- Neurology

Содержание
- 2. Primary Secondary
- 3. TENSION HEADACHES Muscular pain Primary type headache The most common type of headache It can be
- 4. Simptoms dull ache, like a ‘tight pressure feeling’, ‘heavy weight almost daily hours (can last days)
- 5. CLUSTER HEADACHE Diagnosis retro-orbital headache + rhinorrhoea + lacrimation → cluster headache Treatment O2 Triptants Prophylaxis:
- 6. HORNER’S SYNDROME Miosis a persistently small pupil. Denervation of dilatator pupillae m. Ptosis dropping of the
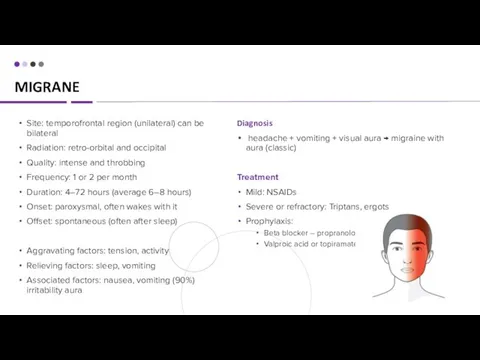
- 7. MIGRANE Diagnosis headache + vomiting + visual aura → migraine with aura (classic) Treatment Mild: NSAIDs
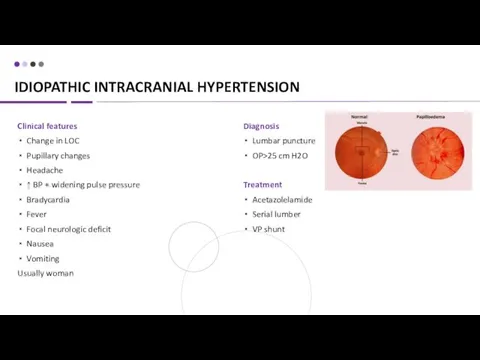
- 8. IDIOPATHIC INTRACRANIAL HYPERTENSION Clinical features Change in LOC Pupillary changes Headache ↑ BP + widening pulse
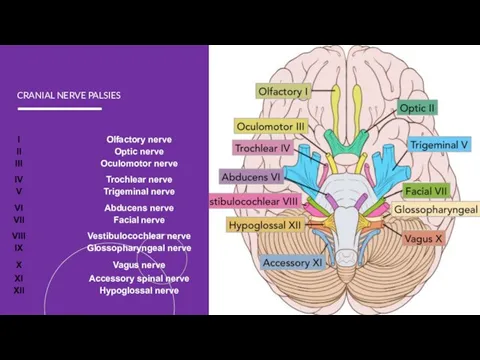
- 9. CRANIAL NERVE PALSIES
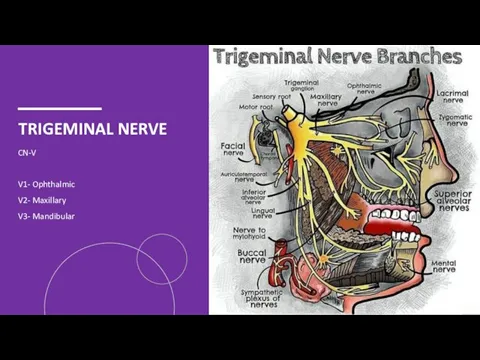
- 10. TRIGEMINAL NERVE CN-V V1- Ophthalmic V2- Maxillary V3- Mandibular
- 11. TRIGEMINAL NEURALGIA Causes Idiopathic or compression of the TN Local pressure on the nerve root entry
- 12. TRIGEMINAL NEURALGIA Treatment Carbamazepine Oxcarbazepine Baclofen Lamotrigine Surgical Diagnosis Clx MRI to rule out secondary causes
- 13. FACIAL NERVE CN – 7 frontal (or temporal) zygomatic buccal marginal mandibular cervical
- 14. BELL’S PALSY Causes infection or inflammation of the facial nerve head trauma head or neck tumor
- 15. BELL’S PALSY Treatment Supportive: Artificial tears if eye is dry and at bedtime Massage and facial
- 16. LUMBAR PUNCTURE Preparing Stop taking blood-thinning medications, such as aspirin and warfarin. Tell your doctor if
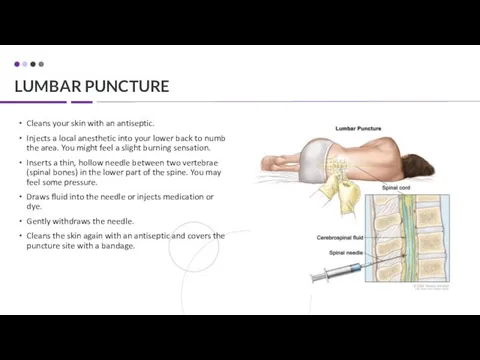
- 17. LUMBAR PUNCTURE Cleans your skin with an antiseptic. Injects a local anesthetic into your lower back
- 19. DISORDERS OF THE VISUAL PATHWAY
- 20. APPROACH TO SYNCOPE
- 21. APPROACH TO SYNCOPE W vasovagal Visceral Baroreceptors Psychogenic Situational and recurrent Drop 50 points in the
- 22. APPROACH TO SYNCOPE Orthostatic hypotension Volume down: dehydration, diarrhea, diaresis and hemorrhage Dysfunctional autonomic nervous system:
- 23. APPROACH TO SYNCOPE Psych Dx: face-palm maneuver Electrolytes Dx: BMP Na, Ca – mental status K,
- 26. Скачать презентацию

