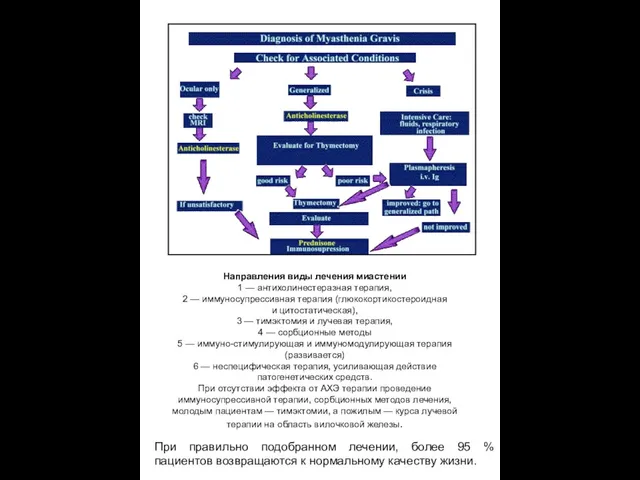
Направления виды лечения миастении
1 — антихолинестеразная терапия,
2 — иммуносупрессивная терапия (глюкокортикостероидная и цитостатическая),
3 — тимэктомия
Направления виды лечения миастении
1 — антихолинестеразная терапия,
2 — иммуносупрессивная терапия (глюкокортикостероидная и цитостатическая),
3 — тимэктомия

Chronically demyelinated axons degenerate owing to loss of myelin trophic support.
Chronically demyelinated axons degenerate owing to loss of myelin trophic support.

A model of MS immunopathogenesis. Myelin-autoreactive T cells are found in
A model of MS immunopathogenesis. Myelin-autoreactive T cells are found in
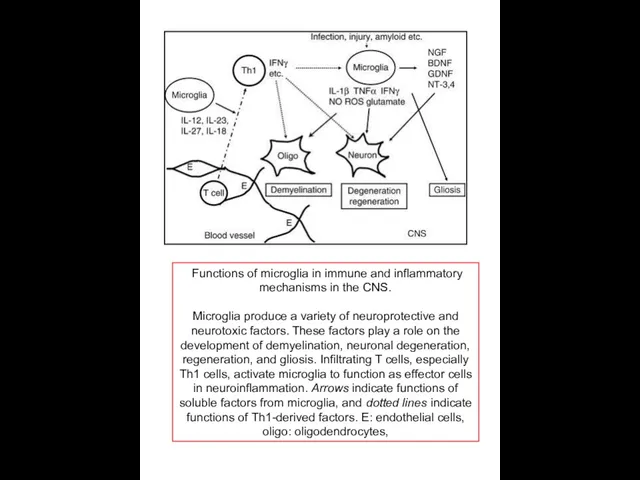
Functions of microglia in immune and inflammatory mechanisms in the CNS.
Microglia
Functions of microglia in immune and inflammatory mechanisms in the CNS.
Microglia
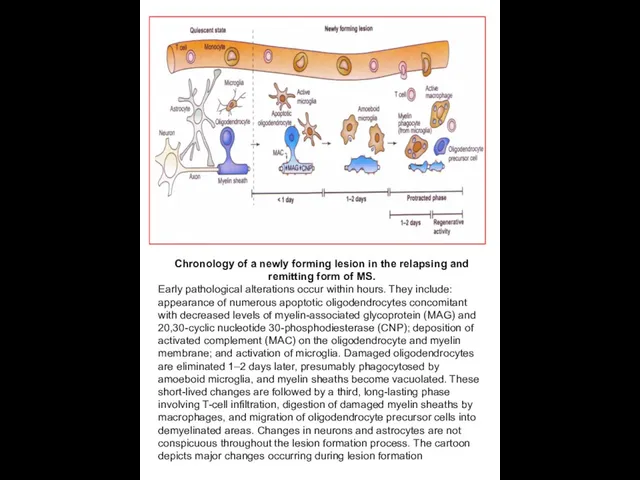
Chronology of a newly forming lesion in the relapsing and remitting
Chronology of a newly forming lesion in the relapsing and remitting
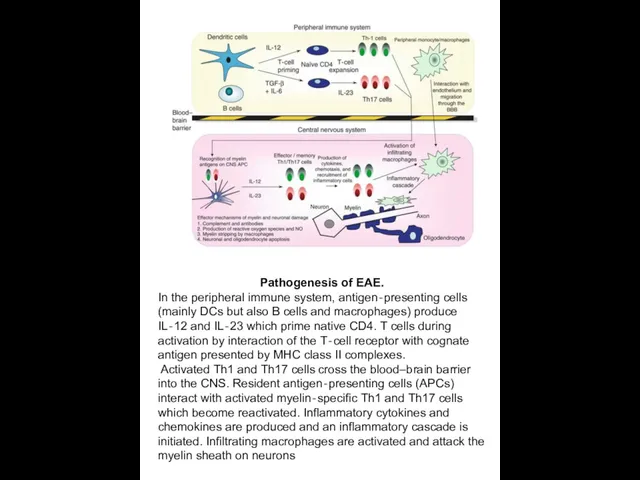
Pathogenesis of EAE.
In the peripheral immune system, antigen‐presenting cells (mainly DCs
Pathogenesis of EAE.
In the peripheral immune system, antigen‐presenting cells (mainly DCs
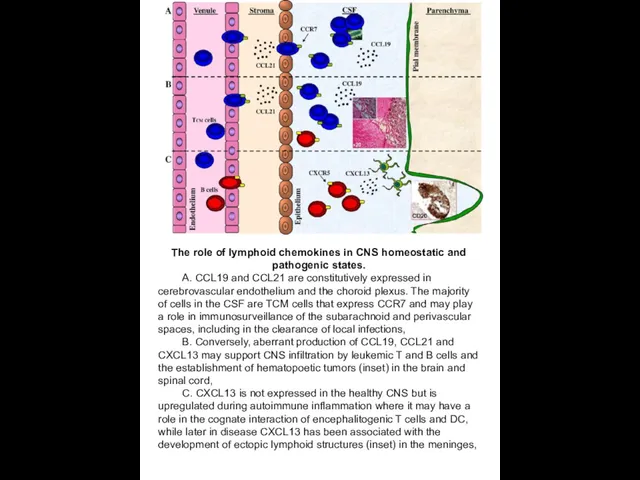
The role of lymphoid chemokines in CNS homeostatic and pathogenic states.
The role of lymphoid chemokines in CNS homeostatic and pathogenic states.
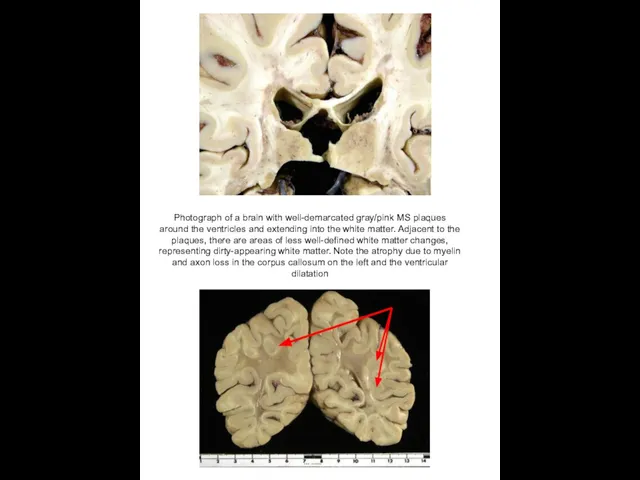
Photograph of a brain with well-demarcated gray/pink MS plaques around the
Photograph of a brain with well-demarcated gray/pink MS plaques around the
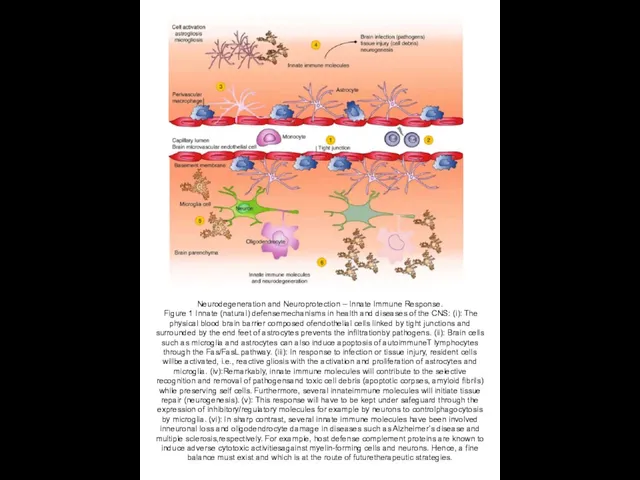
Neurodegeneration and Neuroprotection – Innate Immune Response.