Primary
Secondary
Primary
Secondary
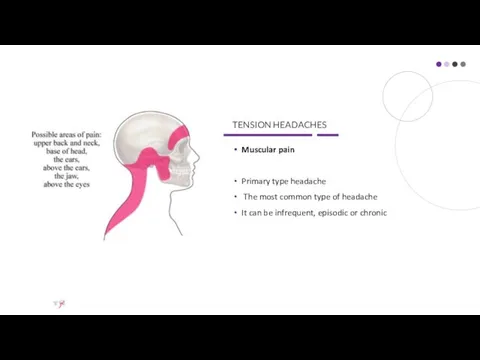
TENSION HEADACHES
Muscular pain
Primary type headache
The most common type of headache
It
TENSION HEADACHES
Muscular pain
Primary type headache
The most common type of headache
It
Simptoms
dull ache, like a ‘tight pressure feeling’, ‘heavy weight
almost daily
hours (can
Simptoms
dull ache, like a ‘tight pressure feeling’, ‘heavy weight
almost daily
hours (can
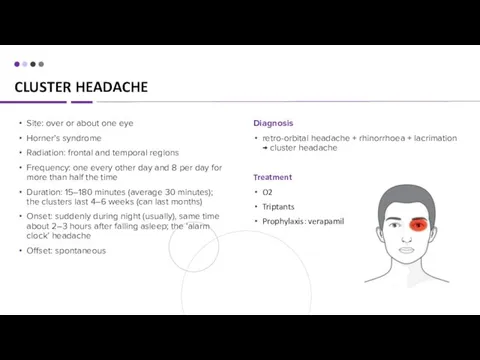
CLUSTER HEADACHE
Diagnosis
retro-orbital headache + rhinorrhoea + lacrimation → cluster headache
Treatment
O2
Triptants
Prophylaxis:
CLUSTER HEADACHE
Diagnosis
retro-orbital headache + rhinorrhoea + lacrimation → cluster headache
Treatment
O2
Triptants
Prophylaxis:
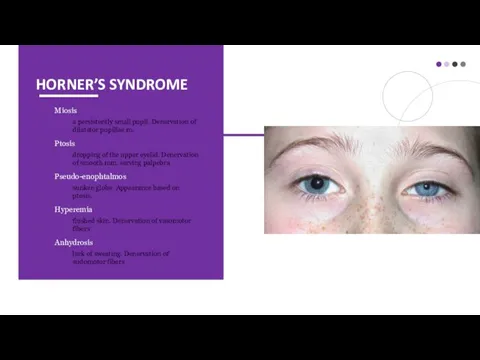
HORNER’S SYNDROME
Miosis
a persistently small pupil. Denervation of dilatator pupillae m.
Ptosis
HORNER’S SYNDROME
Miosis
a persistently small pupil. Denervation of dilatator pupillae m.
Ptosis
MIGRANE
Diagnosis
headache + vomiting + visual aura → migraine with aura
MIGRANE
Diagnosis
headache + vomiting + visual aura → migraine with aura
IDIOPATHIC INTRACRANIAL HYPERTENSION
Clinical features
Change in LOC
Pupillary changes
Headache
↑ BP + widening pulse
IDIOPATHIC INTRACRANIAL HYPERTENSION
Clinical features
Change in LOC
Pupillary changes
Headache
↑ BP + widening pulse
CRANIAL NERVE PALSIES
CRANIAL NERVE PALSIES
TRIGEMINAL NERVE
CN-V
V1- Ophthalmic
V2- Maxillary
V3- Mandibular
TRIGEMINAL NERVE
CN-V
V1- Ophthalmic
V2- Maxillary
V3- Mandibular

TRIGEMINAL NEURALGIA
Causes
Idiopathic or compression of the TN
Local pressure on the nerve
TRIGEMINAL NEURALGIA
Causes
Idiopathic or compression of the TN
Local pressure on the nerve

TRIGEMINAL NEURALGIA
Treatment
Carbamazepine
Oxcarbazepine
Baclofen
Lamotrigine
Surgical
Diagnosis
Clx
MRI to rule out secondary causes
TRIGEMINAL NEURALGIA
Treatment
Carbamazepine
Oxcarbazepine
Baclofen
Lamotrigine
Surgical
Diagnosis
Clx
MRI to rule out secondary causes

FACIAL NERVE
CN – 7
frontal (or temporal)
zygomatic
buccal
marginal mandibular
cervical
FACIAL NERVE
CN – 7
frontal (or temporal)
zygomatic
buccal
marginal mandibular
cervical
BELL’S PALSY
Causes
infection or inflammation of the facial nerve
head trauma
head or neck
BELL’S PALSY
Causes
infection or inflammation of the facial nerve
head trauma
head or neck