Figure 1 Innate (natural)
Neurodegeneration and Neuroprotection – Innate Immune Response.
Figure 1 Innate (natural)

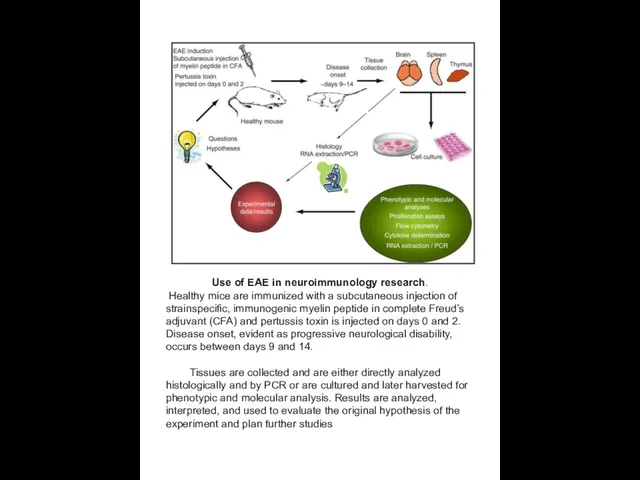
Use of EAE in neuroimmunology research.
Healthy mice are immunized with
Use of EAE in neuroimmunology research.
Healthy mice are immunized with
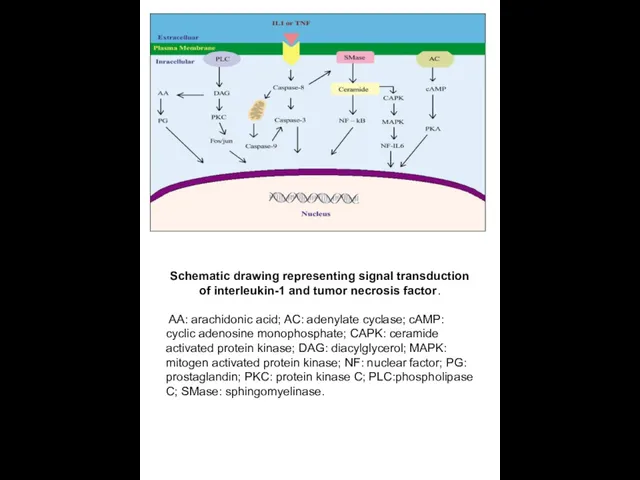
Schematic drawing representing signal transduction of interleukin-1 and tumor necrosis factor.
Schematic drawing representing signal transduction of interleukin-1 and tumor necrosis factor.
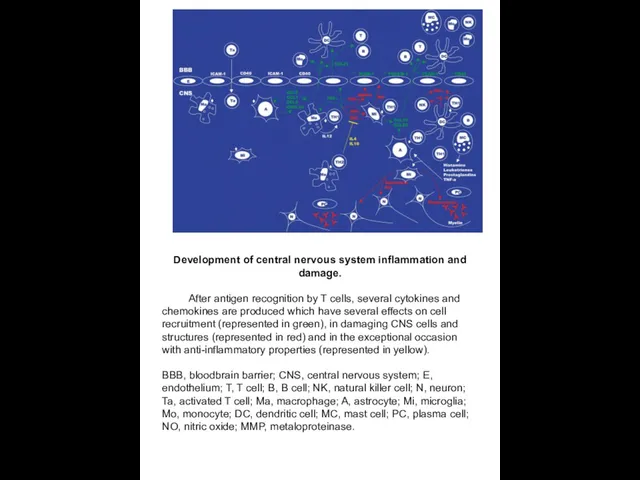
Development of central nervous system inflammation and damage.
After antigen recognition
Development of central nervous system inflammation and damage.