BELL’S PALSY
Treatment
Supportive:
Artificial tears if eye is dry and at bedtime
Massage
BELL’S PALSY
Treatment
Supportive:
Artificial tears if eye is dry and at bedtime
Massage

LUMBAR PUNCTURE
Preparing
Stop taking blood-thinning medications, such as aspirin and warfarin.
Tell your
LUMBAR PUNCTURE
Preparing
Stop taking blood-thinning medications, such as aspirin and warfarin.
Tell your
LUMBAR PUNCTURE
Cleans your skin with an antiseptic.
Injects a local anesthetic into
LUMBAR PUNCTURE
Cleans your skin with an antiseptic.
Injects a local anesthetic into


DISORDERS OF THE VISUAL PATHWAY
DISORDERS OF THE VISUAL PATHWAY

APPROACH TO SYNCOPE
APPROACH TO SYNCOPE

APPROACH TO SYNCOPE
W vasovagal
Visceral
Baroreceptors
Psychogenic
Situational and recurrent
Drop 50 points in the SBP
Dx:
APPROACH TO SYNCOPE
W vasovagal
Visceral
Baroreceptors
Psychogenic
Situational and recurrent
Drop 50 points in the SBP
Dx:

APPROACH TO SYNCOPE
Orthostatic hypotension
Volume down: dehydration, diarrhea, diaresis and hemorrhage
Dysfunctional autonomic
APPROACH TO SYNCOPE
Orthostatic hypotension
Volume down: dehydration, diarrhea, diaresis and hemorrhage
Dysfunctional autonomic
APPROACH TO SYNCOPE
Psych
Dx: face-palm maneuver
Electrolytes
Dx: BMP
Na, Ca – mental status
K, Mg
APPROACH TO SYNCOPE
Psych
Dx: face-palm maneuver
Electrolytes
Dx: BMP
Na, Ca – mental status
K, Mg

 Типы высшей нервной деятельности
Типы высшей нервной деятельности Лечебные грязи Крыма
Лечебные грязи Крыма Мероприятия по снижению распространения злокачественных новообразований среди женщин в Свердловской области
Мероприятия по снижению распространения злокачественных новообразований среди женщин в Свердловской области Набор в детский оздоровительный санаторий в г. Евпатория для детей от 10 до 14 лет,
Набор в детский оздоровительный санаторий в г. Евпатория для детей от 10 до 14 лет, № 2 Симптомдық артериальды гипертензия. № 3 вариант: Иценко-Кушинг синдромы кезіндегі
№ 2 Симптомдық артериальды гипертензия. № 3 вариант: Иценко-Кушинг синдромы кезіндегі Нервные и психические болезни
Нервные и психические болезни Оздоровчі системи
Оздоровчі системи Влияние анатомо-физиологических особенностей челюстно-лицевой области на клиническое течение воспалительных заболеваний
Влияние анатомо-физиологических особенностей челюстно-лицевой области на клиническое течение воспалительных заболеваний Клиническая фармакология препаратов, влияющих на функцию пищеварительной системы
Клиническая фармакология препаратов, влияющих на функцию пищеварительной системы Применение лекарственных средств
Применение лекарственных средств Рентгенодиагностика острой пневмонии у детей
Рентгенодиагностика острой пневмонии у детей Гипертоническая болезнь II стадии. Ситуационная задача
Гипертоническая болезнь II стадии. Ситуационная задача Патологическая анатомия ДВС-синдрома
Патологическая анатомия ДВС-синдрома Принципы неотложной помощи при судорожных припадках с потерей сознания
Принципы неотложной помощи при судорожных припадках с потерей сознания Составление проекта нормативной документации на лекарственные формы для парентерального введения
Составление проекта нормативной документации на лекарственные формы для парентерального введения Роль фельдшера в диагностике, лечении и профилактике закрытой черепно-мозговой травмы
Роль фельдшера в диагностике, лечении и профилактике закрытой черепно-мозговой травмы Врожденная косолапость
Врожденная косолапость Тиреотоксикалық криз және тиреотоксикалық кома
Тиреотоксикалық криз және тиреотоксикалық кома Хроническая болезнь почек при сахаром диабете
Хроническая болезнь почек при сахаром диабете Патофизиология обмена веществ
Патофизиология обмена веществ Скарлатина у детей дошкольного возраста
Скарлатина у детей дошкольного возраста Тиреотоксикалық криз және тиреотоксикалық кома
Тиреотоксикалық криз және тиреотоксикалық кома Пищевые токсикоинфекции
Пищевые токсикоинфекции Характер человека
Характер человека Поведенческие особенности и социализация в младенчестве
Поведенческие особенности и социализация в младенчестве Здоровый образ жизни – залог успешности специалиста
Здоровый образ жизни – залог успешности специалиста Духовные и физические аспекты эпилепсии
Духовные и физические аспекты эпилепсии Возрастная физиология (физиологические особенности детей и подростков)
Возрастная физиология (физиологические особенности детей и подростков)