After antigen recognition
 Научное обоснование ограничений жизнедеятельности инвалидов, страдающих офтальмопатологией
Научное обоснование ограничений жизнедеятельности инвалидов, страдающих офтальмопатологией Инфекции мочевыводящих путей. Хронический пиелонефрит у беременных
Инфекции мочевыводящих путей. Хронический пиелонефрит у беременных Biological rhythms and their medical values
Biological rhythms and their medical values ЛФК при переломах позвоночника и костей таза
ЛФК при переломах позвоночника и костей таза Возбудители ОРВИ
Возбудители ОРВИ Микробиология. Метод Циля — Нельсена
Микробиология. Метод Циля — Нельсена Паркинсонизм и болезнь Паркинсона
Паркинсонизм и болезнь Паркинсона Жүктілікті жоспарлау уақытында Фемибион 1 мен фолий қышқылының әсері
Жүктілікті жоспарлау уақытында Фемибион 1 мен фолий қышқылының әсері Комбинированные первичные, врожденные иммунодефициты
Комбинированные первичные, врожденные иммунодефициты Обучение и воспитание детей с тяжелыми нарушениями речи - заикание
Обучение и воспитание детей с тяжелыми нарушениями речи - заикание Ксенобиотики. Классификация и действие ксенобтотиков. Профилактика отравлений
Ксенобиотики. Классификация и действие ксенобтотиков. Профилактика отравлений Жүктілік пен босануды басқару Босанудан кейінгі кезеңді басқару
Жүктілік пен босануды басқару Босанудан кейінгі кезеңді басқару Сестринский уход при инфекционных заболеваниях новорожденных
Сестринский уход при инфекционных заболеваниях новорожденных Операции в области шеи
Операции в области шеи Түркістан қаласындағы салауатты өмір салтын қалыптастыру
Түркістан қаласындағы салауатты өмір салтын қалыптастыру Сестринская помощь при хроническом гастрите
Сестринская помощь при хроническом гастрите Антибиотики. Показания к системной АБТ в стоматологии
Антибиотики. Показания к системной АБТ в стоматологии Трансанальная слизисто-подслизистая резекция по методу Лонго
Трансанальная слизисто-подслизистая резекция по методу Лонго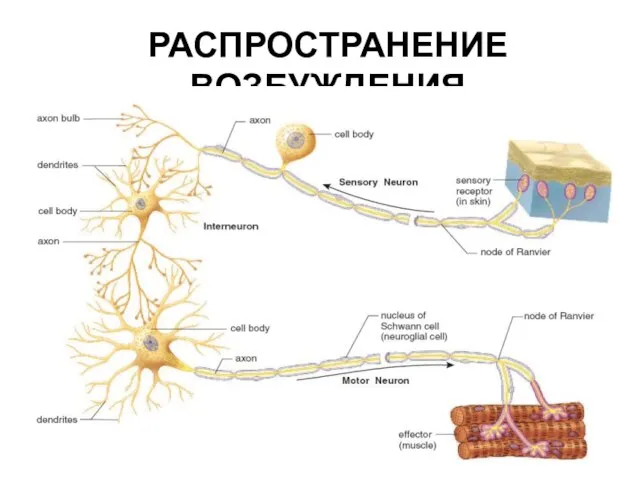 Распространение возбуждения
Распространение возбуждения Организация работы специализированных (БИТ) и линейных бригад скорой помощи
Организация работы специализированных (БИТ) и линейных бригад скорой помощи Особенности развития регионального здравоохранения
Особенности развития регионального здравоохранения Компоненты системы гемостаза
Компоненты системы гемостаза Туберкулез кезіндегі шаралар стандарттары мен алгоритмдері
Туберкулез кезіндегі шаралар стандарттары мен алгоритмдері Гормондар биохимиясы. Гормондар және бейімділік процестер
Гормондар биохимиясы. Гормондар және бейімділік процестер Роговица глаза. Строение роговицы. Заболевания роговицы
Роговица глаза. Строение роговицы. Заболевания роговицы Клиническая фармакология и основы гирудотерапии
Клиническая фармакология и основы гирудотерапии Зудящие дерматозы у детей. Почесуха. Атопический дерматит. Осложнения атопического дерматита. Крапивница. Лекция № 2
Зудящие дерматозы у детей. Почесуха. Атопический дерматит. Осложнения атопического дерматита. Крапивница. Лекция № 2 Общие сведения о ядах и отравлениях (основы судебной токсикологии)
Общие сведения о ядах и отравлениях (основы судебной токсикологии)